The step of canal shaping in the endodontic treatment holds an important place as it influences the following phases of canal irrigation, obturation, and the overall success of the treatment itself [1]. The achievement of this “ideal” preparation is a cumbersome task in curved root canals. The curvature of the canal is considered to be the preeminent risk factor for procedural errors enlisting ledging, zipping and transportation [2–4]. Cimis et al., stated that 46% of curved canals have varying degrees of apical transportation subsequent to instrumentation [5]. Transportation occurs due to the tendency of endodontic instruments to straighten the root canal during the chemo-mechanical preparation [3,4]. The structural durability of the tooth following endodontic therapy is directly proportional to the remaining dentin thickness. The aggressive instrumentation of the root canal structure results in loss of dentin which may eventually weaken the tooth [6]. Bender and Freeland stated that the maximum percentage of vertical root fractures occur following root canal therapy [7].
The incorporation of nickel-titanium (NiTi) rotary files has drastically enhanced the quality of canal shaping [8]. Recently proposed single-file shaping technique simplifies the instrumentation protocol while reducing the risk of instrument failure and cross contamination [9]. The two different concepts of single-file systems are continuous rotation and reciprocation or discontinuous rotation. Wave One and One Shape represent these single file systems that have different instrument designs and metallurgy. OneShape (Micro Mega, Besancon, France) is to be used in full continuous rotation whereas Wave one (Dentsply Maillefer, Ballaigues, Switzerland) is used in a reciprocal motion. Hence, the purpose of this study was to access the effect of these new NiTi rotary instruments on canal transportation and the canal centering ability and compare it with one well-assessed full-sequence rotary NiTi system. CBCT scanning was used because it provides a three-dimensional reproduction of the tooth, allowing better evaluation of shaping ability without the destruction of the specimen [10–12].
Materials and Methods
Specimen Selection
Canal transportation and centering ability were evaluated using a comparative study design, conducted in the Department of Conservative Dentistry and Endodontics, Sri Aurobindo College of Dentistry. The study period was four months. A total of 60 extracted mandibular first molars were selected, disinfected and stored in saline at 4°C until use. Coronal access was achieved using the Endo-Access bur (Dentsply, Maillefer) and exploration with size 10 K file was done to confirm the patency and presence of two separate mesial canals. The inclusion criteria included teeth completely formed apices and mesiobuccal canal curvature between 20° and 35° assessed according to Schneider’s technique [13]. The teeth with calcifications, canal curvatures greater than 35° and anatomic abnormalities were excluded based on buccolingual and mesiodistal radiographic images. Teeth with restorations or caries invading the pulp or extending onto the root surface were also excluded from the study sample.
All teeth were shortened to a length of 18 mm using a diamond cutting disk and were randomly divided into 3 groups of 20 teeth each according to the instrumentation method applied.
Only the mesiobuccal canals were taken up for instrumentation. The working length of each canal was determined by subtracting 1 mm from the observed length of protrusion of a number 10 K file through the apical foramen. Subsequently, a glide path was formed by using#15 K-file.
Scanning procedure
For each tooth, apical 3 mm of the distal root was separated. Teeth were embedded into auto polymerizing transparent acrylic resin using silicon mould 5cm x 5cm. Small pieces of orthodontic wire were inserted parallel to long axis of the tooth close to the MB line angle for adjustment of scan orientation. Each mounting was horizontally fitted to a chin support with its occlusal plane parallel to the plate. This was done to ensure standardization of the specimens for the tomography images before and after root canal instrumentation.
All teeth were scanned by using the CBCT system (CS 9000 3D, Carestream). The images were captured in a small field of view (6 cm) at 90 kVp and 5mA with a 90μm voxel size to determine the root canal shape before instrumentation. Three tomograms were selected for each assessed specimen. The first corresponded to the area located 3 mm (apical third), the second 6 mm (middle third) and the third 9 mm (cervical third) from the root apex.
Root canal preparation
Group 1: ProTaper (PT)
Mesiobuccal canal instrumentation was accomplished using continuous rotation following the sequence of ProTaper S1->SX->S1->S2->F1->F2 with the X-Smart Plus motor.
