Intraventricular Haemorrhage as a Complication of Sub Mucosal Infiltration of Adrenaline
Shefali Gautam1, Sanjeev Kumar2, Ravi Prakash3, Vikas Mandhar4, Vinod Kumar Srivastava5
1 Senior Resident, Department of Anaesthesiology, King George Medical University, Lucknow, U.P, India.
2 Senior Resident, Department of General Surgery, King George Medical University, Lucknow, U.P, India.
3 Senior Resident, Department of Anaesthesiology, King George Medical University, Lucknow, U.P, India.
4 Senior Resident, Department of Anaesthesiology, King George Medical University, Lucknow, U.P, India.
5 Senior Resident, Department of Anaesthesiology, King George Medical University, Lucknow, U.P, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shefali Gautam, Senior Resident, Department of Anaesthesiology, King George Medical University, Lucknow, U.P-226003, India. E-mail : drshefalikgmu@gmail.com
Adrenaline infiltration is a widely used technique in head-neck and ENT surgeries to provide bloodless surgical field. However, use of adrenaline has been associated with hemodynamic changes which can be life threatening at times. Therefore, use of higher concentrations of adrenaline should be avoided and a close hemodynamic monitoring is required with use of other vasopressors. In the present case report, a young male died because of intraventricular bleeding caused by adrenaline infiltration during rhinoplasty.
Anesthesia, Rhinoplasty, Vasopressors
Case Report
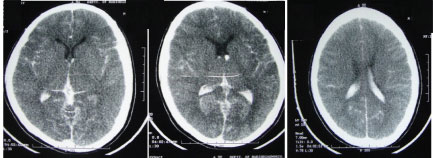
A 19-year-old male patient with weight 64 kg and height 165 cm, was scheduled for elective rhinoplasty under general anesthesia. Preanaesthetic examination was unremarkable. Patient was taken in OT and monitors were connected. Patient was premedicated with inj midazolam 1 mg and inj fentanyl 100 mcg. Patient was induced with inj. propofol 100 mg and inj. succinylcholine 100mg. Patient was intubated with a portex cuffed endotracheal tube of 8.5 mm internal diameter and oropharyngeal packing was done. Anesthesia was maintained with 60:40 N2O and oxygen, isoflurane and vecuronium. Surgery was started after proper cleaning and draping. Nasal mucosa was infiltrated with adrenaline solution in order to achieve bloodless surgical field. For this purpose one ampoule of adrenaline (1 ml of 1:1000) was added to 30 ml of normal saline to make final concentration of 1:30,000. 10 ml of this solution was injected in nasal mucosa over 30 seconds. The heart rate (HR) increased from 80/min to 120/min and blood pressure (BP) from 124/84 mmHg to 150/98 mmHg after 3 min of infiltration. Anaesthesia was deepened with 30 mg of propofol. The BP and HR returned to baseline after 10 min and surgery was started. After 20 min of commencement of surgery, profuse bleeding started from surgical site due to some unidentified vascular injury. The HR reached to 170/min and BP dropped to 90/60 mmHg. Inhalational agent was stopped and patient taken on 100% oxygen. Patient was resuscitated with intravenous fluids. In an attempt to control bleeding, surgeon used adrenaline soaked gauge piece to pack the surgical site. The same solution which was used for infiltration was used for soaking gauge piece. Soon after this, heart rate and blood pressure rose to 190/min and 240/120 mmHg, respectively and showed sustained elevated reading of HR and BP. A 40 mg bolus of propofol was given to control the rise in HR and BP. After 10 min, BP dropped to 76/44 mmHg with HR 180/min and nor epinephrine infusion was started. But BP was not improved and became non recordable. ECG showed Ventricular tachycardia. CPR was started and DC shock monophasic of 360 Joule was given. After 5 minutes of CPR, ECG showed normal sinus rhythm with HR 110/min, BP 105/76 mmHg on vasopressor support. Chest was bilaterally clear. Surgery was completed and patient was shifted to critical care unit (CCU) for intensive monitoring and ventilatory support. Patient was put on mechanical ventilation on SIMV mode. BP was maintained with noradrenalin support and HR was between 110-120/ min. Glasgow coma scale was E1VTM1 without sedation or muscle relaxant and patient showed no spontaneous respiratory effort for next 24 hrs in CCU. Pupillary reflex were absent. Patient doll’s eye test and caloric test were negative. A noncontrast CT scan of head was done which revealed large intraventricular haemorrhage [Table/Fig-1]. Neurological and neurosurgical consultation was taken and accordingly patient was managed conservatively. CT-head angiography was done which excluded any vascular malformation. After 36 hr stay in CCU, patient’s condition deteriorated. Patient went into cardiac arrest after 40 hrs. of admission and could not be revived.
