Purpose: To evaluate the foveal and macular thickness in various degrees of myopia and its association with axial length in low, moderate and high degrees of myopia.
Design: A cross-sectional study was done in the Department of Ophthalmology, MGMCRI, Pondicherry, India.
Materials and Methods: One hundred and twenty five eyes eyes of 64 myopic subjects between the age group of 20-40 who fulfilled the inclusion criteria were selected and complete ophthalmic examination was done. Cycloplegic refraction was done and the subjects were categorized into low (n=43 eyes), moderate (n=43 eyes) and high (n=36) degrees of myopia. The foveal and macular thickness was assessed using spectral OCT- SLO and axial length was measured by A-scan biometry.
Results: The foveae minimum of high myopia (178 ± 26.4 microns) was significantly thicker compared to moderate myopia (p= 0.028). There was no significant intergroup difference in the thickness significance of the outer and inner macular between mild, moderate and high degree of myopia. The mean axial length of high myopia (26.7±0.97mm) was significantly higher compared to moderate (24.6±0.81mm) and low myopia (23.5±0.81mm) with a p-value of p = 0.001. There was a positive correlation of axial length with foveae minimum, fovea and superior inner macula in respect to myopia (p<0.05).
Conclusion: The foveal and macular thickness in myopia is influenced by the axial length. Early detection of such changes in macular thickness by using OCT is helpful in understanding the mechanism and factors affecting the structural changes of myopic eyes. Also it implicates the importance of refractive error induced retinal macular changes while interpreting OCT.
Introduction
Myopia is defined as the state of refraction in which parallel rays of light are brought to focus in front of the retina with accommodation at rest [1-3] . This result in blurred distant vision. The increasing prevalence of myopia has become a major public health impact due to its potentially blinding ocular complications like retinal detachment and glaucoma. In myopic children retinal defocus due to inaccurate accommodation during close work may be a stimulus for increase in elongation of axial length and progression of myopia [4] . In high myopia scleral ectasias are relatively frequent and it involves the posterior pole of the eye leading to poor visual prognosis in adult life [5] . Also, the risk of chorioretinal abnormalities such as retinal detachment, chorioretinal atrophy, lacquer cracks, Foster Fuchs spot, Pigmentary degeneration, Lattice degeneration, posterior staphyloma increased with severity of myopia and increase in axial length [6] . The prevalence of cataract [7] – posterior sub capsular, nuclear cataract and Glaucoma [7] – ocular hypertension, primary open angle glaucoma are found more in high myopia [8] . High degree of myopia is associated with retinal detachment at younger age groups [9] . The vitreous undergoes liquefaction and degeneration which leads to vitreous opacities [5] and posterior vitreous detachment (PVD). An incomplete PVD causes tractional forces on the retina leading to macular damage such as retinoschisis, lamellar holes, shallow foveal detachment and macular hole. These changes are called as ‘Myopic Tractional Maculopathy’ [10] . The traditional methods for evaluating such changes in the fundus are not sensitive to small changes in retinal thickness and are qualitative at best [11]. With the advent of optical coherence tomography (OCT), it has allowed the clinicians to reliably detect and measure small changes Krishnagopal2in macular thickness and to quantitatively evaluate the efficacy of different therapeutic modalities.
This study is to correlate the variations in macular retinal thickness in mild, moderate and high myopia between the age group of 20-40 y by optical coherence tomography and to correlate the axial length with foveal and macular thickness in various degrees of myopia.
Materials and Methods
This was a prospective observational study which was conducted at the Department of Ophthalmology of a rural tertiary care hospital. The Institutional Medical Ethics Committee approved this study. From March 2013 to April 2014 we enrolled all myopic patients who fulfilled the inclusion criteria with spherical equivalent (SE) of at least -0.50 D; between the age group of 20- 40 y attending the Dept. of Ophthalmology. Patients with pseudoexfoliation, uveitis, pigment dispersion syndrome, corneal opacities, retinal disease, previous refractive or intraocular surgeries, intraocular pressure of more than 21 mmHg and any grade of nuclear sclerosis as defined by Lens Opacities Classification System (LOCS) 3 were excluded. An informed written consent was obtained from the patients.