Group 2: One Shape (OS)
Each canal was shaped using OneShape rotary file till the working length with the X-Smart Plus motor set to 350 rpm and a 5-Ncm torque with a 16:1 contra-angle.
Group 3: Wave One (WO)
Canals were shaped with Wave One Primary reciprocating files using a pecking motion till working length. The reciprocating motor X-Smart Plus (Dentsply Maillefer) was used.
Chelating agent, RCPrep (Premier Dental Products, Norristown, PA) was used as lubricant in all canal preparations, and canal irrigation was performed with 1ml of 3.0% NaOCl after the use of each file. One set of instruments was used for the preparation of 4 canals in the Protaper group and each Wave One and One Shape file was used to enlarge 4 canals only. The flutes of the instrument were cleaned after three in-and-out-movements (pecks) using NaOCl soaked sponge. After every insertion the files were examined for any deformation or fracture.
Determination of Preparation Time
The mean working time was recorded using an electronic stopwatch and included active instrumentation time, instrument changes, irrigation and instrument cleaning.
Post Instrumentation Scan
The instrumented canals were scanned with CBCT using the same protocol and parameter settings. All CBCT images were assessed utilizing the ON demand software for CS 9000 3D, Care stream Dental CBCT system.
Assessment of Root Canal Preparation
The shortest distance from the edge of the mesiobuccal canal to the periphery of the root (mesial and distal) was measured on the reconstructed cross-sectional images of the pre and post-instrumentation scans by using the measure length tool [Table/Fig-1].
Representative image of tooth sections showing how transportation and centering ratios were derived
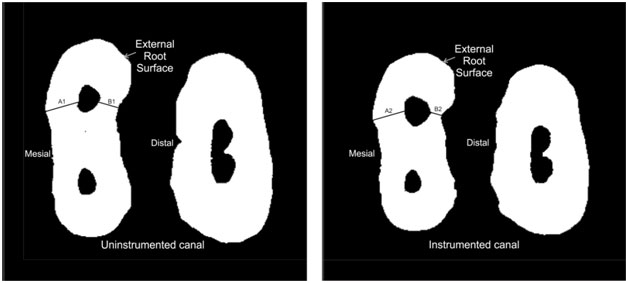
(1) The degree of transportation was calculated according to the formula given by Gambill et al., [14]:
(A1–A2)–(B1–B2)
Where, A1: is the shortest distance from the mesial edge of the root to the mesial edge of the uninstrumented canal.
A2: is the shortest distance from the mesial edge of the root to the mesial edge of the instrumented canal.
B1: is the shortest distance from the distal edge of the root to the distal edge of the uninstrumented canal.
B2: is the shortest distance from the distal edge of the root to the distal edge of the instrumented canal.
A result other than 0 obtained from the above formula indicates that canal transportation has occurred; with the absolute value of result obtained determining the degree of transportation. The total value indicates the tendency of the transportation direction. A positive value represents that transportation has occurred lateral to the curvature, whereas the negative value represents that transportation has occurred in the direction facing the furcation [3,14].
(2) The canal centering ratio at each level according to the following ratio:
(A1–A2) / (B1–B2) or (B1–B2) / (A1–A2)
The formula was chosen in such a manner that the lowest of the results obtained through the difference should always be the numerator. A result of 1 (one) indicated perfect centralization capacity and the closer the result to zero the worse the ability of the instrument to keep itself in the canal central axis.
Endodontic instrumentation was completed by a single experienced operator while the assessment of the cone beam computed tomography scans before and after instrumentation were carried out by a second examiner who was blind in respect of all experimental groups.
Statistical Analysis
One-way analysis of variance (ANOVA) with Tukey’s honestly significant difference (HSD) was applied to make inter-group comparison of canal transportation, canal centering ability, and the time taken for preparation using Minitab version 5.0. A p <0.05 was considered as the statistically significant level.