CT scan showing intraventricular bleed
Discussion
Rhinoplasty is generally associated with increased bleeding due to rich vascular supply of nasal cavity and adrenaline is widely used to decrease bleeding during surgery. Previous studies showed that use of adrenaline is associated with many life threatening complications like myocardial infarction, pulmonary edema and ventricular tachycardia [1]. The dose of adrenaline should not exceed 3 mcg/kg for healthy patient [2]. In our patient, adrenaline was infiltrated intranasaly and intranasal adrenaline solution packing was done again. So, the amount of adrenaline exceeded the recommended dose. The mixing of adrenaline to blood in a highly vascularised and bleeding area leads to increased plasma adrenaline concentration. The patient showed marked hypertension and tachycardia followed by hypotension and cardiac arrest that was revived at that time [3]. CT scan head, which was done after shifting the patient in CCU, showed large intraventricular hemorrhage (IVH). Adrenaline activates β1, β2 and α receptors at different concentrations. β2 being most sensitive leads to hypotension by vasodilatation at lower concentrations while activation of α and β1 receptors leads to hypertension [4,5]. The most probable reason for mortality of our patient was IVH due to acute rise in blood pressure. CT head angiography excluded any vascular malformation. This incidence signifies that anesthetist must remain cautious while infiltration of adrenaline. Use of adrenaline with xylocaine should be used with caution, particularly when we are using epinephrine beyond 5 mcg/kg. Hemodynamic monitoring is must during any injection of vasopressor. By minimizing the concentration of adrenaline, effect of accidental intravascular injection or rapid systemic absorption can be attenuated [3,6].
Conclusion
Adrenaline infiltration can lead to serious complication as in our patient. The safe limit of adrenaline dose should always be respected. Careful hemodynamic monitoring is must to detect adverse effects and prompt treatment of hemodynamic swings should be done. Use of adrenaline on actively bleeding mucosal surface can lead to systemic absorption and it should be done with great care. Adrenaline is a life saving drug but it can become poison if not used carefully.
[1]. Wodorf NM, Pastore PN, Extreme epinephrine sensitivity with general anesthesiaArch Otolaryngol Head Neck Surg 1972 96:272-77. [Google Scholar]
[2]. David SJ, Hamstra J, Amin M, Cardiogenic shock following nasal septoplasty: a case report and review of the literatureCanadian Journal of Anesthesia 2008 55:376-79. [Google Scholar]
[3]. Hema HA, Kulkarni A, Ranjan RK, Ambreesha M, Ventricular tachycardia due to intranasal adrenaline in nasal surgery – a case reportInd J Anaesth 2008 52:199-20. [Google Scholar]
[4]. Yang JJ, Zheng J, Li HJ, Liu YX, She JC, Zhou ZG, Epinephrine Infiltration on Nasal Field Causes Significant Hemodynamic Changes: Hypotension Episode Monitored by Impedance-cardiography under General AnesthesiaJ Pharm Pharmaceut Sci 2006 9(2):190-97. [Google Scholar]
[5]. Bhandari S, Shaffi M, Bano S, Siddiqui SS, Ahmad J, A case of hypotension after intranasal adrenaline infiltration causing a clinical dilemma during the intraoperative periodIndian J Anaesth 2011 55(1):74-76. [Google Scholar]
[6]. Gupta N, Gupta V, Life-threatening complication following infiltration with adrenalineIndian J Anaesth 2014 58:225-27. [Google Scholar]