Background: The pattern of drainage in the right posterior lobe of liver varies considerably. The knowledge of this variation is very important while performing various surgeries on the right posterior lobe.
Aim:A study was conducted to see the variations in the pattern of drainage of posterior segment of the right lobe of liver. The aim was to see the variations of right hepatic vein and small accessory hepatic veins draining the posterior segment, the presence of which led to modifications in drainage of posterior segment.
Material and Methods: Sixty formalin fixed adult human liver specimens were dissected manually.
Results: According to the pattern of drainage of tributaries of right hepatic vein, the right hepatic vein was classified into type I, type II, type III and type IV. According to presence of inferior right hepatic vein, three types of drainage of posterior lobe were seen: Type I, (76.36%) right hepatic vein was large, draining wide area of posterior segment. A small inferior right hepatic vein drained the small area of posterior segment. In Type II, (19.92%) both right hepatic and inferior right hepatic veins were medium sized draining the posteroinferior segment of the right lobe concomitantly. In Type III, (32%) accessory veins, the middle right hepatic vein drained the posterosuperior (VII) as well as the posteroinferior (VI) segment. In one specimen, there were numerous middle right hepatic veins draining the right posterior segment. The knowledge of anatomic relationship of veins draining right lobe, is important in performing right posterior segmentectomy.
Conclusion: For safe resection of the liver, the complex anatomy of the distribution of the tributaries of the right hepatic vein and the accessory veins have to be studied prior to any surgery done on liver.
Introduction
The surgical treatment of neoplastic and traumatic lesions of the liver by respective measures has increased in frequency and magnitude during recent years. There is considerable variation in the pattern of drainage in the posterior segment of liver. A comprehensive knowledge of these variations is mandatory for the successful segmentation and resection of the posterior segment of liver. These variations are due to the diversity in branching pattern of the right hepatic vein (RHV) and presence of accessory veins, the middle right hepatic vein (MRHV) and the inferior right hepatic vein (IRHV) [1]. The present study was conducted to see the variations of RHV and the frequency and variations of IRHV and MRHV. The knowledge of the anatomic relation of these veins is important during right hepatic segmentectomy [2]. The evaluation of the variations of the drainage of the posterior segment is very important as it can help in retaining greater amount of liver during right hepatectomy specially in patients with poor liver function [3].
According to Longmire, isolation and division of the hepatic veins was done before transection of the parenchyma of the liver. Clamping and packing of the veins followed by definitive closure after transection of the parenchyma could control the bleeding due to unforeseen complications [4]. Nakamura recommended that it is crucial to close the veins with running suture after transecting them with vascular clamps. This also helps in avoiding the slipping of the ligature. He further recommended that it was necessary for the transplantation of the liver because a stump of atleast 1cm should be left for the proper ligation of the hepatic veins. This implicates that preoperative evaluation of the length of the tributary free part and also the diameter of the veins is of great importance [5].
It has been reported that massive bleeding can occur if the hepatic veins were lacerated leading to cardiac arrest or air embolism [6]. The ligation of the veins prior to the transection of liver can prevent the pushing of cancer cells into the veins and will reduce bleeding. So, the knowledge of the variable and substantial diameters of these veins is imperative.
Materials and Methods
The study was conducted on 60 specimens of adult human cadaveric livers. The livers were removed from cadavers fixed by the perfusion of 10% formalin solution through the femoral artery and were preserved for one week. They were dissected from the visceral surface in order to maintain the original shape of the liver. The hepatic veins were identified. They run along the borders of the segments of liver. The right lobe of liver is divided into anterior and posterior sectors. RHV runs between anterior and posterior sectors [7-9]. RHV and the accessory hepatic veins draining the posterior segment were dissected from end to end and examined. The conduit of RHV and its tributaries were traced in the posterior segment. Any variation in the drainage of posterior segment was noted. Due to thick vascular sheath over the vessels, the internal diameter was usually much smaller than expected from the external appearance. Proper photographs were difficult to obtain due to damage to the veins during removal of the tough connective tissue over the veins. The veins were cut at the point of ramification and vascular lumen was viewed to confirm the pattern of branching. Caliber and distances of ramifications of RHV and accessory hepatic veins were taken (in millimetres) from their confluence into the IVC, till the first order tributaries using vernier callipers or calibrated divider. Diameter of the main trunk of RHV was taken at the point just before it was joined by the first order tributary.
Special care was taken to see if RHV had any tributary within one cm from the IVC because stump of atleast one centimetre is mandatory for ligation during liver transplantation [4,5].The tributaries which had diameter more than 2mm were taken into account. RHV was observed along the whole length along with its tributaries to note the drainage area of the posterior segment. The posterior segment was identified on the basis of the alignment of RHV as it has been seen that the peripheral course of hepatic veins appears to be the most important cue for the identification of the portal segments. RHV runs in between the anterior and posterior sectors i.e. anterosuperior and posterosuperior and between the anteroinferior and posteroinferior segments [7,8]. Other accessory veins, IRHV and the MRHV were studied as these veins appeared to drain significant areas in the posterior segment of the right lobe of liver. The IRHV was seen draining the right posteroinferior segment (segment VI) and the MRHV was seen draining the posterosuperior (segment VII). The frequency of the veins by which they occurred in the specimens was noted and their calibres were measured. The accessory veins exceeding a calibre of 5mm were taken into account.
Results
The tributaries of RHV were identified by observing the areas drained by them. One tributary of RHV was identified draining a significant area of the right posterosuperior segment. The vein was named the right posterosuperior vein. Another vein the right anterosuperior vein was seen draining the right anterosuperior segment of the right lobe. This vein was joining the RHV at a distance less than 1cm from the IVC in many specimens. Before surgeries of the posterior segment, examination of any tributary of RHV within 1cm from IVC is imperative because injury to RHV during its transection could cause fatal haemorrhage [4,5]. A stump of at least 1cm is necessary for safe transection of the RHV. RHV was classified into four types according to distance of confluence of its tributaries from the IVC.
