In type I diabetes mellitus several genetic and epidemiologic factors have been recognized. Vitamin D is biologically plausible (it has a role in immune regulation).There is some epidemiologic evidence that decreased vitamin D level in pregnancy or early childhood may be associated with diabetic risk, but the evidence is not yet conclusive [1]. Low level of vitamin D has also been shown negative effect in β cells function [2,3]. In this study we evaluate glycemic changes after vitamin D3 supplement in patients with type I diabetes mellitus and vitamin D deficiency.
Materials and Methods
Samples are selected among patients with type I diabetes mellitus returning to pediatric endocrinology clinic in Taleghani Hospital, Gorgan, Iran. The prevalence of vitamin D deficiency in patients with type I diabetes mellitus was between 15% to 90.6% [4–6]. Usage of Medcalc software, with a 95% confidence interval and 80% power of test, 46 samples are at least required in this study. Patients previously had been diagnosed with diabetes mellitus criteria including two fasting blood glucose greater than 126 mg/dl or DKA presentation at first time. Patients with the following criteria were enrolled: older than six months of age, less than age of 17, vitamin D levels less than 50 nmol/lit, lack of secondary diabetes due to other diseases such as thalassemia or taking steroids, and lack of neonatal diabetes. The exclusion criteria include: irregular intake of vitamin D and calcium supplement, abnormal renal function, hypercalciuria with nephrolithiasis or nephrocalcinosis. This study was approved by the Ethics Committee of Gorgan University of Medical Sciences and prior to its beginning. Fifty three patients with type I diabetes participated. The baseline demographic characteristics including weight, height, BMI, BP, years of diabetes, type of treatment including the dose and type of insulin were recorded. HbA1C, 25OHD, PTH, Ca, P, Mg, Alk-P were performed. 25OHD by the method of Eliza with ELIZA READER STATFAX, and HbA1C by the method of immunoturbidometry with NYCOCARD, produced in Norway were performed. Ca, Mg, P and random urine Ca / Cr by AUTO ANALYSER Model Prestige24/I Japan, and PTH by the method of chemiluminoscence with SEIMENSE were measured. 25OHD levels were divided into 3 groups: vitamin D sufficiency (25OHD>51nmol/lit), vitamin D insufficiency (25OHD:35-50nmol/lit), and vitamin D deficiency (25OHD<34.5nmol/lit) [7–10]. HbA1C levels were defined based on the control of diabetes, as follows: good control (HbA1C<7.8%), fair control (HbA1C:7.8%-9.9%), and poor control (HbA1C>9.9%) [7,11]. Patients with vitamin D deficiency and vitamin D insufficiency treated with vitamin D supplement. Hypovitaminosis was treated with 300,000 IU vitamin D3 single dose intramuscular injection [7,8,12,13]. To prevent hungry bone due to vitamin D, 40mg/kg/day calcium in 2 divided doses was administered [8,12,14,15]. Calcium was continued for three months. Insulin dose was recorded by parents in these three months. After three months, patients were invited for repeat measurements of 25OHD and HbA1C. It is rather likelihood that usage of vitamin D can cause hypercalciuria, nephrocalcinosis, and nephrolithiasis [9] .Then random samples of urine calcium and creatinine were measured at the beginning of the study and after 12 weeks. If this level was greater than 0.2, renal sonography were requested to detect nephrolithiasis, and nephrocalcinosis.
Statistical Analysis
Spss16 software was used for statistical analysis and data were described by graphs and tables of numerical index. For comparison before and after 25OHD and HbA1C levels, paired T-test and Mann-Whitney test were used. According to the number of patients, in order to measure the mean of HbA1C in 3 levels of vitamin D adequacy, Kruskal-Wallis test was used. To compare the glycemic control of diabetes in 3 groups of vitamin D level, and 25OHD levels in 3 groups of diabetes control, McNemar test was used. The p-value of less than 0.05 was significant.
Results and Findings
In this study 53 patients with type I diabetes were investigated. 3 cases (5.66%) were vitamin D sufficient. 50 cases (94.3%) were vitamin D deficient and vitamin D insufficient, including 3 cases (6%) with vitamin D insufficiency and 47 cases (64%) with vitamin D deficiency. All of these patients were less than 17-year-old.
Patients were treated with vitamin D supplement. They were called back three months later. 6 patients excluded out of the study since 2 of them changed their correspondent address, and the other 4 refused their cooperation. The above mentioned cases were vitamin D deficient and had fair control.
Finally we had 44 patients for analysis, 21 cases (47.7%) were female and 23 cases (52.3%) were male. None of them previously had hypertension and proteinuria. A 16-year-old female patient with poor control HbA1C and vitamin D deficiency, suffered from retinopathy. Duration of diabetes mean ±SD was 3.62±2.18, between 6 months and 10 years.