A detailed ophthalmic history regarding the duration of myopia, history of spectacle usage, previous refractive or intra ocular surgery was obtained and then subjected to routine ophthalmic examination. Recording of visual acuity by Snellen’s chart, intraocular pressure by Goldman’s applanation tonometry, slit lamp examination of anterior segment, and fundus evaluation by slitlamp biomicroscopy using 90 D and indirect ophthalmoscope was done. Cycloplegic refraction was done once pupil was dilated by installation of Tropicamide+phenylephrine eye drops. Post mydriatic test was done after one day and patients were assigned to 3 groups according to the degree of myopia which is classified as Mild -0.50 to -3.00D, Moderate -3.25 to -6.00D, high > -6.00D. Axial length measurement by A- scans ultrasound biometry (Appascan AME 10A).Macular and foveal thickness assessment by third generation OCT – (OPTOS SPECTRAL OCT/SLO). Which is a combination of OCT and scanning laser ophthalmoscope (SLO) designed to image the vitreo- retina, retina and choroidal-retinal structure as well as provide a confocal fundus image perfectly linked to OCT B-scan image.
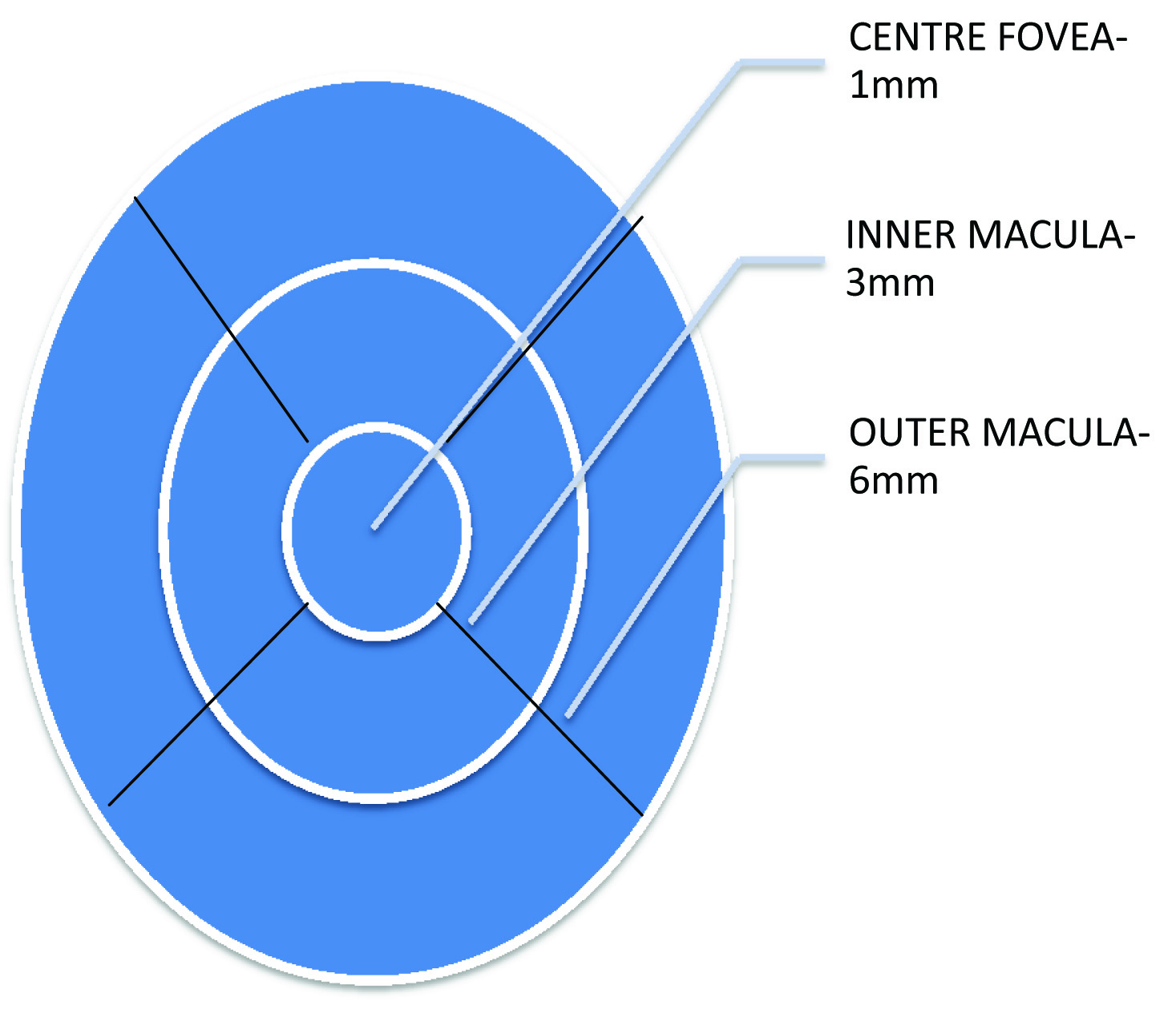
The 3D retinal topography uses the fast macular scan protocol to measure the macular thickness. The macular area was divided into three concentric rings centred on the fovea [Table/Fig-1]. The thickness of foveola was calculated from the mean central point of foveal thickness. The inner and outer rings were divided into four quadrants – Temporal, Nasal, Superior and Inferior quadrants. The data from 4 quadrants of inner, outer & centre rings were recorded and analyzed by the version OCT system 4.0 software. The measurements are compared to set parameters in the normative database and can be compared over time. All instrument handling and measurements were done by the same person.
Statistical Analysis
According to WHO manual for sample size determination in health studies, with a precision of 20% and confidence interval of 90% and prevalence of myopia from previous study as 34.6% the sample size is calculated as 22 in each group. The study subjects were described according to their demographic profiles such as age, gender and type of eyes in terms of percentages according to the degree of myopia. The degrees of myopia were classified in to three category such as High, Moderate and Mild. The macular retinal thicknesses between the three categories were compared by ANOVA test. The above statistical procedures were performed by the statistical package namely IBM SPSS statistics-20. The p-values less than 0.05 (p<0.05) were considered as statistically significant in two tail test.
Results