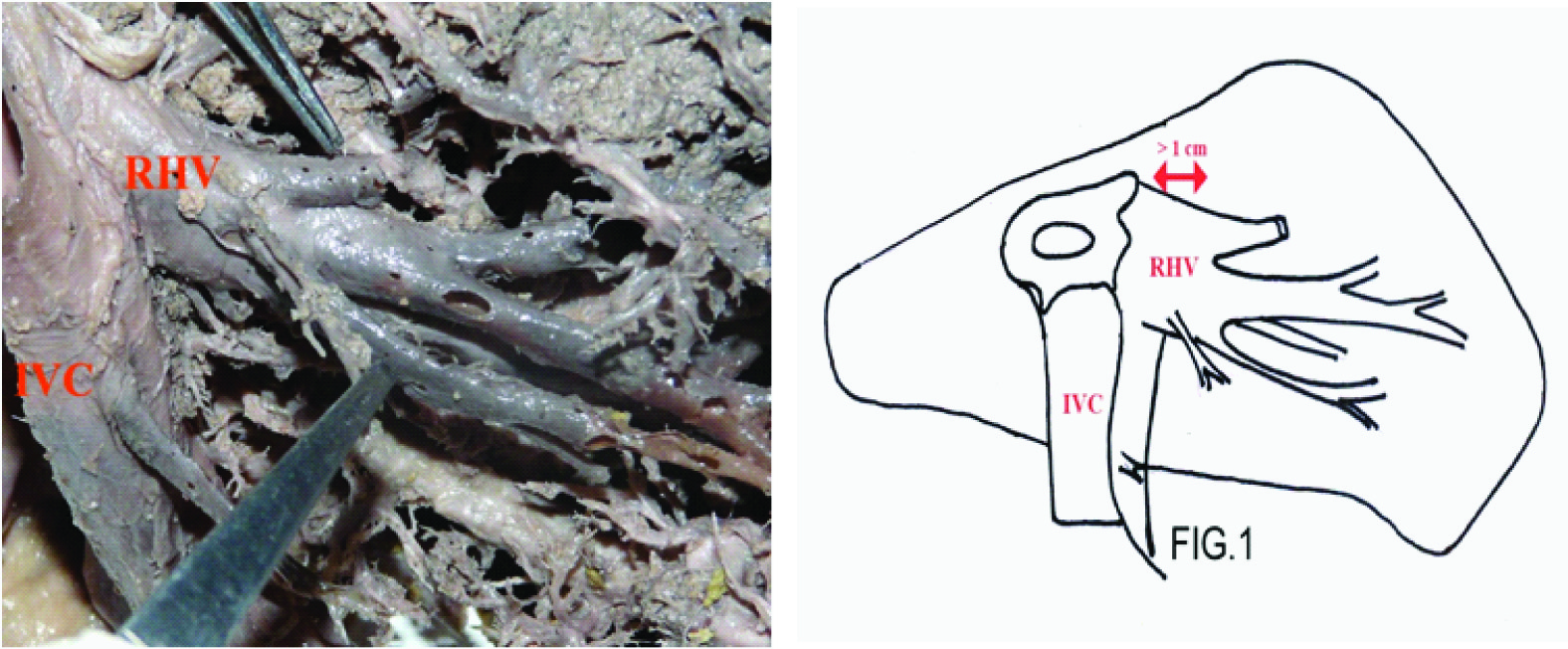
In Type I, the tributaries were joining the RHV at a distance of more than 1cm from the IVC. Such type of distribution was found in 35 cases. Further this type was sub-classified into types Ia, Ib and Ic. In Type Ia, 32 cases (53.12%), no tributary was seen draining into the RHV within 1cm from the IVC [Table/Fig-1]. Other tributaries of more than 2mm in diameter entered the RHV along the whole length.
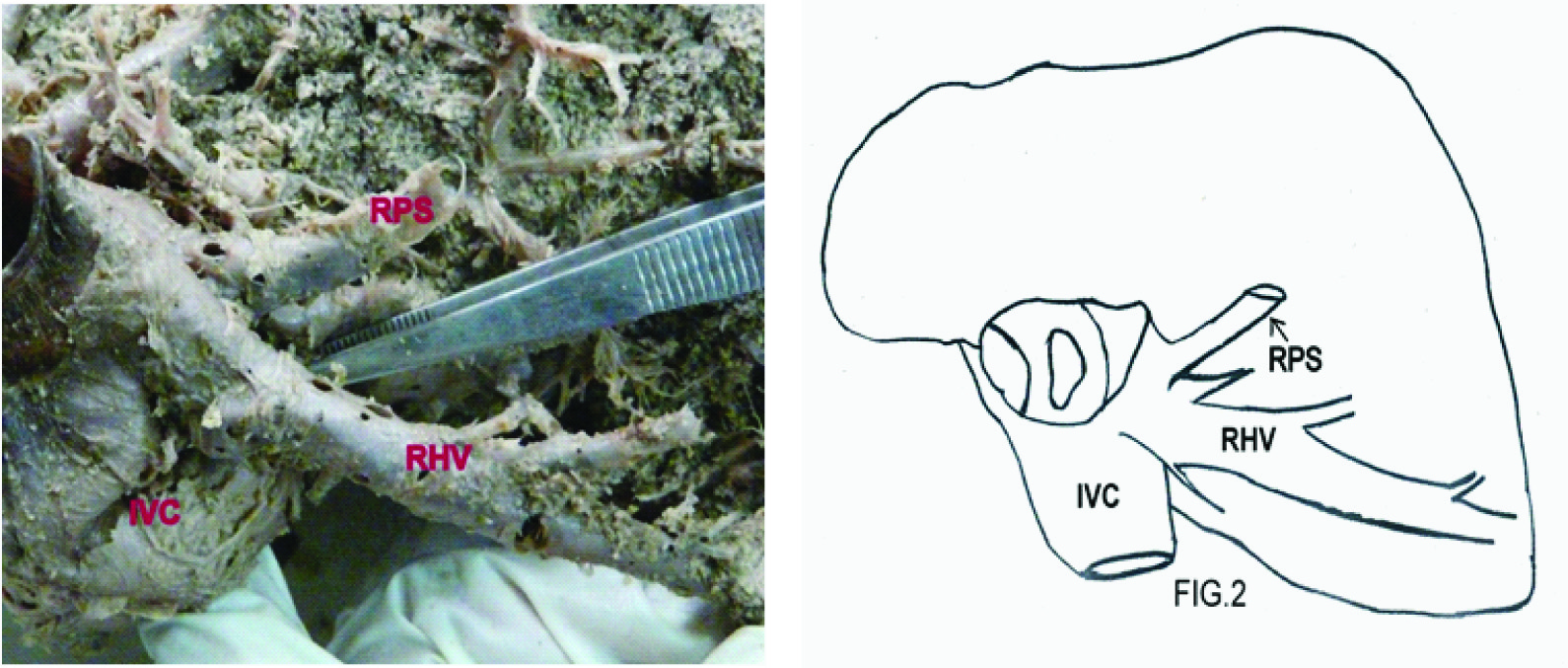
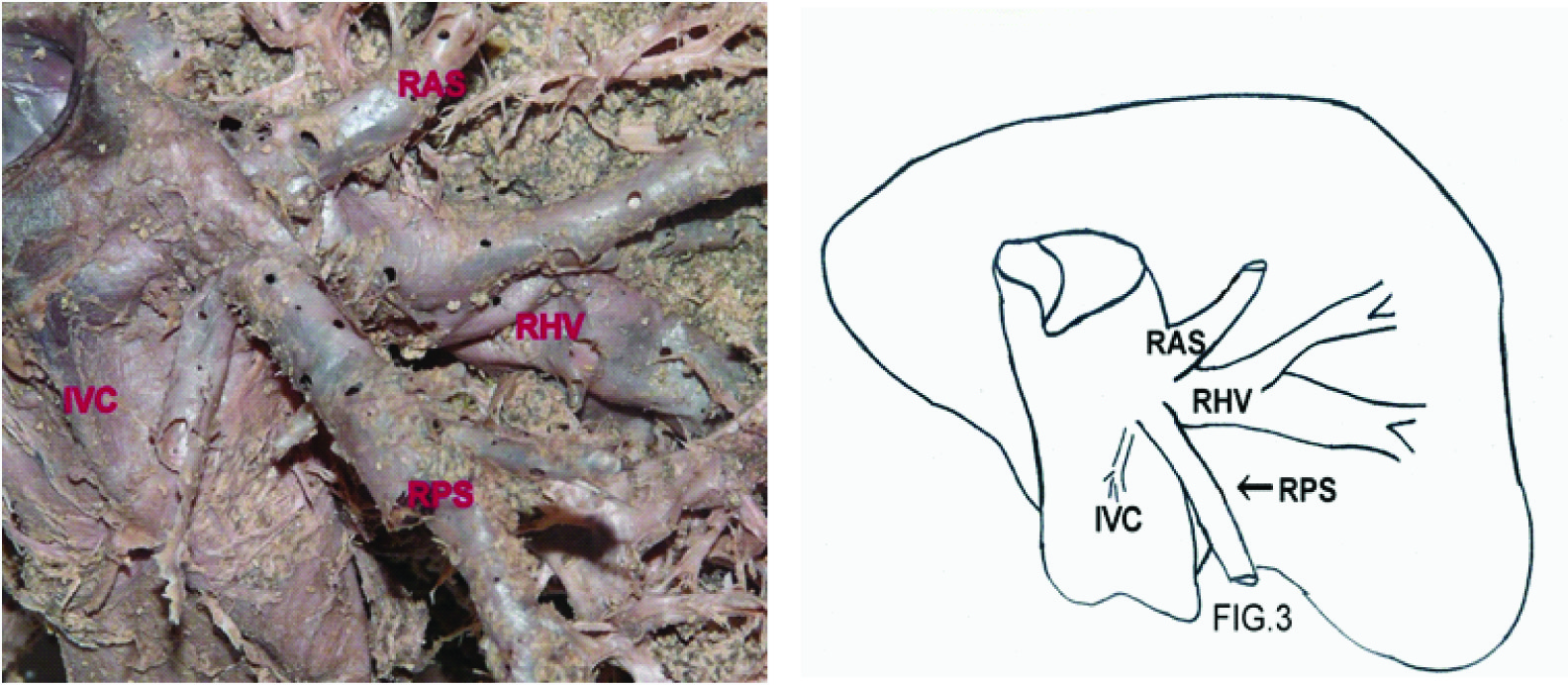
Type Ib, consisting of two cases (3.32%), presented with no tributaries of RHV within 1cm from IVC but the right posterosuperior vein was seen flowing directly into IVC close to RHV [Table/Fig-2]. In this type, the size of the RHV appeared to be reduced. In type Ic, right posterosuperior vein and right anterosuperior vein entered the IVC close to each other [Table/Fig-3]. Instead of joining the RHV, they directly entered the IVC. This type was seen only in one of the livers (1.66%).
