Solitary Extragnathic Langerhans Cell Histiocytosis – A Rare Case
Vankayala Yashoda1, Eppalapally Sharath Kumar Reddy2, Sangala Naga Bhavani3, Krishna A4, Mane Srinivas Muni Sekhar5
1 Post Graduate, Department of Oral and Maxillofacial Pathology, SVS Institute of Dental Sciences, Telangana, India.
2 Post Graduate, Department of Oral and Maxillofacial Pathology, SVS Institute of Dental Sciences, Telangana, India.
3 Reader, Department of Oral and Maxillofacial Pathology, SVS Institute of Dental Sciences, Telangana, India.
4 Assistant Professor, Department of Oral and Maxillofacial Pathology, College of Dentistry, Al Jouf University Sakaka, Al Jouf, Kingdom of Soudi Arabia.
5 Professor and Head, Department of Oral and Maxillofacial Pathology, SVS institute of Dental Sciences, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vankayala Yashoda, Post Graduate, Department of Oral and Maxillofacial Pathology, SVS institute of Dental Sciences, Appanapally, Mahbubnagar, Telangana-509002, India. E-mail : dryashu5@gmail.com
Langerhans cell histiocytosis (LCH), mainly affects the skull, vertebrae, ribs and mandible in children and the long bones of adults. Symptoms range from none to pain, swelling and tenderness over the site of the lesion. This disease presents oral manifestations which can sometimes be the first expression of the condition. It occurs in three forms namely eosinophilic granuloma in which isolated or multiple bones are involved, But has a good prognosis whereas other variants Hand-Shuller-Christian disease (chronic dessiminated variant) and Letterer-Siwe disease (acute dessiminated form) have poor prognosis. Occasionally only soft tissues are affected without bony involvement. Males are more commonly affected than females. This article describes a rare variant of eosinophilic granuloma of labial mucosa without bony involvement.
Birbeck granules, Eosinophilic granuloma, Histiocytes, Langerhans cells, Ulcer
Case Report
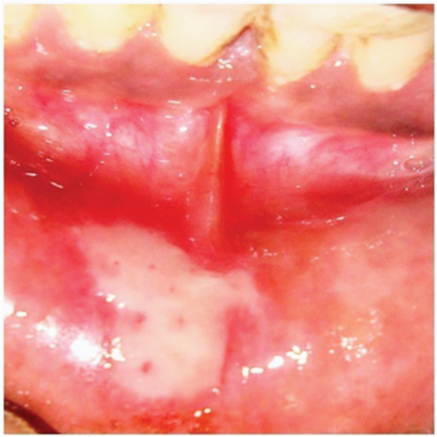
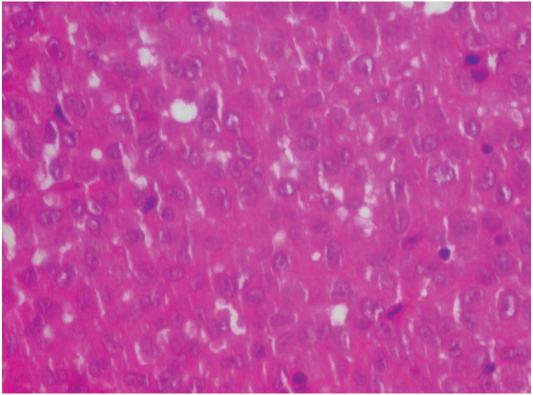
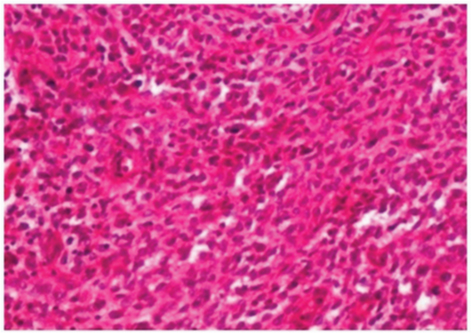
A 50-year-old male patient reported to the Department of Oral Medicine and Radiology of SVS Institute of Dental Sciences, Mahbubnagar with a chief complaint of painful ulcer in the labial sulcus of mandible with a duration of two months. On examination, the ulcer was measuring about 0.8x1 cm approximately. The floor of ulcer was granulomatous with irregular margins and undermined edges [Table/Fig-1]. No other abnormality was detected on general and oral examination. Clinically, the patient was otherwise normal. Incisional biopsy was done and the specimen was sent to our department. H & E stained sections revealed an admixture of cell population comprising of histiocytes containing abundant eosinophilic cytoplasm and eosinophils with bilobed, spectacle shaped nuclei. Cells with relatively pale cytoplasm containing vesicular nuclei with indentations imparting coffee-bean shaped appearance were also seen which are presumably Langerhans cells [Table/Fig-2]. This group of cells comprised a majority of cell population along with plasma cells and lymphocytes. Numerous blood vessels lined by plump endothelial cells and extravasated RBCs were also noted. The intervening delicate connective tissue showed haphazardly arranged collagen fibers with few fibroblasts and fibrocytes [Table/Fig-3,4,5]. Keeping in view the above findings, a diagnosis of eosinophilic granuloma was given. Subsequently, cephalograms and other radiographs were advised which did not reveal any skeletal involvement nor CT scan of the body revealed any involvement of systemic organs. In view of all the above findings, a final diagnosis of solitary extragnathic Langerhans cell histiocytosis was arrived at and the patient was referred to Department of Oral and Maxillofacial Surgery for surgical excision.
