Axillary nerve (ventral rami of C5 & C6) arises from the posterior cord of brachial plexus giving muscular branches to teres minor & deltoid. It also supplies the shoulder joint and the skin over it [1]. The axillary nerve is most commonly injured (6% of all the brachial plexus injuries) during numerous orthopaedic surgeries like shoulder arthroscopy, thermal shrinkage of the shoulder capsule (excessive temperature) and plate fixation (retraction of deltoid muscle) of the proximal humerus [2]. All these possible iatrogenic injuries are because of anatomical variations of the axillary nerve beneath the deltoid muscle. The shoulder joint dislocation and rotator cuff tear causes nerve injury which is called “unhappy triad” of the shoulder joint. The axillary nerve is vulnerable to damage during acute trauma to the shoulder or by chronic repeated trauma like in ‘quadrilateral space syndrome’ (entrapment of axillary nerve) [3]. There is an increased risk of nerve injury during intramuscular injections in deltoid, intra-articular and intra-bursal steroid injections due to lack of proper anatomical knowledge of the nerve [4–6]. It is very much necessary to appreciate the exact anatomical location of the nerve and its course to avoid the possible damages and to protect the nerve during surgeries and injections. Therefore, the objective of this present study is to explore the normal anatomy and possible variations of the axillary nerve in order to guide the surgeons and practitioners to be aware of them, and to have precise knowledge of ‘safe zones during operations that will reduce the incidence of iatrogenic nerve damage and will enhance the good clinical outcome during shoulder surgeries or intramuscular deltoid injections.
Materials and Methods
After the approval of the Institutional Ethical Committee, a total of 50 shoulder region specimens from 25 human adult embalmed cadavers (20 males and 05 females) with age 45-55 years, belonging to both right and left sides during first year M.B.B.S undergraduates dissection in the academic years from 2008–2013 in the Department of Anatomy, Azeezia Medical College, Kollam, Kerala state, were dissected to study the anatomy of axillary nerve. All the cadavers were routinely fixed in formalin as per standard procedure and the specimens having shoulder pathologies or which had surgical procedures were excluded. In the cadavers, shoulder regions were dissected as per the standard methods of dissection. Keeping in prone position, each cadaver (25 cadavers = 50 specimens including right and left sided) were dissected by an incision in the deltoid muscle along the longitudinal axis of humerus. The skin and fascia was removed over the