Small Intestinal Obstruction Secondary to Jejunal Trichobezoar Removed Per Anum Without an Enterotomy: A Case Report
Devbrata Radhikamohan Adhikari1, Siddharth Vankipuram2, Ajeet Ramamani Tiwari3, Aniruddha Prabhakar Chaphekar4, Ritesh Suresh Satardey5
1Assistant Professor, Department of General Surgery, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai, India.
2Resident, Department of General Surgery, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai, India.
3Resident, Department of General Surgery, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai, India.
4Associate Professor, Department of General Surgery, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai, India.
5Resident, Department of General Surgery, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Devbrata Radhikamohan Adhikari, Assistant Professor, Department of General Surgery, 1st Floor, College Building, Topiwala National Medical College and Bai Yamunabai Laxman Nair Charitable Hospital, Mumbai Central, Mumbai-400008, India.
E-mail: Docdev84@gmail.com
Trichobezoars can rarely present with obstruction. This is usually due to collection of a hair ball in the stomach. We encountered an interesting case of small bowel obstruction due to a jejunal trichobezoar. The treatment generally is an enterotomy with removal of the hair ball. We report a case of a 29-year-old post partum female who presented to us with sub acute intestinal obstruction. Exploratory laparotomy revealed an impacted mass in the distal jejunum which was removed per anum without an enterotomy. Postoperative gastroscopy did not show trichobezoar in the stomach. This case highlights the importance of trichobezoar as a differential diagnosis in young women with small bowel obstruction that can be treated without an enterotomy and avoiding the risks and morbidities associated with it.
Acute abdominal pain, Bezoars, Rapunzel syndrome
Case Report
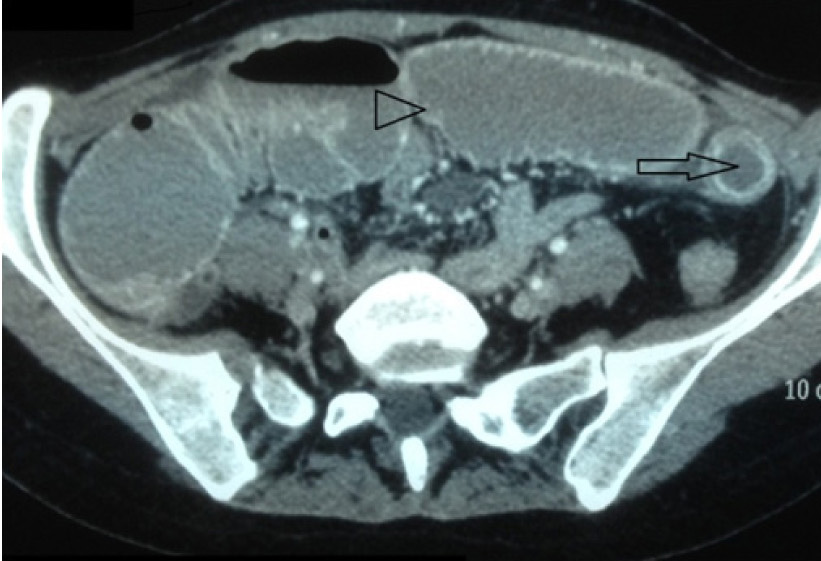
A 29-year-old woman presented to the emergency room with complaints of abdominal pain for five days, multiple episodes of vomiting, mild fever for two days and mild abdominal distention. On examination abdomen was soft with mild tenderness and distention. There was no palpable mass and hyperperistaltic bowel sounds were present. Per rectal examination showed soft stools. Routine blood investigations were normal. Naso gastric drainage was bilious around 100 ml on insertion. An erect plain X-ray of the abdomen showed few gas filled small bowel loops with a few air fluid levels. Ultrasound examination of the abdomen revealed multiple minimally dilated fluid filled bowel loops. Computerised tomograhy of the abdomen showed dilatation of small bowel loops 4 - 5 cm in diameter with transistion point seen at the level of proximal ileum. The large bowel distally appeared collapsed [Table/Fig-1]. Conservative management for sub acute small bowel obstruction with intravenous fluids and nasogastric decompression failed to improve her clinical condition over 24 h. Midline exploratory laparotomy was then performed as the patient did not improve loopsclinically. Intra-operatively, a 6 x 4 cm impacted pliable mass [Table/Fig-2] was found in the distal jejunum with proximal bowel loop dilatation. Distally, the bowel segment was found collapsed. There was no evidence of bowel ischemia or ulceration. The impacted mass was fragmented with fingers without doing an enterotomy and the fragments were gently milked beyond the ileocaecal valve, then all along the colon and removed per rectally. Thus removed specimen was a mixture of hair and semi-solid stools [Table/Fig-3].
The patient had an uncomplicated course after surgery. Retrospectively, further probing of patient’s history revealed symptoms of trichophagia since last one year. An upper G.I endoscopy done three weeks later did not demonstrate trichobezoar in the stomach. The patient is currently on long term psychiatric counselling.
Discussion
A bezoar is build up of undigested or partially digested material in the lumen of gastrointestinal tract. It can be composed of vegetable fibers (phytobezoar), medications (pharmacobezoar), undigested milk (lactobezoar) or foreign material such as hair (trichobezoar) [1,2]. Trichobezoars, unlike other bezoars are not associated with alterations in gastrointestinal motility [2].