Results
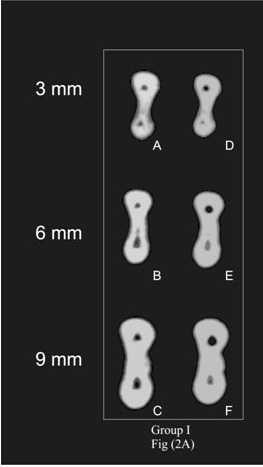
[Table/Fig-2a,b,c] shows representative pre- and post instrumentation CBCT scans at selected levels 3mm, 6mm and 9mm from the apex. The mean and standard deviation values for canal transportation and the centering ratio after instrumentation are presented in [Table/Fig-3,4]. The Tukey’s post hoc test revealed that there were no differences in the amount of transportation between the rotary instruments (p > .05) at 3mm and 6mm from the apex. At 9 mm from the apex, Group I PT showed significantly higher mean canal transportation and lower centering ability (0.19±0.08 and 0.39±0.16), as compared to OS (0.12±0.07 and 0.54±0.24) andWO (0.13±0.06 and 0.55±0.18) while the differences between OS and WO were not statistically significant.
Representative CBCT scans before (A–C) and after (D–F) instrumentation Group I rotary full-sequence technique PT at 3 mm (A and D), 6 mm (B and E) and 9 mm (C and F) level from the apical foramen
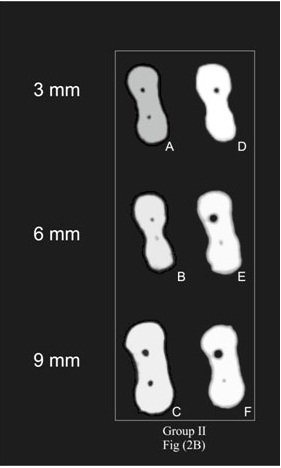
Representative CBCT scans before (A–C) and after (D–F) instrumentation Group II reciprocating single-file technique WO at 3 mm (A and D), 6 mm (B and E) and 9 mm (C and F) level from the apical foramen
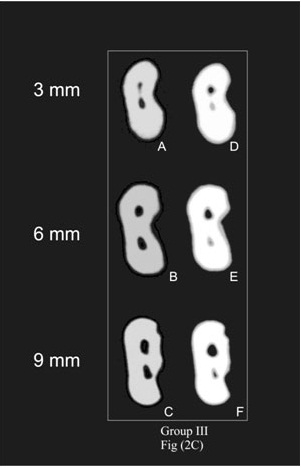
Representative CBCT scans before (A–C) and after (D–F) instrumentation Group III rotary single file technique OS at 3 mm (A and D), 6 mm (B and E) and 9 mm (C and F) level from the apical foramen
(Mean (±SD)) and statistical analysis of mean canal transportation values for the tested groups (n=20)
| Groups | 3mm | 6mm | 9mm |
|---|
| I - PT | 0.05600 (±0.03515) a | 0.08500 (±0.04662) a | 0.18650 (±0.07604) b |
| II – OS | 0.04600 (±0.03251) a | 0.06750 (±0.03596) a | 0.11750 (±0.07276) a |
| III - WO | 0.05750 (±0.03582) a | 0.07500(± 0.04310) a | 0.13000 (± 0.06164) a |
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One
(Mean (±SD)) and statistical analysis of mean canal centering ratio values for the tested groups (n=20)
| Groups | 3mm | 6mm | 9mm |
|---|
| I - PT | 0.6310 (±0.1964) a | 0.5705 (±0.2135) a | 0.3890 (±0.1556) b |
| II – OS | 0.6685 (±0.2439) a | 0.5480 (±0.2451) a | 0.5425 (±0.2447) a |
| III – WO | 0.6445 (±0.2305) a | 0.5705 (±0.2371) a | 0.5515 (±0.1842) a |
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One
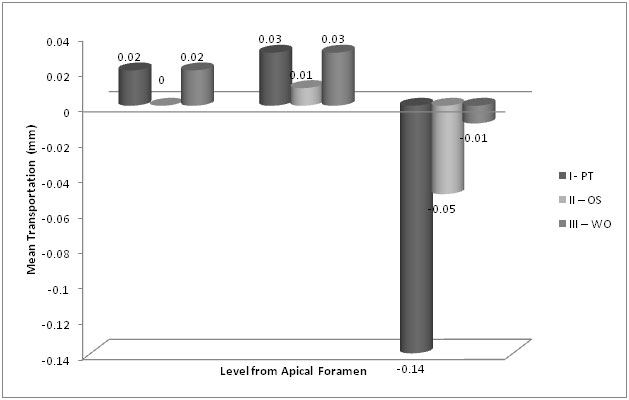
The directions of transportation in each level of experimental groups are shown in [Table/Fig-5]. At 3-mm level both PT and WO groups showed transportation towards the lateral aspect of the curvature while the samples in OS group remained centered. At the 6-mm level all the groups exhibited transportation towards the outer aspect of the curvature. At the 9-mm from the apex level, the canal samples in all the experimental groups showed the same furcation directed transportation tendency.