shoulder region to expose the deltoid muscle. The muscle was separated from the spine of the scapula and turned downwards. Then, the remainder of deltoid, both clavicular and acromial heads were divided close to the origin and turned it downwards. After transecting its humeral insertion, it was turned upwards. Always care was taken so as to not to damage the axillary nerve and posterior circumflex humeral vessels that lies deep to the muscle. The deltoid muscle was separated into anterior, middle and posterior heads by following the white avascular raphe of connective tissue separating the muscle. The origin of the nerve from the brachial plexus was noted [Table/Fig-1]. The entire course of the nerve along with its branches and their accompanying structures were noted [Table/Fig-2]. The anterior, posterior and any other branches of the axillary nerve, the point of branching and their distribution were recorded [Table/Fig-3]. Quadrangular space dimensions like height, width, depth (in centimeter) were measured and the contents (axillary nerve and posterior circumflex humeral vessels) were identified.
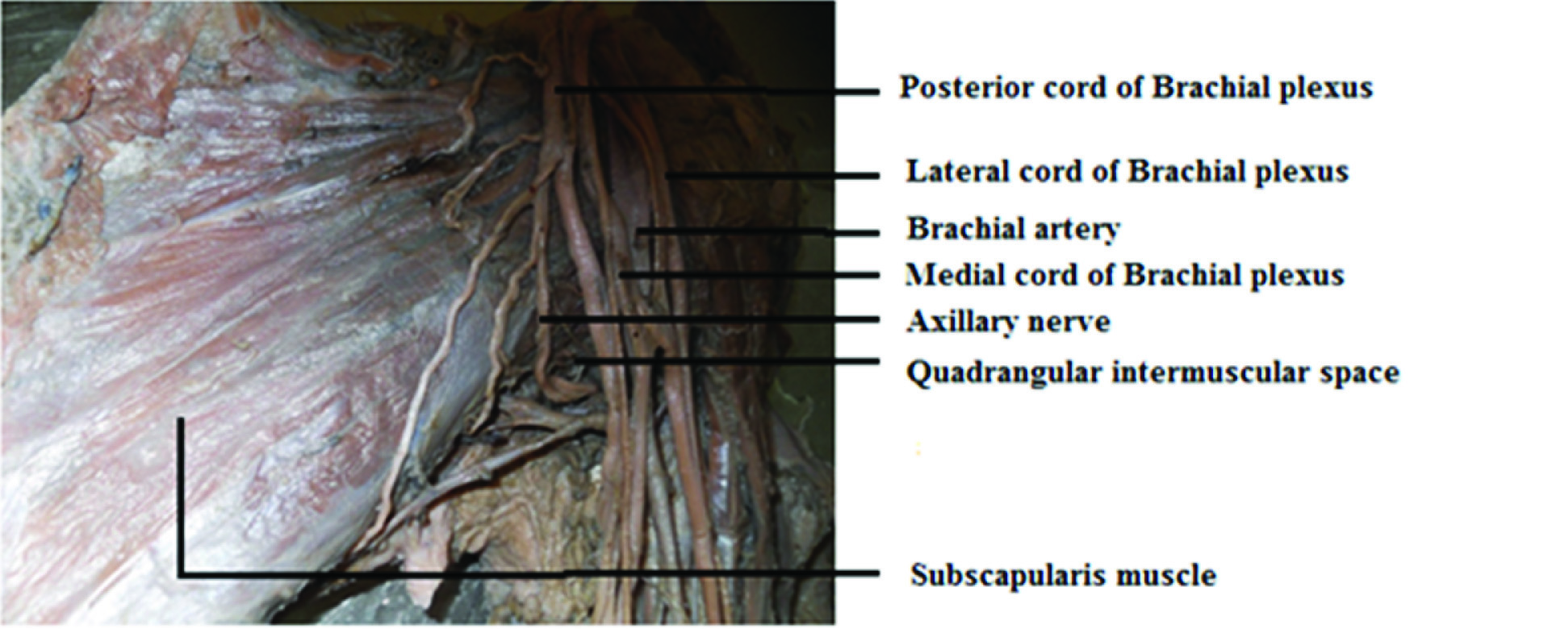
Origin of axillary nerve from posterior cord of brachial plexus – anterior view
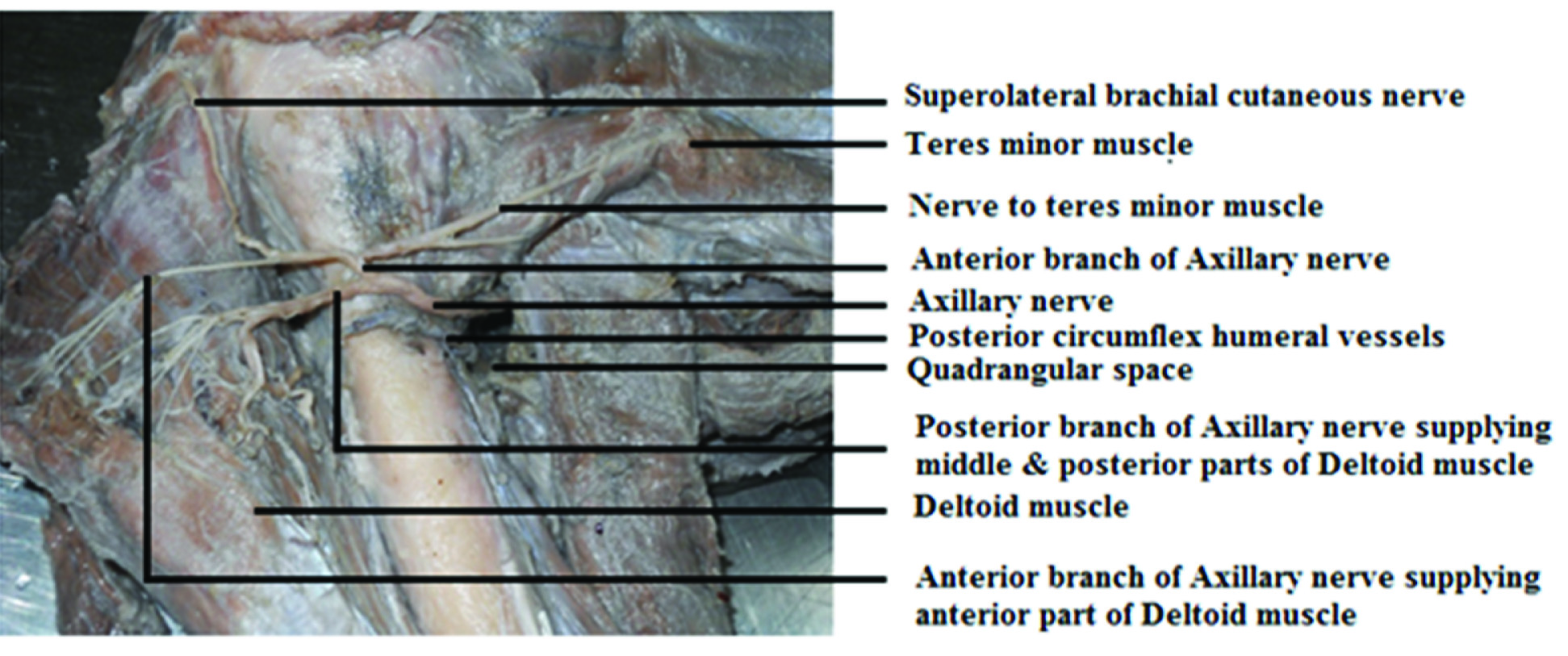
Course of axillary nerve – posterior view
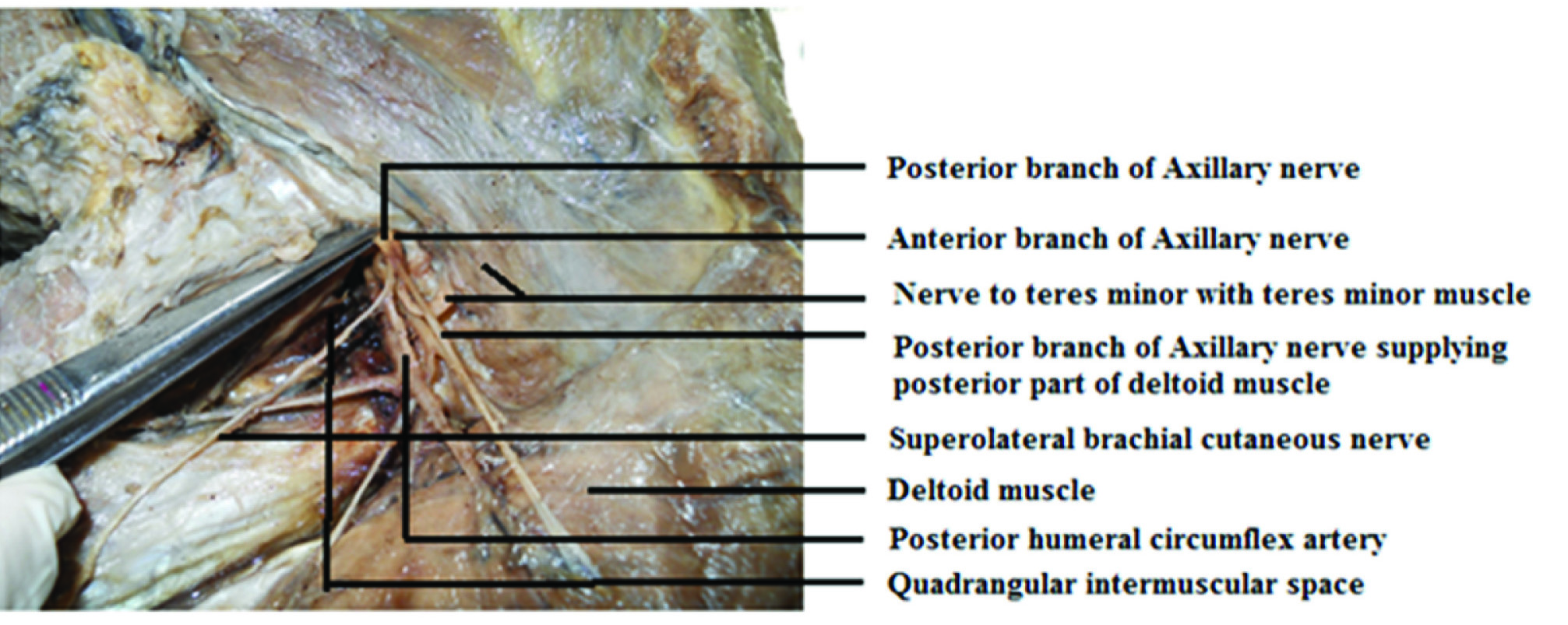