Granulomatous ulcer in labial sulcus
Sheets of Langerhans cells with coffee bean shaped nucleus (40x)
Sheets of inflammatory cells with predominantly delicate CT background (10x)
Admixture of cell population comprising à Histiocytes + Eosinophils (20x)
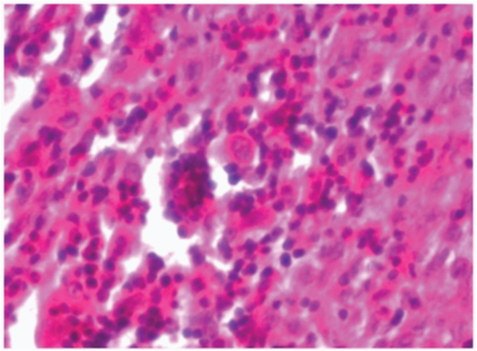
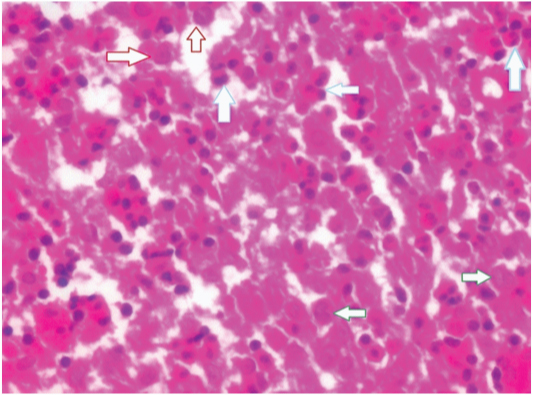
In addition to chronic inflammatory cell population à Cells with relatively pale cytoplasm containing vesicular nuclei with indentations imparting “coffee-bean” shaped appearance à Langerhans’ cells (green arrow), histiocytes (red arrow), eosinophils (blue arrow) (40x)
Discussion
Langerhans cell histiocytosis (LCH) is a group of disorders containing three clinical variants: eosinophilic granuloma, Hand-Shuller-Christian disease and Letterer-Siwe disease [1]. Though the latter two are more generalized and serious forms, eosinophilic granuloma is localized form of LCH generally presenting as a monostotic lesion affecting any of the flat or long bones [2]. Soft tissue involvement might occur affecting mainly the lymph nodes, lungs and mucous membranes subsequently. However, on rare occasions, only soft tissue involvement mostly presenting as palatal or gingival ulcerations without the involvement of underlying bone have been reported [3,4]. To the best of our knowledge, only six cases have been reported where they presented as ulceration in the soft tissues overlying bone [5]. But the present case is quite different from those reported and is probably the first of its kind where it has occurred in the lip, a soft tissue that has no bone within it. Secondly, 90% of cases reported are in children below the age of 10 years [2] and in the present case, the patient is an elderly individual in the sixth decade.
Clinically, a variety of lesions may present as an ulcer. But careful biopsy and histological examination may help us in their accurate diagnosis. In the present case histologically it was observed that there was an inflammatory process with presence of abundant proliferation of eosinophils, histiocytes and Langerhans cells. On extensive search of literature for lesions containing eosinophils and histiocytes, a variety of lesions such as eosinophilic ulcer of oral mucosa, atypical histiocytic granuloma (AHG), angiolymphoid hyperplasia with eosinophilia (ALHE), Kimura disease and LCH particularly eosinophilic granuloma were considered [6,7].