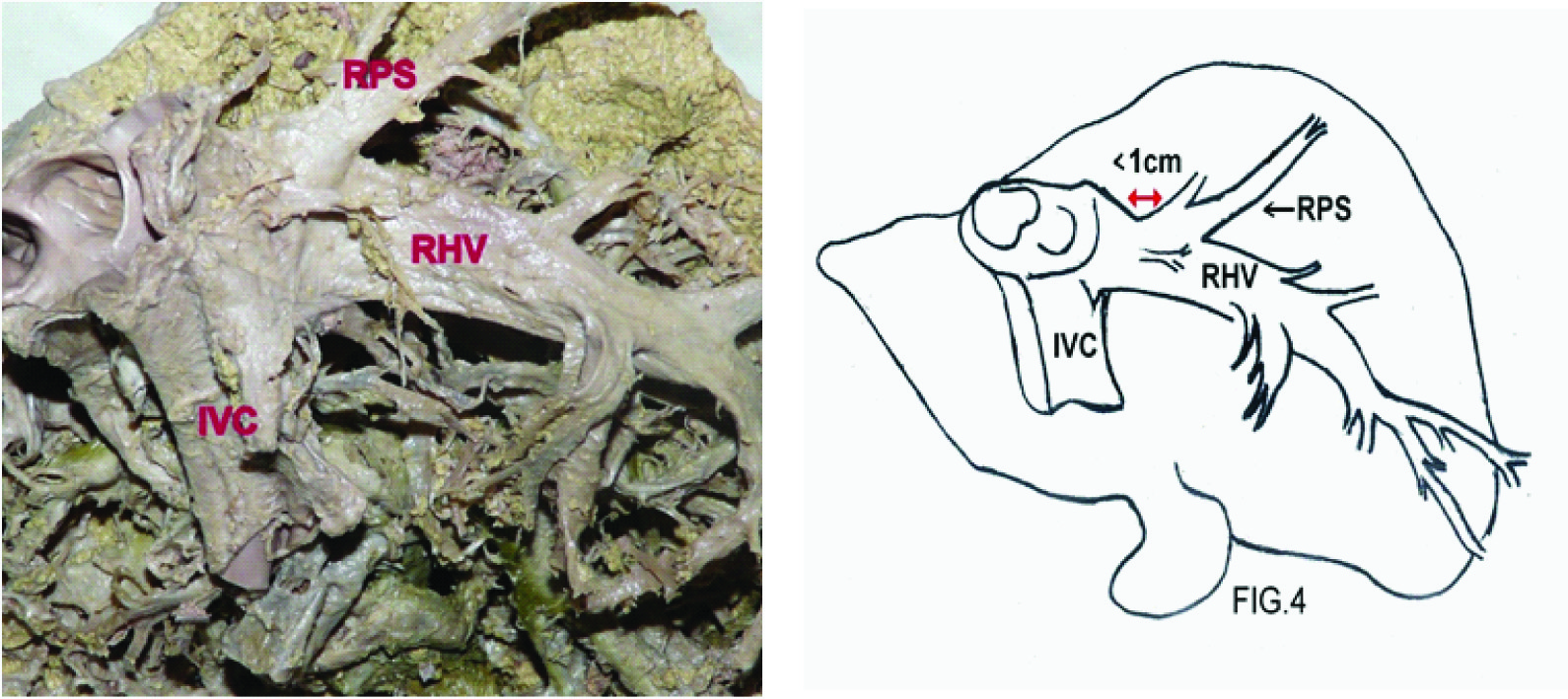
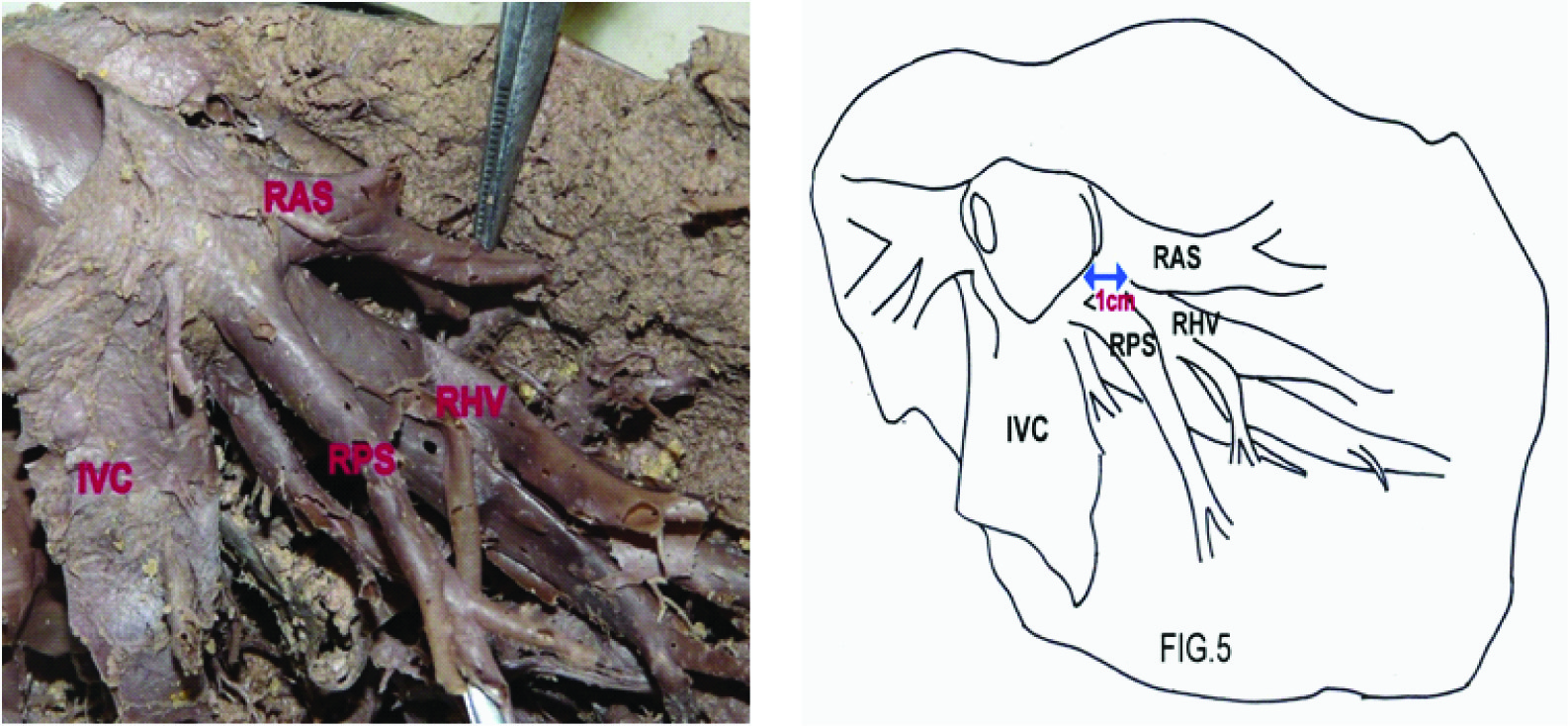
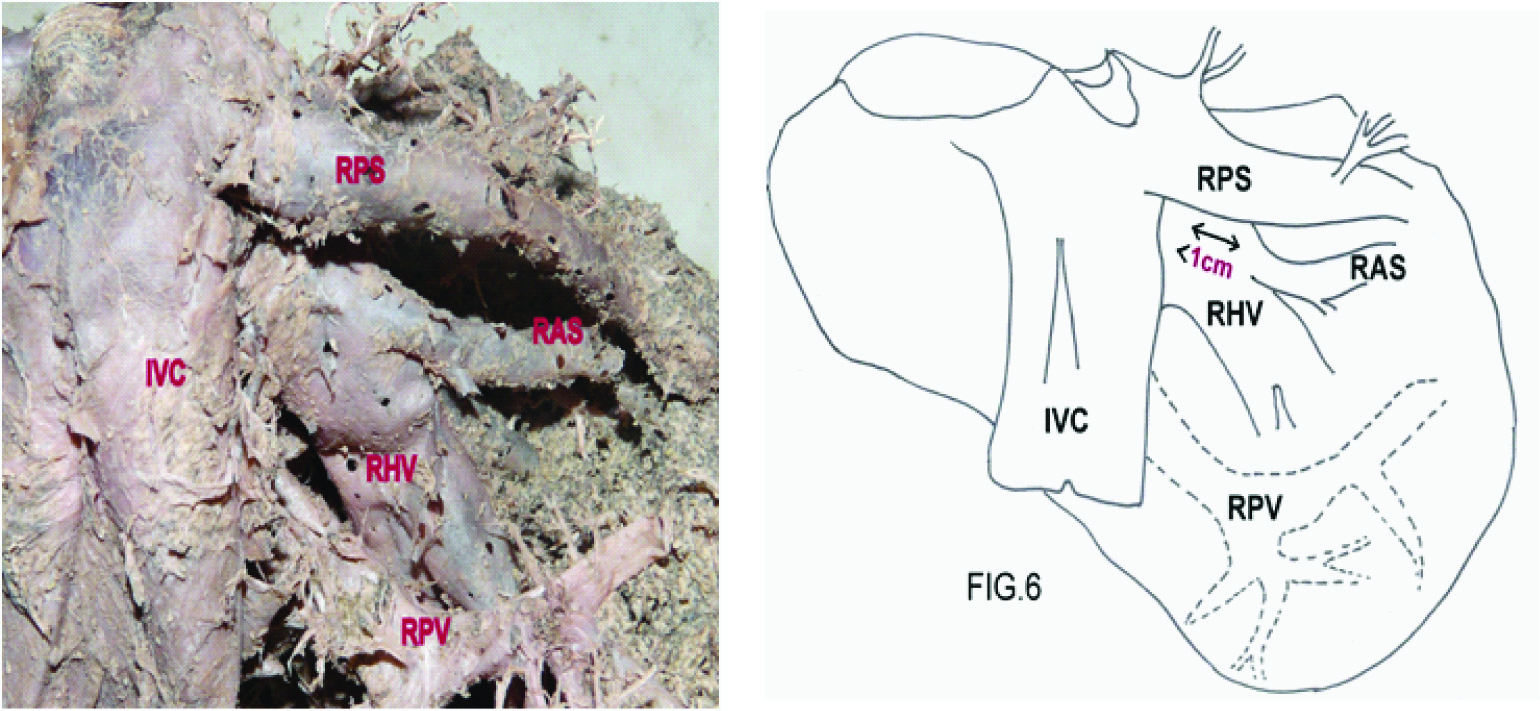
In type II, RHV had tributaries within a distance of 1cm from the right hepatocaval confluence. This type was subtyped into type IIa and IIb. Type IIa consisted of cases where the right posterosuperior vein drained into the RHV within 1cm from the IVC [Table/Fig-4]. This type was seen in 10 cases (16.6%). Type IIb consisted of 4 cases (6.64%), which had right anterosuperior vein flowing into the RHV within 1cm from the IVC. Type III consisting of 4 cases (6.64%) had both right posterosuperior and right anterosuperior veins within 1cm [Table/Fig-5]. Type IV was formed when right posterosuperior vein entered directly into the IVC with right anterosuperior