Among the 64 patients, 35 were females and 29 were males. A total of 125 eyes were examined of which 39 eyes of 20 patients in high myopia, 43 eyes of 22 patients in moderate and 43 eyes of 22 patients mild myopia were included. In respect of total eyes the percentage of myopia was 31.3% in high myopia and the other two categories were 34.4% each.
The mean ages of high, moderate and mild category were 25.7±6.5 y, 22.7±3.7 y and 24.0±5.1 y respectively.
The foveae minimum (178±26.4) of high degree of myopia was significantly thicker compared to mild (171± 18.1) and moderate group (165.5±21.2) with p<0.05. Similarly the fovea of high myopia (205.1±21.0) was greater than mild (197.3±23.2) and moderate group (194±24.0) but was not statistically significant with p>0.05.The inner and outer macular thickness of high myopia was thinner when compared to mild and moderate groups. But there was no statistical significant inter group difference in the macular thickness between the three groups [Table/Fig-2].
The mean axial length of high degree myopia (26.7±0.97) was statistically very highly significant with the other two categories such as Moderate (24.6±0.81) and mild (23.5±0.81) [Table/Fig-3]
In total myopic eyes, Foveae Minimum & Fovea thickening and Superior inner thinning had a significant positive correlation with axial length (p<0.05). In moderate categories, Fovea minimum, Fovea, Superior inner, Nasal inner, Inferior inner were positively correlated with axial length (p<0.05). In mild myopic eyes, temporal inner and inferior inner were significantly correlated with axial length (p< 0.05). In high myopia though there was increase in thickness of foveae minimum and fovea and thinning of inner and outer macular thickness there was no statistical significance correlation between axial length and macular thickness [Table/Fig-4].
Discussion
In previous studies done by Wakitani et al., [12] and Xie et al., [13] have postulated that the increase in the axial length of myopia causes mechanical stretching of the sclera in the posterior pole. This causes traction of vitreous on the fovea in the myopic eyes. Thus the increase in the foveal thickening with increasing degree of myopia can be an early sign of vitreoretinal traction. This incomplete vitreous traction in the myopic eyes may be associated with retinal detachment, myopic traction maculopathy and foveoschisis [14] . Springer and Hendrickson have explained the reason for increased foveal thickness in experimental animal models. They explained that the absence of vasculature in the foveal area may lead to foveal pit which is deformable in response intraocular pressure and ocular growth induced retinal stretch [15] . The parafoveal region being more elastic undergoes stretching and peripheral thinning.