Course & branches of axillary nerve – posterior view
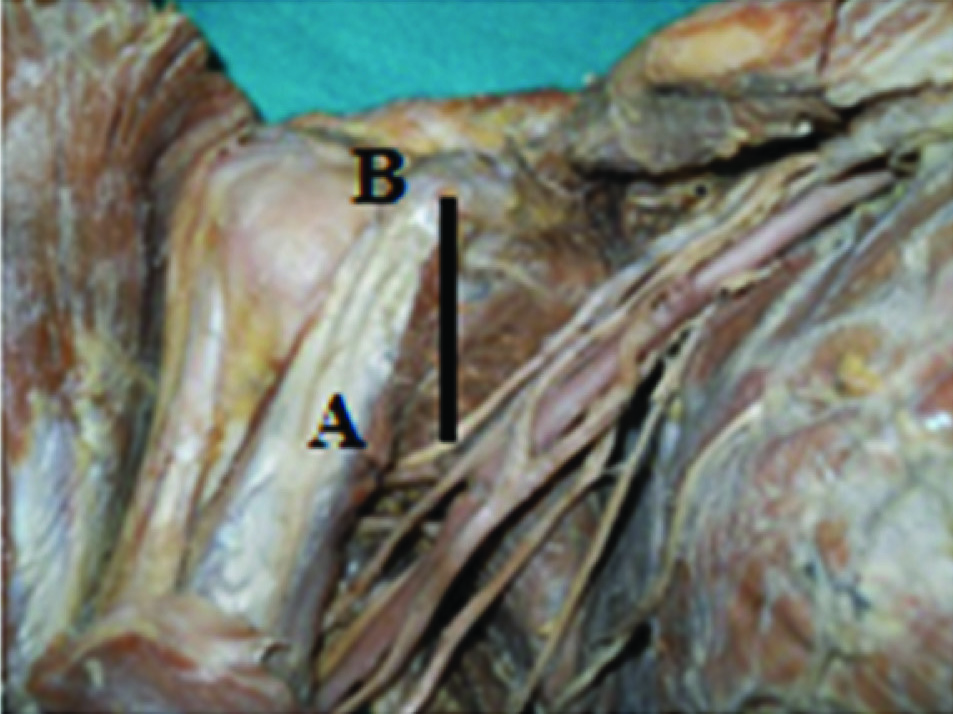
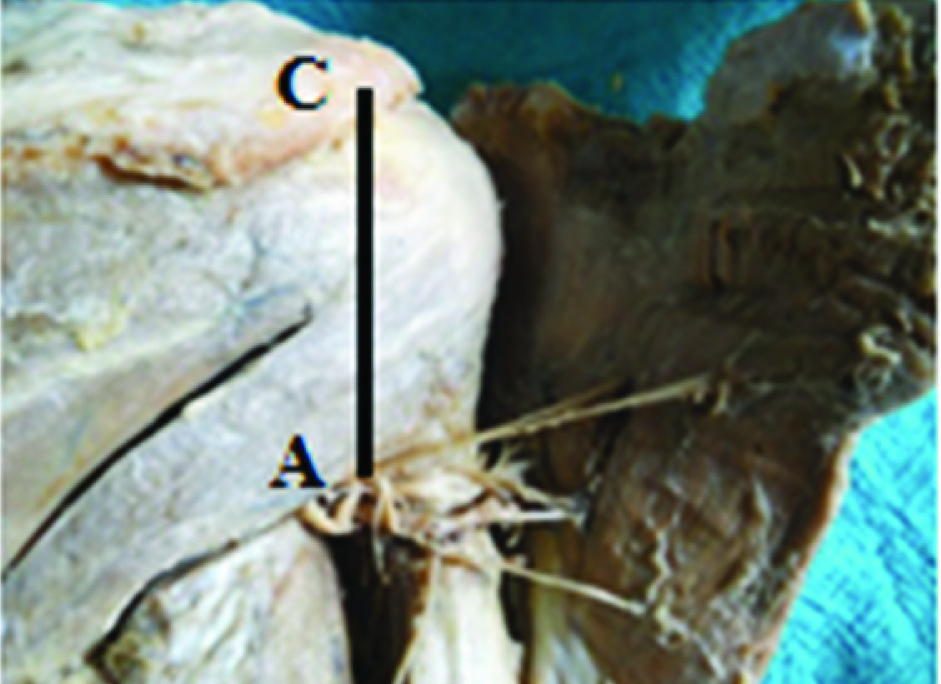
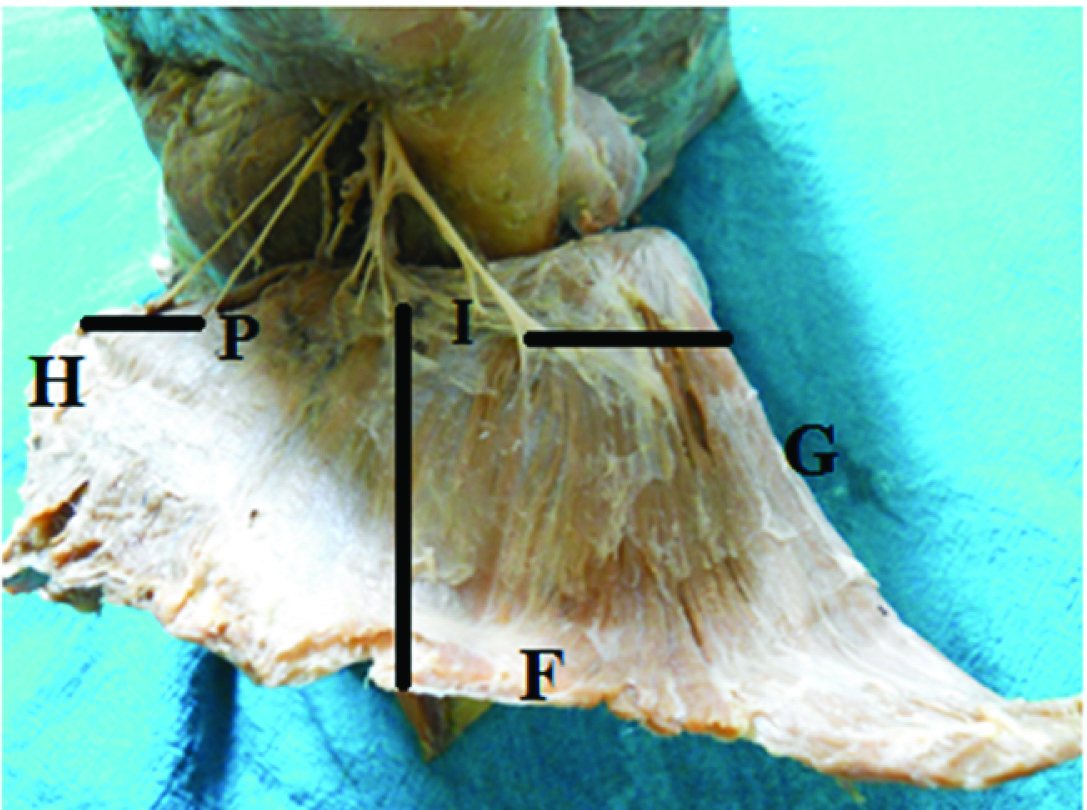
Using an electronic digital Vernier callipers, on the anterior aspect of the shoulder, the distance (AB) of the axillary nerve (A) at the point just before it entered the quadrangular space (just prior its division) from the anteromedial aspect of tip of coracoid process (B) was measured [Table/Fig-4], and also, the distance (AC) between the posterolateral aspect of the acromion process (C) and the nerve point (A) where it entered into thedeltoid muscle was measured [Table/Fig-5]. And with the same callipers, the distance (IE & ID respectively) of anterior branch of axillary nerve (I) from the midpoint of vertical deltoid distance (E) and from midpoint of deltoid insertion (D) were measured [Table/Fig-6] in centimeter and tabulated. Finally, axillary nerve was mapped beneath deltoid muscle by measuring the vertical distance (IF) of it from anterior upper border, from mid-middle upper border and from posterior upper border of the deltoid muscle. Similarly, horizontal distance of nerve (anterior branch – I & posterior branch – P) from anterior (G) and posterior (H) borders of deltoid muscle were recorded [Table/Fig-7], tabulated and photographs were taken.