draining into RHV within a distance of 1cm from the IVC or when right anterosuperior vein entered into the IVC and right posterosuperior drained into RHV at distance less than 1cm [Table/Fig-6]. This type was seen in 7 cases (11.66%).
It was observed that the drainage of the right posterior segment is influenced by the presence of inferior right hepatic vein (IRHV). Knowledge of the presence of this accessory vein is important during complex surgeries in the right posterior segment of liver [4]. This vein joins the IVC inferior to the opening of RHV into the IVC. The IRHV was always located close to the visceral surface of the liver. The diameter of the RHV ranged from 9 to 27 mm, with an average of 14.31 ± 3.72mm. The diameter of IRHV ranged from 8 to 15mm, with an average of 10 ± 1.85mm. The distance between the RHV and the IRHV ranged from 23 to 53 mm, 32.23 ± 6.6469mm. Along with IRHV, numerous other accessory veins were sometimes present between the inflows of RHV and IRHV into the IVC. These veins were referred to as middle right hepatic veins (MRHV).
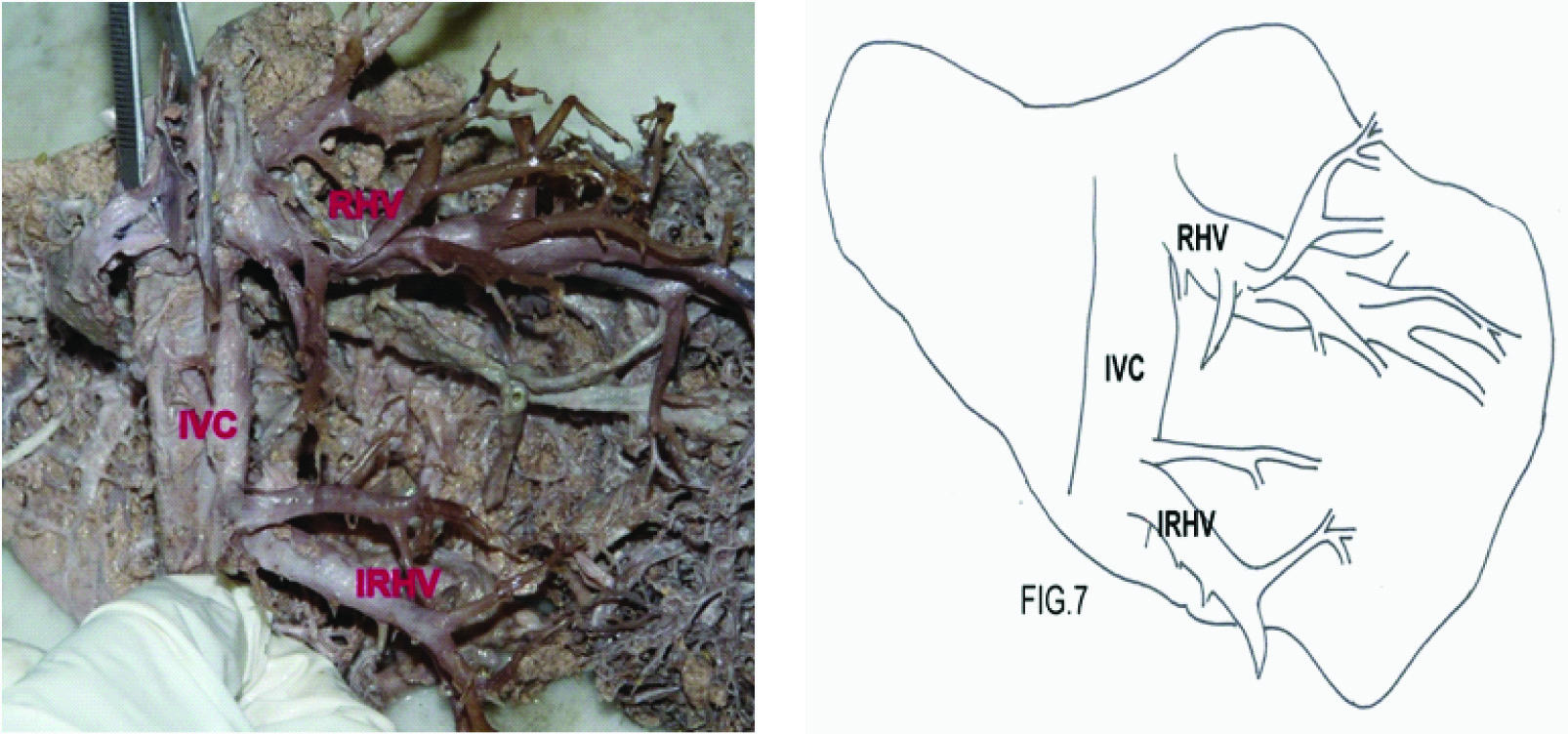
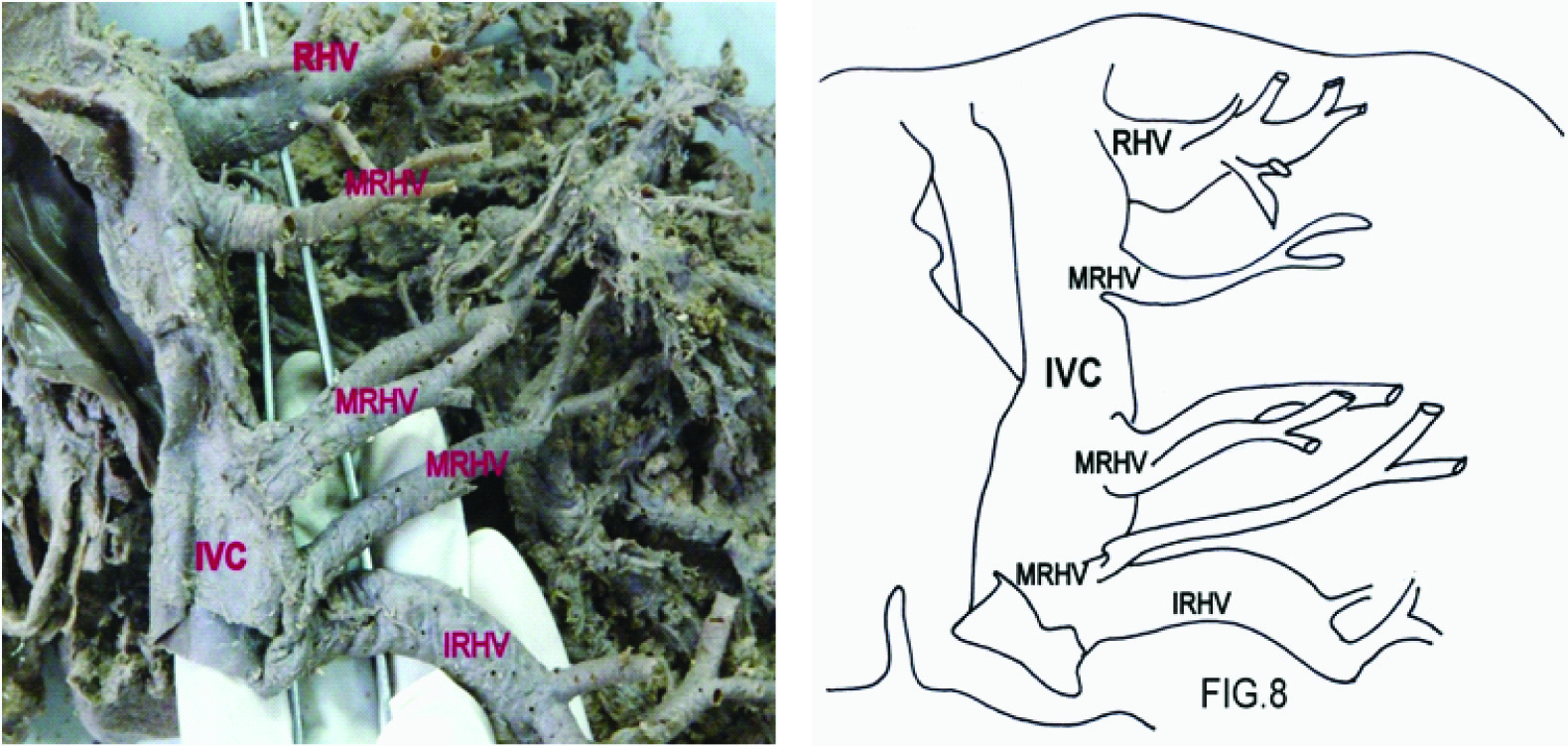
The diameter of RHV varied due to presence of the IRHV and MRHV. According to the presence of these veins, the drainage of the posterior lobe was classified into three types. In the Type I, 76.36% (n=46), i.e. in almost three-fourths of the livers dissected, the RHV was large and drained a wide area of the posterior segment of the right lobe while the IRHV drained a very small area of the posteroinferior segment [Table/Fig-7]. In Type II, 19.92% (n=12), the size of RHV was smaller than in type I and the size of the IRHV was similar to RHV. The areas drained by them were comparable. Type III (n=2), 3.32%, had other accessory veins along with IRHV, i.e. MRHV draining the posterosuperior (VII) as well as the posteroinferior (VI) segments [Table/Fig-8]. The diameter of MRHV ranged from 6 to 8mm, with an average of 7.3 ± 1.154mm. In these cases, the RHV had a smaller diameter which ranged from 9 to 10mm only. In one of the two livers, three large middle right hepatic veins (MRHV), one having diameter 6mm and the other two having diameter 8mm were seen. The MRHV usually drained the right posterosuperior segment of the liver and IRHV drained the right posteroinferior segment [Table/Fig-9].
Discussion
The RHV was studied in relation to venous drainage of right hepatic lobe and classified into 4 types [Table/Fig-10]. Other veins draining the right lobe of liver, the IRHV and MRHV were also studied and the territory of their drainage observed. Majority of the previous studies were done by corrosion cast, colour Doppler and ultrasound.