Trichobezoars are almost exclusively seen in women with only isolated cases reported in males usually occurring between the age group of 13-20 [1,2]. They often coexist with underlying learning disabilities or psychiatric illness [2]. Large bezoars are generally contained in the stomach due to the pyloric sphincter. They may produce obstructive symptoms, including non bilious vomiting, dehydration and colicky abdominal pain [2,3]. Various criteria have been used to describe Rapunzel’s syndrome. Broadly it’s a stomach bezoar with extension up to ileocaecal junction that might lead to intestinal obstruction [1-5]. Our patient presented with a trichobezoar in the distal jejunum with no portion in the stomach which is unusual. Nicole et al., described a case report of a 45- year-old female with documented gastric trichoboezoar presenting one week later with small bowel obstruction in which laparotomy did not reveal any gastric component of the trichobezoar [4]. The precise mechanism probably involved migration of the trichobezoar from the stomach into the small bowel. Goyal et al., also reported a similar case of primary trichobezoar in the terminal ileum presenting as acute abdomen without any portion in the stomach [6]. The most common presenting features of trichobezoars are abdominal pain, nausea, vomiting progressing to obstruction and peritonitis [2]. Our patient presented with similar complaints of abdominal pain and vomiting but without any frank signs of peritonitis.
While, the gold standard in the diagnosis of trichobezoar remains upper GI endoscopy which also allows therapeutic intervention, a CT scan of the abdomen will usually reveal the trichobezoar. The diagnostic accuracy of CT is reported to be 73 to 95% [5]. In our case CT did not give us any clue that the obstruction was due to a trichobezoar. The modality of treatment depends upon the size, consistency and location of the bezoar. Small bezoars especially phytobezoars and lactobezoars are amenable to endoscopic treatment, however this modality is less effective for large trichobezoars [7]. Surgery is indicated when a very large or solid bezoar causes perforation or hemorrhage, or in the case of Rapunzel syndrome. Surgical removal can be accomplished using laparoscopy for small to moderate-size bezoars or by laparotomy for larger trichobezoars [2]. In our patient, we removed the trichobezoar without an enterotomy by fragmenting the impacted mass and milking distally beyond the ileocaecal valve. Glatstein et al., described a case report of a four year old child with impacted phytobezoar in the distal ileum which was similarly managed [8]. Similar techniques have been used by Aslan et al., and Das et al., for phytobezoars in the terminal ileum [9,10]. This may be one of the very few occasions where such a technique has been reported for an impacted jejunal trichobezoar. This alternative method of removing smaller trichobezoars without enterotomy decreases the risk of anastomotic leak and subsequent complications related to enterotomy. Few recurrences are reported after the initial removal of bezoars [3]. To decrease recurrences, long term psychiatric follow up is advised.
Contrast enhanced axial Computerized tomography scan of abdomen and pelvis showing dilated jejunal loops (arrow head) with transition point in proximal ileum (arrow)
Intraoperative findings showing 6cm x 4cm impacted pliable mass in the distal jejunum with proximal dilated small bowel loopsclinically

Fragmented specimen recovered post operatively showing a mixture of stool and hair

Conclusion
Trichobezoars causing small bowel intestinal obstruction are rare and need to be kept in mind in the differential diagnosis of young, female patients with intestinal obstruction. Further, enterotomy can be avoided in small uncomplicated trichobezoars to ensure quick recovery.
[1]. AU Emre, O Tascilar, G Karadeniz, O Irkorucu, K Karakaya, M Comert, Rapunzel syndrome of a cotton bezoar in a multimorbid patientClinics 2008 63:284-88. [Google Scholar]
[2]. M Iwamuro, S Tanaka, A Shiode, J Imagawa, M Mizuno, S Fujiki, Clinical characteristics and treatment outcomes of nineteen Japanese patients with gastro-intestinal bezoarsIntern Med 2014 53(11):1099-105. [Google Scholar]
[3]. SA Memon, P Mandhan, JN Qureshi, AJ Shairani, Recurrent Rapunzel syndrome – a case reportMed Sci Monit 2003 9:CS92-94. [Google Scholar]
[4]. Coufal Nicole G, Kansagra Akash P, Doucet Jay, Lee Jeanne, Coimbra Raul, Bansal Vishaln, Gastric Trichobezoar Causing Intermittent Small Bowel Obstruction: Report of a Case and Review of the LiteratureCase reports in Medicine 2011 vol. 2011. Article ID 217570. 3 pages [Google Scholar]
[5]. TW Ho, DC Koh, Small-bowel obstruction secondary to bezoar impaction: a diagnostic dilemma World J Surg 2007 31:1072-78. [Google Scholar]
[6]. V Goyal, PK Goyal, M Gupta, A rare case of small bowel obstruction due to primary trichobezoarJ Clin Diagn Res 2014 8(3):168-69. [Google Scholar]
[7]. YG Wang, U Seitz, ZL Li, N Soehendra, XA Qiao, Endoscopic management of huge bezoarsEndoscopy 1998 30:371-74. [Google Scholar]
[8]. M Glatstein, D Danino, A Rimon, S Keidar, D Scolnik, An unusual case of small bowel obstruction in a child: ingested rhubarbCase Rep Surg 2013 2013:49724 [Google Scholar]
[9]. PA Aslan, I Unal, G Karagazel, M MelikoÄŸlu, A case of intestinal obstruction due to phytobezoar--an alternative surgical approachSwiss Surg 2003 9:35-39. [Google Scholar]
[10]. SS Das, M Husain, A Bhat, FF Hajini, Phytobezoar Causing Terminal Ileal Obstruction–Can Enterotomy be Avoided?JSM Clin Case Rep 2014 2(2):1024 [Google Scholar]