Our study showed that the thickness of foveae minimum in high myopia was greater when compared to moderate myopia with a statistically significant value p<0.05 (p= 0.028). Also the thickness of fovea in the high myopia group increased compared to the moderate and mild myopia groups. This suggests that the significance of increase in foveal thickness with progression of myopia. This was similar to the study done by Xie R et al., which showed that the minimum and average foveal thickness was similar in emmetropia and low myopia groups but increased in high myopia groups [13] . Also, in a study by Choi et al., [16] showed that as the level of myopia increased the thickness of fovea also increased, while the peripapillary retinal nerve fibre layer decreased. But the correlation of inner and outer macular thickness between the mild, moderate and high myopia were not statistically significant. This suggests that the inter group difference in the thickness of inner and outer macula did not differ significantly in various degree of myopia. This was similar to the study done by Lim et al., [17] which showed that the average macular retinal thickness did not significantly vary between various degrees of myopia.
On comparing the axial length between the degrees of myopia, the high myopia showed greater axial length compared with moderate myopia, also the moderate myopia was significantly greater than mild myopia. The statistical significance between the axial length of the three groups shows a significant p-value (p=0.001). This suggests that the axial length increases with increasing degree of myopia. The degree of myopia and elongation of globe are associated with thinning of most areas of perifovea was found in a study by oathman SF et al., [18] .
Also, we compared the relation of axial length with various regions of macular thickness in the total myopic patients. There was a positive correlation of axial length with the foveae minimum, fovea and superior inner quadrant of the macula with a significant value of p<0.05. Similarly in moderate myopia the fovea minimum, fovea, and superior inner, nasal inner, inferior inner regions and in mild myopia the temporal and inferior inner regions of macula correlated significantly with the axial length. This suggests the influence of axial length over macular thickness in myopia. This correlates with the study done by Lam et al., in which minimum foveal thickness increased with axial length [14-19] . Similarly, Hwang et al., [20] also found that in healthy young myopic eyes showed thinner macular thickness, lower macular volume and thicker foveal thickness were associated with longer axial length. In our study we found there was no significant correlation of macular thickness with axial length in high myopia groups. This could be attributed to the small sample size of high myopia compared with moderate and mild myopia.
Macular region divided into 3 rings centred on fovea
Comparision of various regions of macula with degree of myopia
| Regions In Macula | Mild | Moderate | High | p-Value |
|---|
| Foveae Minimum | 171.4 ±18.1 | 165.5±21.2 | 178.7±26.4 | p = 0.028 |
| Fovea | 197.3±23.2 | 194.0±24.0 | 205.1±21.0 | p = 0.086 |
| Inner Macula Superior | 269±26.8 | 271.7±23.9 | 272.4±17.2 | p = 0.803 |
| Temporal | 261±25.9 | 260.0±19.2 | 261.5±22.1 | p = 0.048 |
| Inferior | 272.2±23.0 | 269.6±26.1 | 266.9±20.3 | p = 0.599 |
| Nasal | 267.3±26.1 | 267.1±26.1 | 264.9±20.5 | p = 0.889 |
| Outer Macula Superior | 281.6±21.9 | 272.5±26.5 | 273.5±25.7 | p = 0.182 |
| Temporal | 260.9±26.0 | 255.5±22.3 | 253.0±27.2 | p = 0.351 |
| Inferior | 273.2±28.8 | 268.5±44.3 | 267.7±33.1 | p = 0.283 |
| Nasal | 288.5±21.5 | 283.0±20.2 | 284.5±25.9 | p = 0.512 |
Comparison of axial length between three categories
| S. No | Category | Eyes n | Mean ±SD | ANOVA ‘F’ | Significance | Comparison of significance |
|---|
| 1 | High | 39 | 26.7±0.97 | 92. 921 | p=0.001 | 1&2=S |
| 2 | Moderate | 43 | 24.6±0.81 | 2&3=S |
| 3 | Mild | 43 | 23.5±0.81 | 3&1=S |
the mean axial length of high degree myopia 26.7±0.97 was statistically very highly significant with the other two categories such as Moderate (24.6±0.81) and mild (23.5±0.81). Similarly the other two categories were also very highly statistically significantly differed with each other (p<0.001).