In the present study, the tributary free part of RHV was >1cm in 53.12% livers (Type Ia). Similar findings have been reported by Nakamura et al., in 61.4% cases [5]. It was reported in 53% cases by Chevallier 1988 and in 77% cases by Cecchis et al., [10,11]. Difference in the number of cases with the length of the tributary free part of more than 1cm could be due to difference in number of specimens in previous studies as compared to the present study. In some of the specimens, where the RHV had no tributaries within 1cm from the IVC, either the right posterosuperior vein or the right anterosuperior vein drained into the IVC very close to the inflow of the RHV into the IVC (Types Ib, Ic). The hepatic veins were buried inside the liver except for a short segment of the confluence of the veins with the inferior vena cava. So these veins have to be taken into special account, as most grave type of hepatic trauma during surgeries is laceration of the hepatic veins with avulsion of the inferior vena cava. So in our opinion, the knowledge of these subtypes Ib and Ic is important while performing right posterior segmentectomy. Type I of Nakamura corresponds to Ia of present study [Table/Fig-10]. Type Ib and Ic as described in present study have not been reported by any researcher in the available literature till date. Special care should be taken to ligate the tributaries which are draining independently into the IVC from the right posterosuperior and the right anterosuperior segments [Table/Fig-10].
In rest of the specimens, we found that either the right anterosuperior vein or the right posterosuperior vein or both were draining into the RHV within a distance of 1cm from the hepatocaval confluence. In these cases the RHV should be ligated under wide field after the liver is transected and if seen in the hepatic venography, should not be ignored at the time of surgery to avoid haemorrhage. The right anterosuperior vein and the right posterosuperior veins have to be evaluated carefully before surgery to establish if they are draining into the RHV or directly into the IVC.
Type IIa was found to be prevalent in 16.6% of the cases, which is close to that reported by Nakamura i.e. 15 (or 18%). Type IIb was seen in 6.64% of the cases while Nakamura, reported it to be 4 (or 4.8%). Another type, i.e. Type III appeared in 6.64% of our cases. It was found in 8.9% of cases in the study done by Nakamura. Type IV in our study was found in 11.66% cases. This is almost double the frequency reported by Nakamura [Table/Fig-10] . This difference in frequency could be explained by the fact that Nakamura included only those cases which had independent right posterosuperior vein flowing into IVC, with presence of right anterosuperior vein at a distance <1cm from IVC in their ‘type IV’. But in the present study, along with Nakamura’s type IV, we found another type in which right anterosuperior vein was draining into IVC independently while rig posterosuperior vein was seen flowing into RHV within one cm from IVC [Table/Fig-6]. These two types of variation have been included under type IV.
The accessory hepatic veins (≥5mm in diameter) draining the right posterior segment: the inferior right hepatic vein (IRHV) and middle right hepatic vein (MRHV) were studied. These veins have been named the “short hepatic vein” (SHV) in study done by Hata et al., [12] and are also mentioned in past by other workers (Hardy 1972, Gupta 1979) [13,14].
Embryological Basis for the Presence of the Right Posteroinferior Vein
There are various connections between the ductus venosus and the sinusoids of the liver in intra-uterine life. During the further development these sinusoids are absorbed and the connections also disappear. It can be hypothesized that at some places the connections between the ductus venosus and the sinusoids remain patent. This can be a reason for the presence of the posteroinferior and the right middle hepatic veins draining the posterior segment of the liver leading to separate opening in the IVC.
The MRHV was not always present but it was considered important in cases where drainage area was limited to one segment or a part of segment in the right lobe of liver as observed by Cecchis LD et al., [11]. It was observed that the diameter of RHV varied according to the presence or absence of the IRHV. In the livers where the RHV was large draining the right posterosuperior segment and small areas of posteroinferior segments, IRHV was small draining small area of the right posteroinferior segment [Table/Fig-9]. In contrast when IRHV of larger diameter was present, it was seen draining a wide area in the posterior inferior segment, it was associated with RHV of smaller diameter. Moreover, it seemed that both the veins had their own independent drainage areas. So it can be concluded that an increase in the diameter of IRHV was related with decrease in the diameter of the RHV. The diameter of RHV ranged from 9 to 27mm, 14.1±3.7mm [Table/Fig-11] and that of IRHV ranged from 8 to 15mm, 10±1.85mm [Table/Fig-12].
Large sized MRHV when present drained inferior part of the right posterosuperior segment. The diameter of MRHV was found to range from 6 to 8mm, 7.3±1.154mm. Comparison of the diameter of MRHV with that of previous studies is given in [Table/Fig-13]. The distance between of the opening of the RHV and the IRHV into the inferior vena cava was found to range from 23 to 53mm, 32.23 ± 6.6469mm. This distance was found to range from 23 to 60mm, (44 ± 10mm) in a study by Cecchis et al., [11]. It ranged from 3 to 5cm (average 3.7cm) in study done by Cheng et al., [1].
Preoperative evaluation of veins and the areas drained by them is very important during hepatic surgeries. The surgeries preserving the accessory veins during hepatectomies due to various causes could help in retaining a greater proportion of liver parenchyma than right hepatectomy. In other words substantial amount of liver could be preserved for patients. Xing X et al., also suggested that the posteroinferior area of the right lobe can be preserved along-with IRHV, even if entire RHV is resected during segmentectomy of segments VII and VIII in patients of primary liver cancer by preserving accessory veins [2]. Cheng YF et al., showed that the evaluation and knowledge of the accessory veins was important before performing a right subtotal hepatectomy with preservation of segment VI and segment V and with RHV resection [1]. Hirai I, also concluded in his study, that IRHV preserving hepatectomy can retain a greater proportion of liver parenchyma than right hepatectomy [3]. It has been suggested by Shimuzi A, that in cases where tumour infiltrated the main RHV trunk, partial segmentectomies could be useful instead of right hepatectomy, after studying the veins draining the posterior segments [15] So, during various types of hepatic resection surgeries, it is mandatory to have knowledge of the accessory veins present in the right lobe of liver and their drainage areas.
The anatomic relationship of the tributaries draining the right lobe, mentioned above is important in performing right posterior segmentectomy. A comprehensive knowledge of these veins is important before any procedure done on the right lobe of liver.