27 patients (61.36%) used NPH/Regular insulin, and 17 (38.64%) used Glargine/Aspart insulin. From familial history point of view; 27(61.27%) had negative past history and 17(38.73%) had a positive history for two type of diabetes in their close sanguinity.
Mean ±SD HbA1C was 9.73±1.85 before the study which was diminished to 8.55±1.91 after vitamin D3 supplement treatment. This decline has a significant difference (p-value < 0.0001). Mean ± SD HbA1C was evaluated between groups of 25OHD [Table/Fig-1], separately with paired T-test. Decreasing in this parameter has a significant difference in vitamin D deficient group (p-value < 0.0001). By the usage of Mann-Whitney test had a non-significant difference in vitamin D insufficient group.
Mean ± SD HbA1C in sub groups of 25OHD level
| 25OHD level | | X±SD | HbA1C | |
|---|
| Number | Before Study | After Study | P-value |
|---|
| Vitamin D deficiency | 41 | 1.89 ±9.68 | 1.97 ±8.50 | <0.0001 |
| Vitamin D insufficiency | 3 | 1.04 ±10.47 | 0.72 ±9.20 | NS |
| Total | 44 | 1.85 ±9.73 | 1.91 ±8.55 | <0.0001 |
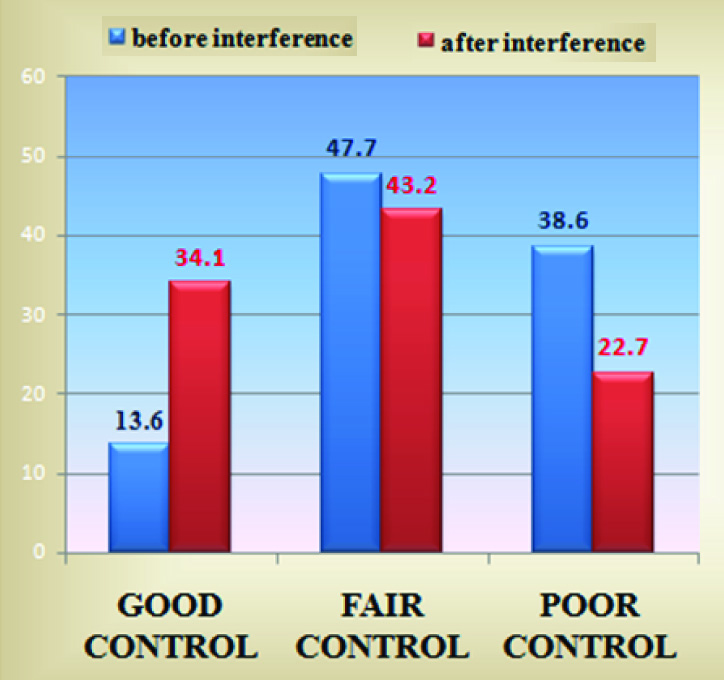
Before the interference, the glycemic control of patients in good, fair, and poor control were 6 (13.6%), 21 (47.7%), and 17(38.6%) respectively. After interference, the statistics changed respectively to 15(34.1%), 19(43.2%), and 10(22.7%). By McNemar test, these differences were significant) p-value<0.0001). Vitamin D3 supplement causes the improvement of HbA1C in all groups of glycemic control including HbA1C <7.8, 7.8-9.9, and >9.9. This supplement transfers patients toward better glycemic control in all groups (p-value < 0.0001) [Table/Fig-2]. Mean ± SD 25OHD was 17.33±8.97 nmol/lit before the study which is increased to 39.31 ±14.38 nmol/lit after treatment with vitamin D3 supplement. This increase also has a significant difference (p-value < 0.0001).
Comparison of glycemic control in patients with type I diabetes and vitamin D deficiency before and after interference
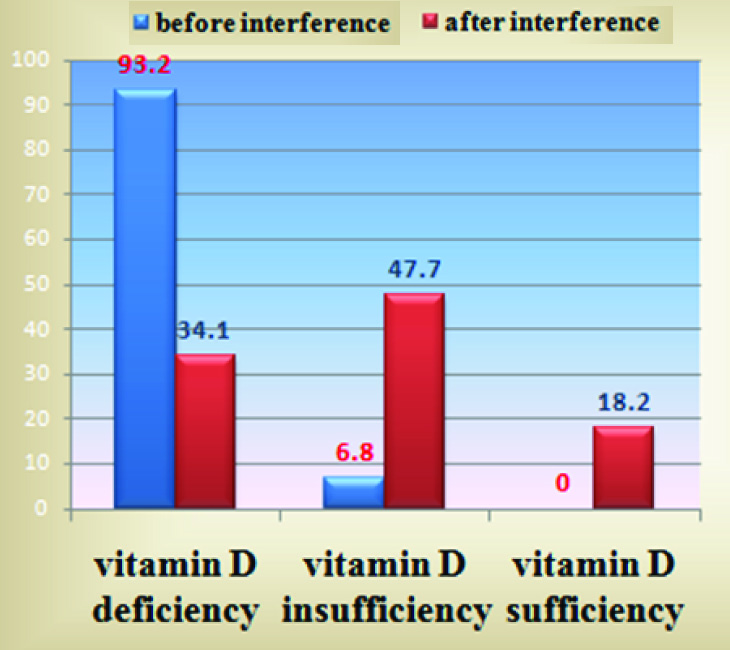
The changed adequacy of vitamin D based on 25OHD were 41(93.2%) vitamin D deficient and 3(6.8%) vitamin D insufficient before interference, then 15 (34.1%) vitamin D deficient, 21(47.7%) vitamin D insufficient, and 5(18.2%) vitamin D sufficient after interference [Table/Fig-3]. After intervention, the relative frequency of vitamin D deficiency and insufficiency was 81.8%. Insulin requirement for each patient was not changed during study and pre and post vitamin D supplement.