Measuring the distance of axillary nerve (a) from the anteromedial aspect of tip of coracoid process (b)
Measuring the distance of axillary nerve (a) from posterolateral aspect of acromion process (c)
Measuring the distance of Anterior branch (I) of Axillary nerve from midpoint of Deltoid muscle insertion (D) & from midpoint of vertical length of Deltoid muscle (E).[F- Upper border of Deltoid]

Measuring the distance of anterior (i) & posterior branches (p) of axillary nerve from anterior border of deltoid (g), from posterior border of deltoid (h) & upper border of deltoid (f)
Results
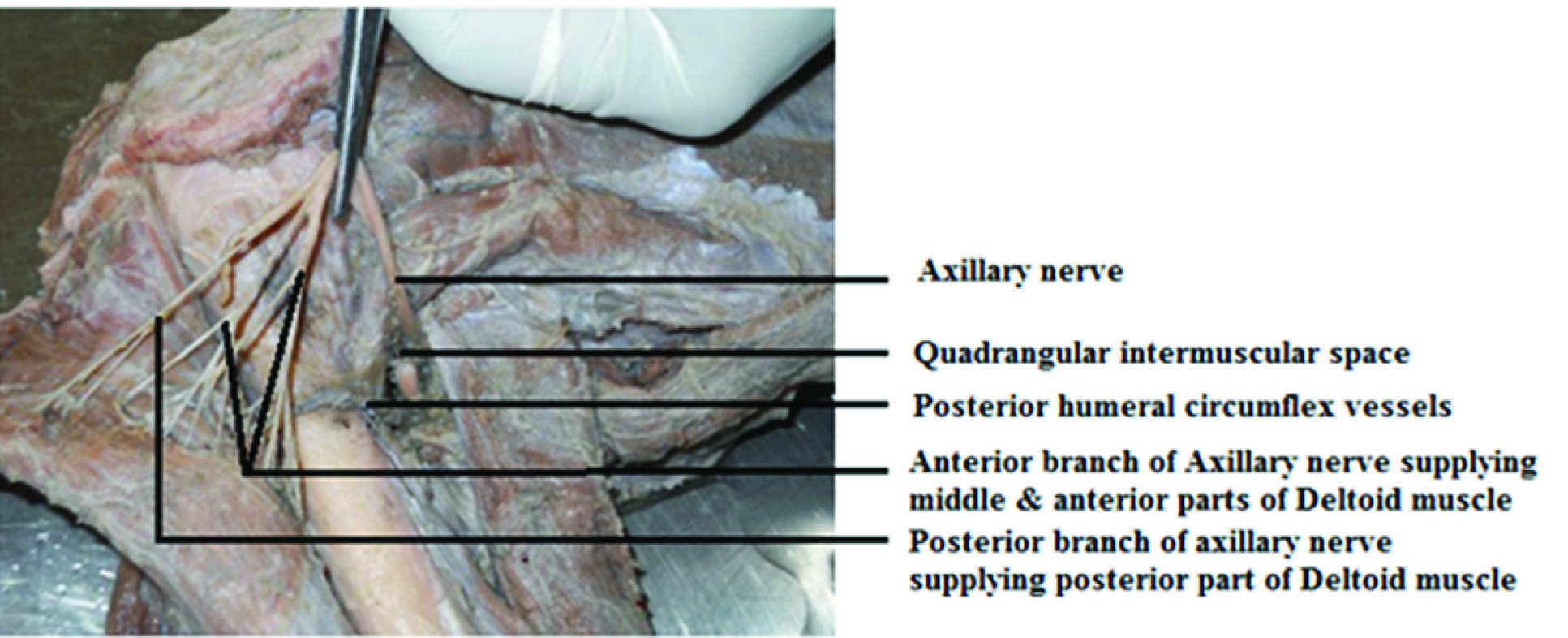
The axillary nerve in all the specimens observed to take origin from the posterior cord of brachial plexus [Table/Fig-1] giving anterior & posterior branches in quadrangular space (segment of the nerve from subscapularis to long head of triceps) & beneath the deltoid muscle in 88% & 12% respectively [Table/Fig-3]. In all the specimens, the axillary nerve found to course from origin to inferior border of subscapularis, then to long head of triceps, surgical neck of humerus finally runs beneath the deltoid muscle [Table/Fig-2,3]. Anterior branch of the axillary nerve found to be accompanied by posterior circumflex humeral vessels in quadrangular space of all the specimens, the nerve being above the vessels. The anterior part of the deltoid muscle was supplied by anterior branch (100%), middle part by anterior branch alone (56%), by both anterior and posterior branches (44%) & the posterior part of the deltoid by posterior branch alone (92%), by both posterior and anterior branches (08%). In all the specimens teres minor muscle is supplied by posterior branch, shoulder joint capsule by both anterior and posterior and posterior branch giving superolateral brachial cutaneous nerve [Table/Fig-8].
Muscular supply of Axillary nerve to Deltoid– Posterior view
The anterior branch of axillary nerve found to lie beneath the deltoid muscle at a mean distance of 6.71 ± 0.47 cm and 2.45 ± 0.48 cm, above the midpoint of deltoid muscle insertion and from the midpoint of vertical length of deltoid muscle respectively. Similarly, the mean distance between the nerve before it entered the quadrangular space (just prior its division) & the anteromedial aspect of tip of coracoid process was 3.56 ± 0.51 cm. The axillary nerve before it enters the deltoid muscle found to run at a mean distance of 7.46 ± 0.99 cm from the posterolateral aspect of acromion process [Table/Fig-9].The mean vertical distance of entering point of axillary nerve from the upper deltoid border was - anteriorly: 4.94 ± 0.86 cm, middle: 5.14 ± 0.90 & posteriorly: 5.44 ± 0.95 cm. Similarly, the mean horizontal distance was – anteriorly: 4.54 ± 0.65 & posteriorly: 3.22 ± 0.53 [Table/Fig-9]. The mean height, mean width & mean depth of Quadrangular space respectively was 2.23 ± 0.40 cm, 2.19 ± 0.22 cm & 1.25 ± 0.14 cm.