Relationship between axial length with the macular thicknesses of three categories of myopia and total myopia
| Axial length correlation with Macular thickness | High n= 39 | Moderate n=43 | Mild n=43 | Total n=125 |
|---|
| R | Sig.(p=) | R | Sig.(p=) | R | Sig.(p=) | R | Sig.(p=) |
|---|
| Foveae Minimum | .086 | 0.061 | .366 | 0.016 | -.041 | 0.796 | .196 | 0.028 |
| Fovea | .229 | 0.160 | .454 | 0.002 | .171 | 0.273 | .288 | 0.001 |
| Temporal inner | .072 | 0.664 | .249 | 0.108 | .349 | 0.022 | .145 | 0.106 |
| Superior inner | .024 | 0.887 | 0.494 | 0.001 | .180 | 0.247 | .192 | 0.032 |
| Nasal inner | .108 | 0.514 | .535 | <0.001 | .223 | 0.150 | -.153 | 0.092 |
| Inferior inner | .097 | 0.558 | .420 | 0.005 | .340 | 0.026 | .110 | 0.220 |
| Temporal outer | -.045 | 0.784 | .075 | 0.634 | .043 | 0.783 | -.085 | 0.345 |
| Superior outer | -.134 | 0.416 | .155 | 0.322 | -.064 | 0.684 | -.106 | 0.240 |
| Nasal outer | -.057 | 0.731 | 0.218 | 0.159 | .046 | 0.769 | -.018 | 0.841 |
| Inferior outer | .060 | 0.719 | -.109 | 0.487 | -.080 | 0.609 | -.075 | 0.407 |
In high myopia eyes none of the macular thicknesses, either positively or negatively correlated with axial length (p>0.05). in moderate categories, foveae minimum, fovea, superior inner, nasal inner, inferior inner were significantly positively correlated with axial length (p<0.05). in mild myopia eyes, temporal inner and inferior inner were significantly positively correlated with axial length (p<0.05). in respect of all myopia eyes, foveae minimum, fovea and superior inner had significantly positively correlated with axial length (p<0.05)
Limitations
The limitations of our study are other confounding factors such as age, gender, ethnic groups which affects the retinal thickness which was not studied in detail which requires further detailed evaluation. Also other ocular parameters, such as anterior chamber depth, lens thickness, corneal curvature, vitreous length which are associated with myopic changes were not evaluated in this study. In the present study only a small group of subjects were included , hence detailed evaluation of contributing factors and myopic associations were not evaluated in depth, which calls for further studies on a large scale of myopic Indian population.
Conclusion
Our study showed that the minimum foveal thickness increases with myopic progression and positive correlation of axial length with foveae minimum and fovea. Understanding the mechanism and factors affecting the structural changes of a myopic eye helps in the development of therapeutic strategies. Since there is no current treatment for reversing the structural changes of a myopic eye the goal should be aimed at preventing the progression of myopia. Factors such as refractive correction, use of bifocal lenses for accommodative lag, adequate lighting while reading and outdoor physical activity should be made aware among parents and young people as these prevent the progression of myopia. Use of progressive additional lens (PALs) had shown to slow down the progression of myopia in children with accomodative lag by providing clear retinal images. Young myopes should be encouraged to participate in screening programmes and investigations like OCT as they are helpful in early detection and interpretation of macular changes.
the mean axial length of high degree myopia 26.7±0.97 was statistically very highly significant with the other two categories such as Moderate (24.6±0.81) and mild (23.5±0.81). Similarly the other two categories were also very highly statistically significantly differed with each other (p<0.001).