Comparison of 25OHD level in patients with type I diabetes and vitamin D deficiency before and after interference
Calcium, phosphorus, magnesium, and PTH were in the normal range. By Kruskal-Wallis test, mean for them were not different according to age and sex (p-value>0.05).
Hypercalciuria were defined with random Calcium/Creatinin ratio>0.2 in patients older than 2 y [16]. Before the study, 4 cases, then after the study another 3 cases (not previous cases) had hypercalciuria, normal renal sonography without dysuria and indication for treatment. We recommended them to follow up.
Discussion
In this study, it is shown that treatment with vitamin D3 causes better glycemic control in patients with type I diabetes mellitus. Moreover, vitamin D3 supplement causes the improvement of HbA1C in all groups of glycemic control including poor, fair and good. Increased level of 25OHD in all groups including sufficiency, deficiency and insufficiency of vitamin D was observed. According to mentioned numbers in previous studies, relative frequency of 94.3% (before supplement) in patients with type I diabetes, was expected. Gorgan has a rainy weather in most seasons of the year and climate has a significant role in this statistic. El Baba et al., showed lower level of 25OHD in patients with type I diabetes at the end of cloudy season [17]. In Aljabri study, more level of 25OHD with better glycemic control was observed [7]. In our study, reduction in mean HbA1C among vitamin D deficient group was statistically significant. It is notable we had only 44 children with type I diabetes and in Aljabri’s study 88 children and adults had been participated. In both of them, the effect of vitamin D on glycemic control had no differences according to age and sex.
The Thraikill et al., recognized vitamin D deficiency or insufficiency is slightly more prevalent in diabetic patients with microalbuminuria, especially with the increase in urinary vitamin D Binding protein excretion [18]. Attended children were already checked for microalbuminuria and had no problem. The Kaur et al., showed higher percentage of retinopathy in vitamin D deficient patients [19]. In this study we had a 16-year-old female with retinopathy which had poor control condition. Her sibling had no changes in HbA1C and 25OHD regardless of using similar supplement of other patients. Low level of vitamin D causes inflammatory process and increases microvascular complications [20].
Two studies in Iran suggest polymorphism of vitamin D receptor genes in type I diabetes mellitus [21,22]. In our study positive family history for two types of diabetes were 38.73% and changes in HbA1C and 25OHD did not differ in relatives and non- relatives (p-value>0.05). In another study, bidirectional relation between diabetes and vitamin D deficiency was expressed [18], and Borkar showed 86 percent of recent onset diabetic patients were vitamin D deficient [23]. Also, we had vitamin D deficiency in recent onset patients with diabetes.
Bizzarri’s study was not confirmed calcitriol protective effect on β cells function in recent onset diabetes [24]. Unlike that study, treatment response in our results did not differ in involvement duration group including <2 y and ≥2 y (p-value>0.05).
Our study was limited by number of patients and changes in address and telephone number. We need another study to follow our patients and possible changes in insulin requirement. Based on high incidence of vitamin D deficiency in patients with type I diabetes mellitus, we recommend serious treatment of this subject. It seems that when we encounter healthy patients with vitamin D deficiency, their family has also investigated for similar condition, especially when they have risk factor for diabetes. According to relation between retinopathy and vitamin D deficiency in Devaraj study, we propose early evaluation of vitamin D level in newly diagnosed children, and when the patient is vitamin D deficient, ophthalmologic checkup will be performed earlier and more frequent.
Finally, we offer patients with diabetes and vitamin D deficiency the daily dosage of 400 to 1000 IU of vitamin D [25], and maintenance dose of 3.5-9 gr / m2 elemental calcium [12]. Family member of patients with vitamin D deficiency, was also vitamin D deficient [8]. We recommend diagnostic evaluation in their family and treatment if needed.
Conclusion
Vitamin D3 supplement improves HbA1C in patients with type I diabetes and vitamin D deficiency.