The presence of Langerhans cells with characteristic cleaved or coffee bean shaped nuclei is hallmark of LCH which was evident in our case. However, positivity with CD1a and S100 protein would have helped in confirming the diagnosis [8,9]. However, no such definitive diagnosis could be arrived at due to inadequacy of the tissue and the patient’s refusal for further investigations, a detailed follow up could not be carried out.
In our case, a diagnosis of eosinophilic granuloma was made at by excluding Hand-Schuller-Christian disease which shows a classical triad of punched out bone destructions in skull, uni/bilateral exophthalmos and diabetes insipidus with or without manifestations of dyspituaitarism such as polyurea, dwarfism/infantilism . Letterer-Siwe disease was also excluded as it is an acute fulminating disorder which invariably occurs in infants usually before the age of three years along with diffuse involvement of visceral organs [10].
The patient was referred to Department of Oral and Maxillofacial Surgery for surgical excision of the lesion. In case of LCH, the prognosis largely depends on the involvement of multiple organ systems. However, eosinophilic granuloma is a chronic localized form, the prognosis is good. It has also been suggested that the patients must be evaluated regularly during the first six months for any bone or visceral involvement and that long term follow up is important to rule out the possibility of recurrence [11,12].
Conclusion
Keeping in view the clinical manifestation of present case, though it is tempting us to suggest that LCH should also be included in the differential diagnosis of long standing, non-healing ulcers like non-healing diabetic ulcers, chronic ulcers due to trauma, necrotizing sialometaplasia, tuberculosis, deep fungal infections or ulcers in carcinomas occurring in oral cavity, it is difficult to decisively comment on the same till few more cases with similar features are reported in future.
[1]. Jalil Ab, Hin-Lau S, Oral Langerhans cell histiocytosis in Malaysian children:a 40-year experienceInt J Paediatr Dent 2009 19:349-53. [Google Scholar]
[2]. Anshita A, Gaurav P, Sarwar A, Benazeer H, A Case of Unifocal Eosinophilic Granuloma of the Mandible in an Adult Female: A Case ReportCase Rep Dent 2012 1:1-3. [Google Scholar]
[3]. Manfredi M, Corradi D, Vescovi P, Langerhans cell histiocytosis: a clinical case without bone involvementJ Periodontol 2005 76:143-47. [Google Scholar]
[4]. Joanna R, Paterson AW, Langerhans cell histiocytosis in an adultBrit J Oral Max Surg 2009 47:52-53. [Google Scholar]
[5]. Kilic E, Er N, Mavili E, Alkan A, Gunhan O, Oral mucosal involvement in Langerhans cell histiocytosis: long-term follow-up of a rare caseAust Dent J 2011 56:433-36. [Google Scholar]
[6]. Segura S, Pujol RM, Eosinophilic ulcer of the oral mucosa: a distinct entity or a non-specific reactive pattern?Oral Dis 2008 14:287-95. [Google Scholar]
[7]. Shashi R, Sailesh KM, Rashmi I, Atypical histiocytic granuloma: A differential to nonhealing ulcers of the oral cavityIndian J Dent Res 2014 25(3):406-09. [Google Scholar]
[8]. John H, Catherine MF, Langerhans cell histiocytosis: Current insights in a molecular age with emphasis on clinical oral and maxillofacial pathology practiceOral Surg Oral Med Oral Pathol Oral Radiol Endod 2005 100(2):S42-S66. [Google Scholar]
[9]. Regezi Oral Pathology: Clinical Pathologic Correlations 2003 4th editionElsevier:305 [Google Scholar]
[10]. Sheila W, Maarten E, Langerhans cell histiocytosis: update for the pediatricianCurr Opin Pediatr 2008 1:23-29. [Google Scholar]
[11]. Alajbeg I, Vucicevic RM, Femenic R, Arambasin C, Anicic M, Kelecic J, Unrecognized oral manifestations of Langerhans cell histiocytosis which progressed to systemic diseaseOral Oncol 2006 42(1):10-13. [Google Scholar]
[12]. Batra P, Roychoudury A, Prakash H, Langerhans cell histiocytosis- a case reportJ Indian Soc Pedo Prev Dent 2004 22(4):168-71. [Google Scholar]