Type Ia has tributaries at distance >1cm from IVC. RHV= Right Hepatic vein. IVC= Inferior Vena cava
Type Ib has no ramifications within 1cm but one branch, i.e. the right posterosuperior (RPS) is seen draining directly into IVC. RPS = Right posterosuperior, RHV= right hepatic vein, IVC=Inferior vena cava
Type Ic has right anterosuperior (RAS) and right posterosuperior (RPS) flowing into IVC. No significant tributary draining the RHV within a distance of 1cm. RAS=right anterosuperior, RPS= right posterosuperior, RHV= right hepatic vein
Type IIa has right posterosuperior (RPS) coming from right posterosuperior segment flowing into RHV within distance 1cm. RPS=right posterosuperior, RHV=right hepatic vein
Type III has right anterosuperior (RAS) and right posterosuperior (RPS) draining into RHV within 1cm from IVC. RAS=right anterosuperior, RPS= right posterosuperior, RHV= right hepatic vein
Type IV has right posterosuperior (RPS) draining into inferior vena cava (IVC), right anterosuperior (RAS) draining into right hepatic vein(RHV) at <1cm from IVC. RPV= right portal vein
Type I shows RHV larger in calibre than IRHV. RHV= right hepatic vein, IRHV= inferior right hepatic vein
Type III shows numerous MRHV in between RHV and IRHV draining the posterior segment. The calibre of MRHV is similar to the RHV and IRHV. RHV= Right hepatic vein, MRHV= Middle right hepatic vein. IRHV= inferior right hepatic vein. IVC=Inferior vena cava
The pattern of drainage of posterior segment of right lobe
| Pattern | DRAINAGE | Cases (%) |
|---|
| Type I | RHV > RPI | 76.36% |
| Type II | RHV = RPI | 19.92% |
| Type III | RHV = RPI = MRHV | 3.32% |
Comparison of the types of RHV with literature
| Studies done | Types and percentages of RHV |
|---|
| Present study | Ia 53.12 | Ib 3.32 | Ic 1.66 | IIa 16.6 | IIb 6.64 | IIb 6.64 | IV 11.6 |
| Nakamura et al(1981)5 | I 51-61.4 | - | - | IIa 15-18 | IIb 4-4.8 | III 8-8.9 | IV 5-6 |
Comparison of diameter of RHV with previous Studies
| Studies Done | Min | Max | Mean ± SD |
|---|
| Present Study | 9mm | 27mm | 14.1 ± 3.7mm |
| Nakamura et al., [5] | 1.0cm | 2.5cm | 1.7 ± 0.5cm |
| Hata et al., [12] | - | - | 21.1mm(average) |
| L.D. Cecchis [11] | 0.7cm | 2.3cm | 1.5 ± 0.4cm |
| Hwang JW[16] | - | - | 8mm(average) |
Comparison of diameters of IRHV with previous studies
| Studies Done | Min | Max | Mean ± SD |
|---|
| Present Study | 8mm | 15mm | 10 ± 1.85mm |
| Nakamura et al.,[5] | 5mm | 18mm | - |
| Cheng YF[1] | 0.1cm | 0.8cm | 0.46cm(average) |
| L.D. Cecchis [11] | 0.4cm | 1.3cm | 0.8 ± 0.3cm |
| Hwang JW [16] | - | - | 6.2mm(average) |
Comparison of diameters of mrhv with previous studies
| Studies Done | Min | Max | Mean ± SD |
|---|
| Present Study | 6mm | 8mm | 7.3 ± 1.154mm |
| Cheng YF [1] | 0.1cm | 0.9cm | 0.34cm |
| L.D. Cecchis [11] | 0.4cm | 1.0cm | 0.6 ± 0.2cm |
Conclusion
We conclude that a very comprehensive knowledge of the varying patterns of the veins draining the posterior segment of the right lobe of liver is very important. In our study we found out many variations in the drainage system which should be studied carefully before any surgery on the liver to prevent any unforeseen complications. Precise knowledge might also help in preserving more of liver parenchyma.
[1]. YF Cheng, TL Huang, CL Chen, TY Chen, CC Huang, SF Ko, Variations of the middle and inferior right hepatic vein: application in hepatectomyJ Clin Ultrasound 1997 25(4):175-82. [Google Scholar]
[2]. X Xing, H Li, WG Liu, Clinical studies on inferior right hepatic veinsHepatobiliary Pancreat Dis Int 2007 6(6):579-84. [Google Scholar]
[3]. I Hirai, W Kimura, A Fuse, T Yamamoto, M Moriya, Evaluation of inferior right hepatic vein-preserving hepatectomy with resection of the superior right hepatic veinHepatogastroentrology 2001 53(70):516-20. [Google Scholar]
[4]. WP Longmire, TetracyclineTeratologyJr Hepatic resection. Advances in surgery 1974 VIIIChicagoBMPI [Google Scholar]
[5]. S Nakamura, T Tsuzuki, The surgical anatomy of the hepatic veins and the inferior vena cavaSurg gynae Obs 1981 152:43-50. [Google Scholar]
[6]. RD Brasfield, Major resection for malignant neoplasms of the liverAnn Surg 1972 176:171 [Google Scholar]
[7]. Ph.D. Woodburne, Goldsmith N.A., The surgical anatomy pertaining to liver resectionSurg Gynae Obstet 1957 105:310-18. [Google Scholar]
[8]. JE Healey, Vascular anatomy of the liverAnn NY Acad Sci 1970 170:8-17. [Google Scholar]
[9]. H Bismuth, Surgical anatomy and anatomical surgery of the liverWorld J surg 1982 6:3-9. [Google Scholar]
[10]. JM Chevalier, Anatomical basis of vascular exclusion of the liverSurg Radio Anat 1988 10:187-94. [Google Scholar]
[11]. LD Cecchis, M Hribernik, Ravnik D, EM Gadzjev, Anatomical variations in the pattern of the right hepatic veins: possibilities for type classificationJ Anat 2000 197:487-93. [Google Scholar]
[12]. F Hata, K Hirata, G Murakami, M Mukaiya, Identification of segments of VI and VII of the liver based on the ramification patterns of the intrahepatic portal and hepatic veinsClin Anat 1999 12:229-44. [Google Scholar]
[13]. KJ Hardy, The hepatic veinsANZ J Surg 1972 42:11-14. [Google Scholar]
[14]. SC Gupta, CD Guptan, The hepatic veins- A radiographic and corrosion cast studyInd J Med Res 1979 70:333-44. [Google Scholar]
[15]. A Shimuzi, A Kobayashi, T Yokoyama, T Nakata, H Motoyama, K Kubota, Hepatectomy preserving drainage veins of the posterior section for liver malignancy invading the right hepatic vein: an alternative to right hepatectomyAm J Surg 2012 204(5):717-23. [Google Scholar]
[16]. JW Hwang, KM Park, SC Kim, JH Lee, KB Song, YH Kim, urgical impact of an inferior right hepatic vein on right anterior sectionectomy and right posterior sectionectomyANZ J Surg 2014 84(1-2):59-62. [Google Scholar]