Transportation tendencies of groups in each section (negative value indicates the transportation tendency toward the furcal aspect of the curvature)
The time taken for preparation is presented in [Table/Fig-6]. PT showed significantly higher mean preparation time (106.00 ± 11.09) as compared to the other groups, while the differences between OS (57.05 ± 3.73) and WO (60.15 ± 4.98) were not significant (p<0.05).
(Mean (±SD)) and statistical analysis of mean values for the time taken for preparation (seconds) for the tested groups (n=20)
| Groups | Mean (±SD) |
|---|
| I - PT | 106.00 (± 11.09) b |
| II – OS | 57.05 (±3.73) a |
| III – WO | 60.15 (±4.98) a |
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One
Discussion
The anatomy and morphology of the root canal system promulgates other challenges necessary for achieving ideal cleaning and shaping. Schneider emphasized that a tapering funnel shape along with the smallest diameter at the apical end is considered to be the most appropriate canal shape for irrigation and filling with gutta-percha. Attaining this ideal flare is a problematic task in narrow curved canals [11].
Since their introduction, in the early 1960’s numerous NiTi rotary systems have been added to the arsenal of endodontic instruments. Single file (NiTi) rotary systems are gaining clinical acceptance as they reduce the time required for biomechanical preparation, as well as reduce the number of failures related to instrumentation [15]. The single file systems can be used either in a reciprocal motion (Wave One, Dentsply Maillefer) or in continuous rotation (OneShape, MicroMega).
The reciprocating working motion consists of an unequal counterclockwise and clockwise motion. The greater angle of the counterclockwise rotation ensures apical advancement of the file while the clockwise motion disengages the file. The reciprocating action acts to reduce the problem of taper lock by continually reversing the direction of rotation and minimizes torsional and flexural stresses on the instrument [15,16]. One-Shape instruments have different cross-sectional designs and variable pitch length along the working part. This design helps to eliminate threading and binding of the instrument in continuous rotation [17]. Though there is literature on the reduction of fatigue and extended life span of the instrument but there is requirement of investigations regarding canal shaping ability of single file systems. These are necessary because fast approaches toward the apex with fewer instruments and sharp cutting edges produces aberrations [18,19].
The Glossary of Endodontic Terms of the American Association of Endodontists defines transportation as ‘the removal of canal wall structure on the outside curve in the apical half of the canal due to the tendency of files to restore themselves to their original linear shape during canal preparation’ [20]. Wu et al., stated that apical transportation of more than 300 μm has the capability of negatively affecting the sealing of the obturation [21].
In this study we evaluated three files system including Protaper, WaveOne and OneShape in extracted mandibular first molars with curvature of 20° to 35°. The mesiobuccal root canals of mandibular molars normally have an accentuated curvature, so they were selected for this study [22]. CBCT examination of the preoperative and postoperative images of the cross-section of root canal facilitates the evaluation of the significant parameters of root canal preparation, namely centering ability and canal transportation [23]. CBCT analysis has been found to be one of the most accurate method for assessing the centering ability of different rotary systems [11,24].
The degree of canal transportation at each level i.e. 3 mm, 6 mm and 9 mm from the apex was calculated according to the formula given by Gambill et al., [18].