Statistical Analysis – 50 Axillary nerve specimens (overall)
| | Quadrangular Space Dimensions | Distance of Axillary Nerve from |
|---|
| Vertical Distance | Horizontal Distance |
|---|
| Midpoint Deltoid insertion | Antero-medial tip of Coracoid process | Postero-lateral aspect of Acromion process | Midpoint of vertical distance of Deltoid muscle | Ant. Upper | Mid. Middle | Post. Upper | Horiz. Ant. | Horiz. Post. |
|---|
| Height | Width | Depth |
|---|
| No. of | Samples | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 |
| Mean | 2.23 | 2.19 | 1.25 | 6.71 | 3.56 | 7.46 | 2.45 | 4.94 | 5.14 | 5.44 | 4.54 | 3.22 |
| Std. Deviation | 0.40 | 0.22 | 0.14 | 0.47 | 0.51 | 0.99 | 0.48 | 0.86 | 0.90 | 0.95 | 0.65 | 0.532 |
| Variance | 0.16 | 0.05 | 0.02 | 0.22 | 0.26 | 0.98 | 0.23 | 0.75 | 0.80 | 0.90 | 0.43 | 0.28 |
| Minimum | 1.6 | 1.6 | 1.0 | 5.8 | 2.2 | 3.6 | 1.6 | 3.0 | 3.2 | 3.4 | 3.0 | 2.0 |
| Maximum | 4.4 | 2.8 | 1.4 | 7.4 | 4.4 | 8.8 | 3.6 | 6.2 | 6.4 | 6.6 | 6.0 | 4.6 |
Statistical Analysis
Data were collected from 50 embalmed adult human cadaveric specimens (20 males and 05 females) belonging to both right and left sides, and entered in Microsoft excel and analysed by using SPSS 16th version. Mean, Proportion, Standard deviation and Unpaired t-test was applied for analysing the data obtained.
The results obtained after applying Unpaired t-test to the sex & to the distance of the axillary nerve from the important land marks were shown in [Table/Fig-10] and it was found to be highly significant (p≤0.05)
Statistical Analysis - Unpaired t-test for the sex (Comparison of Male & Female)
| | Male (n=40) | Female (n=10) | p- value |
|---|
| Mean | Std.Deviation | Mean | Std.Deviation |
|---|
| Quadrangular space Dimensions | Height | 2.34 | 0.36 | 1.80 | 0.13 | 0.00 |
| Width | 2.27 | 0.133 | 1.88 | 0.22 | 0.00 |
| Depth | 1.28 | 0.13 | 1.14 | 0.14 | 0.01 |
| Distance of Axillary nerve from | Midpoint of deltoid insertion | 6.88 | 0.36 | 6.06 | 0.23 | 0.00 |
| Anteromedial tip of coracoid process | 3.73 | 0.38 | 2.90 | 0.46 | 0.00 |
| Posterolateral aspect of acromion process | 7.74 | 0.82 | 6.32 | 0.77 | 0.00 |
| Midpoint of vertical deltoid distance | 2.54 | 0.46 | 2.10 | 0.39 | 0.01 |
| Distance of Axillary nerve beneath Deltoid muscle from | Vertical distance | Anterior upper border | 5.13 | 0.85 | 4.18 | 0.38 | 0.00 |
| Mid middle upper border | 5.39 | 0.81 | 4.14 | 0.35 | 0.00 |
| Posterior upper border | 5.69 | 0.89 | 4.46 | 0.39 | 0.00 |
| Horizontal distance | Horizontal anterior border | 4.65 | 0.68 | 4.10 | 0.17 | 0.02 |
| Horizontal posterior border | 3.30 | 0.57 | 2.91 | 0.14 | 0.04 |
The results found after applying Unpaired t-test to the sides & to the distance of the axillary nerve from important landmarks were shown in [Table/Fig-11], which was found to be not significant (p ≥ 0.05).The Quadrangular space dimensions (height, width & depth) found to be not significant (p ≥ 0.05), but depth of Quadrangular space found to be significant (p=0.01, which is less than 0.05).
Statistical Analysis-Unpaired t-test for the sides (Comparison of Right & Left sides- 25 each side)
| | Right side (n=25) | Left side (n=25) | p-value |
|---|
| Mean | Std.Deviation | Mean | Std.Deviation |
|---|
| Quadrangular space Dimensions | Height | 2.08 | 0.28 | 2.26 | 0.51 | 0.59 |
| Width | 2.04 | 0.20 | 2.15 | 0.19 | 0.56 |
| Depth | 1.0 | 0.01 | 1.18 | 0.15 | 0.01 |
| Distance of Axillary nerve from | Midpoint of deltoid insertion | 6.56 | 0.51 | 6.79 | 0.49 | 0.34 |
| Anteromedial tip of coracoid process | 3.60 | 0.58 | 3.54 | 0.55 | 0.87 |
| Posterolateral aspect of acromion process | 7.60 | 0.87 | 7.35 | 1.14 | 0.43 |
| Midpoint of vertical deltoid distance | 2.48 | 0.51 | 2.41 | 0.48 | 0.41 |
| Distance of Axillary nerve beneath Deltoid muscle from | Vertical distance | Anterior upper border | 4.96 | 0.98 | 4.98 | 0.83 | 0.83 |
| Mid middle upper border | 5.08 | 0.95 | 5.15 | 0.88 | 0.97 |
| Posterior upper border | 5.36 | 1.11 | 5.46 | 0.91 | 0.95 |
| Horizontal distance | Horizontal anterior border | 4.44 | 0.71 | 4.60 | 0.66 | 0.46 |
| Horizontal posterior border | 3.20 | 0.65 | 3.28 | 0.56 | 0.28 |
Discussion
Mario Loukas et al., studied the axillary nerve in 50 human cadavers and observed that it took origin from the posterior cord in all the specimens and enter the quadrangular space descending infero laterally on the anterior surface of subscapularis muscle. They observed that the nerve gave branches to anterior, middle, and posterior parts of the deltoid; a branch to teres minor and the superior lateral brachial cutaneous nerve. The division of axillary nerve into anterior and posterior branches occur in quadrangular space and within deltoid muscle in 65% and 35% respectively. They also found that the posterior branch of deltoid muscle gave a branch to teres minor & superior lateral brachial cutaneous nerve in 100% cases. The branches to posterior and middle parts of deltoid were present in 100% & 38% cases respectively. The anterior branch of deltoid found to supply the anterior and middle parts of deltoid muscle in 100% specimens and also supplied the shoulder joint capsule and the posterior part of the deltoid muscle in 18% of the cases. The middle and posterior parts of the deltoid muscle were supplied by both anterior and posterior branches in 38% & 08% of the cases respectively [2].