In high myopia eyes none of the macular thicknesses, either positively or negatively correlated with axial length (p>0.05). in moderate categories, foveae minimum, fovea, superior inner, nasal inner, inferior inner were significantly positively correlated with axial length (p<0.05). in mild myopia eyes, temporal inner and inferior inner were significantly positively correlated with axial length (p<0.05). in respect of all myopia eyes, foveae minimum, fovea and superior inner had significantly positively correlated with axial length (p<0.05)
[1]. S-M Saw, J Katz, OD Schein, S-J Chew, T-K Chan, Epidemiology of myopiaEpidemiol Rev 1996 18(2):175-187. [Google Scholar]
[2]. BJ Curtin, The myopi: Basic science and clinical management 1985 PhiladelphiaHarper and row [Google Scholar]
[3]. B Curtin, Topics to be considered when establishing standards for clinical myopia studiesActa ophthalmol suppl 1988 185:61-62. [Google Scholar]
[4]. JE Gwiazda, Accommodation and Related Risk Factors Associated with Myopia Progression and Their Interaction with Treatment in COMET ChildrenInvest Ophthalmol Vis Sci 2004 45(7):2143-51. [Google Scholar]
[5]. T N Ursekar, Classification, etiology and pathology of myopiaIndian J Ophthalmol 1983 31:709-11. [Google Scholar]
[6]. SM Saw, G Gazzard, EC Shih-Yen , WH Chua, Myopia and associated pathological complicationsOphthalmic Physiol Opt 2005 25(5):381-91. [Google Scholar]
[7]. CKS Leung, S Mohamed, KS Leung, CYL Cheung, SLw Chan, DKy Cheng, Retinal Nerve Fiber Layer Measurements in Myopia: An Optical Coherence Tomography StudyInvest Ophthalmol Vis Sci 2006 47(12):5171-76. [Google Scholar]
[8]. KD Schweitzer, D Ehmann, R García, Nerve fibre layer changes in highly myopic eyes by optical coherence tomographyCan J Ophthalmol J Can Ophtalmol 2009 44(3):e13-6. [Google Scholar]
[9]. TC Burton, The influence of refractive error and lattice degeneration on the incidence of retinal detachmentTrans Am Ophthalmol Soc 1989 87:143 [Google Scholar]
[10]. Sharples E Optical Coherence Tomography findings in High MyopiaOptician 2005 230 [Google Scholar]
[11]. A Chan, JS Duker, TH Ko, JG Fujimoto, JS Schuman, Normal macular thickness measurements in healthy eyes using stratus optical coherence tomographyArch ophthalmol 2006 124:193-98. [Google Scholar]
[12]. Y Wakitani, M Sasoh, M Sugimoto, Macular thickness measurements in healthy subjects with different axial lengths using optical coherence tomographyRetina 2003 23:177-82. [Google Scholar]
[13]. T Xie, XT Zhou, F Lu, M Chen, A Xue, S Chen, Correlation between Myopia and Major Biometric Parameters of the Eye: A Retrospective Clinical studyOptometry and Vision Science 2009 86:503-08. [Google Scholar]
[14]. DSC Lam, KS Leung, S Mohamed, WM Chan, MS Palanivelu, CYL Cheung, Regional Variations in the Relationship between Macular Thickness Measurements and MyopiaInvest Ophthalmol Vis Sci 2007 48(1):376-82. [Google Scholar]
[15]. AM Dubis, JT McAllister, J Carroll, Reconstructing foveal pit morphology from optical coherence tomography imagingBr J Ophthalmol 2009 93(9):1223-27. [Google Scholar]
[16]. SW Choi, SJ Lee, Thickness changes in the fovea and peripapillary retinal nerve fiber layer depend on the degree of myopiaKorean J Ophthalmol 2006 20(4):215-19. [Google Scholar]
[17]. MCC Lim, Use of Optical Coherence Tomography to Assess Variations in Macular Retinal Thickness in MyopiaInvest Ophthalmol Vis Sci 2005 46(3):974-78. [Google Scholar]
[18]. SF Othman, FA Manan, Macular thickness as determined by optical coherence tomography in relation to degree of myopia, axial length and vitreous chamber depth in Malay subjectsClinical and Experimental Optometry 2012 95(5):484-91. [Google Scholar]
[19]. E Harb, L Hyman, M Fazzari, J Gwiazda, W Marsh-Tootle, Factors Associated with Macular Thickness in the COMET Myopic CohortOptom Vis Sci 2012 89(5):620-31. [Google Scholar]
[20]. HY Hwang, YY Kim, Macular thickness and volume of myopic eyes measured using spectral-domain optical coherence tomographyClinical and Experimental Optometry 2012 95:492-98. [Google Scholar]