When comparing the transportation at each level of cross-sectional images, both single-file systems i.e. reciprocating motion as well as continuous rotation did not show any significant differences (p > .05). At the level of 9 mm, Group I i.e. Protaper showed significantly higher mean canal transportation and lower centering ability as compared to Group II and Group III. In a study conducted by Maitin et al canals prepared with ProTaper had more canal transportation at all the investigated levels of root canal (coronal, middle, and apical third) as compared to instrumentation with Mtwo and RaCe systems. The increased transportation with ProTaper could be due to its reduced flexibility, increased tip stiffness and progressive taper design of the instrument [12].
However, McRay et al., in a study based on microCT imaging reported no statistically significant difference in the canal centaring ability of WaveOne and ProTaper systems. This could be attributed to the difference in specimen preparation wherein coronal pre-flaring with SX was not carried out [25].
At 3-mm level it was observed that both Protaper and WaveOne groups had akin tendencies of transportation toward lateral aspect of the canal curvature while the samples in One Shape group remained centered, thus concluding that though there was no statistical significance, at the level of 3 mm One Shape showed better results. At the 6-mm level all the groups exhibited transportation towards the outer aspect of the curvature. At the 9-mm from the apex level, the canal samples in all the experimental groups showed the same furcation directed transportation tendency. However, transportation towards inner aspect of curvature at 9 mm level from apex i.e. close to the furcation area was least with the Wave One group. Inner aspect of curvature is considered as the danger zone in mandibular molars [26].
Abou-Rass, Frank, Glick first described the danger zone of the mandibular molars and established its importance during cleaning and shaping procedures [27]. Sinai observed that aggressive instrumentation in the cervical third of the root canal can lead to strip perforations and inflammatory complications [28]. Less transportation towards this area can be considered a favourable feature for the Wave One system.
The inclination of transportation and values observed are in accordance with those of previous studies, even though the evaluation method used was dissimilar. Goldberg et al., evaluated the centering ability of WaveOne in curved canals and observed excellent results with low apical transportation without any blockage or separation [29].
In the study conducted by Tambe et al., the canal transportation after instrumentation with One Shape rotary file and primary Wave One reciprocating file and Protaper system was compared, and it was concluded that Wave One system showed less canal transportation and better centering ability as compared with other systems tested [30]. The difference in the result obtained could be due to enlargement of canal up to size 20 with hand files prior to Wave One instrumentation. In an earlier study comparing the canal shaping efficacy of Wave One and Reciproc it was concluded that the Wave One file exhibited better maintenance of canal anatomy following establishment of a glide-path larger than #15 [31].
None of the instruments fractured but there was macroscopic deformation of One Shape file after use. The technique, numbers of instruments used and the operator experience influence the time taken for root canal preparation [32]. The comparison of time taken for canal preparation was based on total time for active instrumentation as well as time for instrument changes, cleaning the instrument flutes and irrigation. One Shape and Wave One were significantly faster than the full sequence Protaper instruments (p <0.05), they reduced preparation time by up to 46.2 % and 43.4 % respectively. Though reduced chair side time is beneficial the time available for chemical disinfection of the root canal system is also simultaneously reduced. To compensate the decreased irrigation time, utilization of larger volumes of irrigant and activation of the irrigants has been advised to improve chemical dissolution of residual debris [15].
Further it has been shown that rotary files can produce various degrees of radicular dentinal defects such as craze lines or incomplete cracks [33,34]. There is possibility of increased stress generation when only one instrument is used for complete preparation. Further investigations are required to assess the cleaning effectiveness and incidence of dentinal defects with the use of new single-file systems.
Conclusion
Although none of the instruments evaluated in this study were totally effective in performing biomechanical preparation of the root canals, single file systems demonstrated average canal transportation and centering ability comparable to full sequence Protaper system in curved root canals. This indicates safety in the preparation of root canals with these new single-file systems.
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One
Comparisons between groups apply to each column. Means with same lower case letter are not statistically different at p = 0.05 (ANOVA and Tukey HSD). PT – Protaper, OS – One Shape, WO – Wave One