Our present study revealed that in all the specimens (100% cases), the axillary nerve found to take origin from the posterior cord of brachial plexus [Table/Fig-1] and coursing from the origin to the inferior border of subscapularis, long head of triceps, surgical neck of humerus and finally entering the deltoid muscle [Table/Fig-2,3].
In another study, 30 shoulders were dissected in fixed adult cadavers and revealed that in all the cases, the posterior branch of axillary nerve gave off its first muscular branch to innervate the teres minor, and the acromial & clavicular parts of the deltoid muscle were observed to be innervated by anterior branch; but posterior part of the deltoid was innervated by posterior branch only (70%), by both anterior and posterior branches (26.7%) and by only anterior branch (3.3%) [7].
In this current study, anterior branch of the axillary nerve found to supply anterior part of the deltoid muscle (100%). The middle part of the deltoid muscle was supplied by anterior branch alone in 56% cases & by both anterior and posterior branches in 44%. Similarly, posterior part of the deltoid was supplied by posterior branch alone (92%) & by both branches in 8%. Shoulder joint capsule was supplied by both anterior & posterior branches in 100% cases. The posterior branch of the axillary nerve found to supply teres minor & give superolateral brachial cutaneous nerve in all the specimens (100%) [Table/Fig-8].
In a study of 30 specimens, axillary nerve found to branch into its muscular components within the quadrangular space in 33% & posterior to it in 66% cases. The cutaneous component of the axillary nerve branched from the main trunk of the nerve posterior to the quadrangular space in 100% cases [8].
In our study, the axillary nerve found to divide into anterior and posterior branches in Quadrangular space (that is a nerve segment from subscapularis to long head of triceps) in 88% cases & within deltoid muscle in 12% [Table/Fig-3].
In a cadaveric study from 19 fresh frozen human cadavers through posterior approach dissection, it was found that the posterior branch of the axillary nerve has an intimate association with the inferior aspects of the glenoid and the shoulder joint capsule, which may place it at a particular risk during capsular plication or thermal shrinkage procedures. The superior – lateral brachial cutaneous nerve and the nerve to the teres minor always aroused from the posterior branch that supplies skin over the shoulder [9].
In a dissection study of 32 shoulders from embalmed adult cadavers, the axillary nerve had been divided into five segments from its origin to intramuscular distribution in the deltoid muscle in order to define a few morphological features of anatomy which is useful for the physician, the radiologist or the surgeon for the evaluation or operative procedures on the axillary nerve and to provide a hypothesis about the variable aspects of injuries of the nerve [10].
In a cadaveric study of 30 specimens to measure the dimensions and the contents of the quadrangular space, it was found that the mean height of this space was 2.5 cm, mean width 2.5cm and its mean depth was 1.5 cm. Axillary nerve was always the most superior structure in the space in all the cases hugging the surgical neck of humerus along with the artery [8].
In our study, the mean height, width & depth found to be (in cm) 2.23, 2.19 & 1.25 respectively. And the contents of the space were anterior branch of axillary nerve accompanied by posterior circumflex humeral vessels, nerve being superior in all the specimens.
In a cadaveric study, it was found that the distance between the anteromedial aspect of the coracoid process and the axillary nerve was 3-4 cm [3].
In a dissection study of 30 human cadavers, it was found that the axillary nerve was consistently located within an anatomical triangle constructed by lines passing between the coracobrachialis and the pectoralis minor muscles and the axillary artery. The study also revealed the distance between the axillary nerve and tip of the coracoid process was 4 cm [11].
In a study of 30 shoulders of 15 fixed adult cadavers, it was observed that the axillary nerve found to be at a mean distance of 3.7 cm & 1.1 cm from the anteromedial aspect of the coracoid tip and the glenoid labrum respectively. The mean distance between the tip of anteromedial aspect of the coracoid process and the medial edge of the subscapularis muscle was measured to be 2.5 cm [12].
In our present study, it was found that the mean distance between the axillary nerve at the point just before it entered the quadrangular space (just prior its division) & the anteromedial aspect of the tip of the coracoid process was 3.56 ± 0.51 cm [Table/Fig-4].
In a study of 30 shoulder specimens, it was recorded that the mean distance from the posterolateral aspect of the acromion process to the axillary nerve and its branches was 7.8 cm [7].
Ozgur Cetik et al., observed in their study that, the axillary nerve at an every point was not at a constant distance from the tip of acromion process along its course. They found the distance between the axillary nerve and the tip of the acromion process, and its relation to arm length. They concluded a quadrangular shape area above the axillary nerve whose length of the lateral edges were dependent on individual arm length [13].
In an anatomical study of 16 unembalmed cadavers, they observed that the mean distance between the point where the axillary nerve entered into the deltoid muscle and the humeral head was 5.0 cm, and it was 6.8 cm from the acromion process. And the mean distance between the origins of the anterior and posterior branches of the axillary nerve was 5.4 cm indicating the – safe zone – during trans deltoid approaches to the shoulder is the anterior region of the deltoid muscle for a maximum of 6.7 cm from the acromion process [14].
Burkhead et al., found from their study of axillary nerve in 51 embalmed and 5 fresh cadaveric specimens that the distance of the axillary nerve from the palpable tip of the acromion process was 5 cm (minimum being 3.1 cm) [15].
In a dissection study of 42 embalmed shoulder specimens (20 male & 22 female), it had been found that the mean distance between acromio-clavicular joint and the axillary nerve was 7.90 cm (7.2-9.1 cm) in males and 6.37 cm (5.2 – 8.1 cm) in females. This study also revealed the axillary nerve index average being 0.48 (0.42-0.57) in males and 0.41 (0.31-0.57) in females. The axillary nerve index was described as the ratio between the distance of the nerve from acromio- clavocualr joint and the length of the deltoid from the anterior clavicular line and this was proposed as a useful guide for the estimation of position of the nerve at the time of surgery [16].
This present study revealed that the mean distance of axillary nerve from posterolateral aspect of acromion process found to be 7.46 ± 0.99 cm [Table/Fig-5].
Kontakis GM et al., in their study of 67 cadavers found that the vertical distance of axillary nerve from the upper deltoid border was less than 4 cm in both sided shoulders of 17 cadavers and the minimal distance between axillary nerve and the mid-middle portion of the deltoid was found to be 2 cm. This study also concluded that the vertical distance of axillary nerve from the upper border of the deltoid was less than 4 cm in both shoulders (right and left), having a minimal measured distance of 2 cm. The axillary nerve was located a mean of 2.6 (1.7 – 3.4) cm above the midpoint of the vertical length of the deltoid. Taking into the account of dimensions of the deltoid, the surgeons can protect the nerve during surgery. The shorter the deltoid length, the greater the danger of damaging the nerve at a short distance from the upper border of the muscle. The deltoid ratio is useful for the estimation of the axillary nerve position, especially the vertical distance from the middle of the acromion. Their study also revealed the vertical distance (in centimetre) from the upper deltoid border to the axillary nerve as 4.5 (2.5-6.5) anteriorly,4.6 (2-6) middle and 5.0 (3-7.5) posteriorly. Similarly, the horizontal distance from the anterior and posterior borders to the entering points of the nerve was measured to be 4.3 (3-6) and 2.9 (2-4) [17].
In a cadaveric dissection study, it was found thatthe axillary nerve is 2.2 – 2.6 cm above the midpoint of the vertical length of the deltoid muscle [18].
In this present study, it was measured that the anterior branch of axillary nerve beneath the deltoid muscle lies at a mean distance of 2.45 ± 0.48 cm (1.6 – 3.6) from the midpoint of vertical length of deltoid muscle [Table/Fig-6]. The distance between the same nerve and the midpoint of deltoid insertion found to be 6.7±0.47cm [Table/Fig-6].This study also concluded that the anterior branch of axillary nerve was measured (centimetre) to be at a distance of 4.94 (3.0-6.2), 5.14 (3.2-6.4) & 5.44 (3.4-6.6) from vertical anterior, vertical middle & vertical posterior of deltoid muscle respectively. Similarly, the anterior branch was found to be at 4.54 (3.0-6.0) from anterior border of deltoid muscle & the posterior branch at 3.22 (2.0-4.6) from posterior border of deltoid horizontally [Table/Fig-7].
In an evidence based study by anthropometric measurements, it had been observed that the midpoint of the muscle (midway between the acromion and the deltoid tuberosity) with the arm abducted to 60o is a safe site for intra muscular injection in deltoid muscle [5].
Nakatani et al., studied the course of axillary nerve and suggested the surface marking of it for the safe administration of deltoid intramuscular injection without injuring the nerve. Their study revealed the safe surface mark of axillary nerve i.e. a transverse line present at the lower 3rd between the superolateral margin of the acromion antero-posterior axillary line [6].
Conclusion
From the study of total 50 dissected cadaveric axillary nerve specimens (20 Males & 05 Females) including both right & left sides, and comparing our study with the previous works, it can be concluded that the axillary nerve found to take origin from the posterior cord of brachial plexus (100%) dividing into anterior & posterior branches in Quadrangular space (88%) and supply deltoid muscle mainly. It also gave branches to teres minor muscle, shoulder joint capsule & superolateral brachial cutaneous nerve (100%). This study concluded that the mean distance of axillary nerve from the anteromedial aspect of tip of coracoid process, posterolateral aspect of acromion process, midpoint of deltoid insertion & from the midpoint of vertical length of deltoid muscle measured to be (in cm) as 3.56±0.51, 7.4±0.99, 6.7±0.47 & 2.45±0.48 respectively. The mean vertical distance of entering point of axillary nerve from the anterior upper, mid middle upper & posterior upper deltoid border found to be (in cm): 4.94±0.86, 5.14±0.90 & 5.44±0.95 respectively, and the horizontal anterior & horizontal posterior mean distance being 4.54±0.65 & 3.22±0.53 respectively. The mean height, mean width & mean depth of Quadrangular space measured to be (in cm): 2.23±0.40, 2.19±0.22 & 1.25±0.14 respectively. The statistical analysis concluded that all the findings found to be highly significant when males compared with females but not significant when sides (right & left) were compared.
Acknowledgment
I sincerely express my profound heartfelt gratitude to the Management of the Institution, Principal, Head of the Department, Colleagues, other teaching and non-teaching staffs of the department for their constant and unfailing kind support, valuable suggestions and encouragement directly or indirectly to carry out this work.
Source of Support
After the approval of the Institutional Ethical Committee, a total of 50 shoulder region of human adult embalmed cadaveric specimens (20 Males and 05 Females) belonging to both the right and left side, with an average of 45-55 years, during M.B.B.S – Ist year undergraduates dissection from 2008–2013 in the Department of Anatomy, Azeezia Medical College, Meeyyannoor, Kollam, Kerala, India.