From the very beginning of the medical science the blood supply of human brain is of immense curiosity. Brain has high metabolic rate and intensely susceptible to ischemia. During intracranial or extracranial surgical procedures including carotid endarterectomy, angioplasty or stenting, the knowledge of cerebral blood flow is highly necessary to neurosurgeons or interventional radiologists for the surgery to be uneventful [1,2]. The base of the brain is closely related to a very sophisticated arterial network of vertebro-basilar and internal carotid arterial system, named circle of Willis. Posterior communicating artery (PCoA), a branch of internal carotid artery (ICA) acts as an anastomotic channel between the two systems. It joins with the posterior cerebral artery (PCA) and divides it into a pre (P1) and a post (P2) communicating segment. In classical circle, the blood flow through PCA is from basilar artery (BA) via P1 and P2 segment. But sometimes PCA carries blood from ICA instead of BA via PCoA even if the BA and its terminal branches are quite normal. In that case PCoA acts as a main artery rather than a collateral channel, and continues as P2 segment of PCA. Depending on the calibre, PCoA have different configurations like adult, fetal or transitional type and any of the three variants may develop in fetal period [3]. In adult life, commonly the adult configuration is present where P1 segment has a greater diameter than ipsilateral PCoA. But reverse is not rare where diameter of PCoA is greater than ipsilateral P1segment and the P2 segment is a continuation of PCoA, named as fetal type of posterior cerebral artery (FTP) [4]. In this type of configuration (fetal configuration) PCA is basically arises from ipsilateral ICA instead of BA. Such anatomical variation has clinical importance as thrombotic material from atherosclerotic lesion of ICA may be dislodged into PCA via greater diameter of PCoA [5]. Third type of configuration is transitional where diameter of both PCoA and P1 is equal and blood flow via P2 segment is from both arterial systems. Many studies have been reported regarding variations of circle of Willis, but best to our knowledge little literature is there addressing the configurations of circle of Willis comparing the both hemispheres, particularly in Indian population. This study has been done to compare the configuration of PCoA of each cerebral hemisphere with its other half on random basis in Indian population. Aim of the study is to know the degree of contribution of arterial system (vertebro-basilar or carotid) to the origin of PCA of each hemisphere. This knowledge will be helpful not only for future studies related with PCA but also for the neurophysicians and neurosurgeons while correlating the occurrence of stroke or TIA with the arterial pattern of P2 segment.
Materials and Methods
Fifty six brains, removed during routine dissection of 1st year M.B.B.S curriculum were used for this study from March 2010 to May 2013. All brains were obtained from donated cadavers of Indian population aged above 60 years. Any specimen with evidence of gross pathological lesions or trauma of the brain and its blood supplying vessels that might have affected the topography of the arteries was excluded from study. To exclude gender as one possible compounding factor, study was done only in male cadavers. After opening each calvaria by saw, dura was incised carefully. Special attention was taken in interpeduncular fossa to preserve the arterial circle which lies in subarachnoid cistern. After that the brain had been detached from spinomedullary junction and preserved in 10% formalin. The base of the brain was cleaned by peeling off arachnoid mater to expose the vessels. Each component vessel of the circle was dissected out. The origin, course, diameter and variations of P1 and P2 segment of PCA and PCoA were noted, recorded and evaluated in detail. Individual specimen was serially numbered, photographs were taken. Diameters of arterial segments (PCoA, P1, and P2) were measured by slide calliper to differentiate the adult, fetal and transitional type PCA. To compare the arterial (carotid or vertebro-basilar) predominance to the origin of P2 segment, all circles were classified into three types (I, II, III). The circles which contain classical or adult type configuration (unilateral / bilateral) were classified as type I. The circles which contain embryonic or fetal type PCA (unilateral or bilateral) were classified as type II and the circles which contain transitional type PCA (unilateral / bilateral) were classified as type III. As classical circle described by Willis contains bilateral adult configurations only, authors had considered the circle of unilateral fetal type configuration with adult or transitional configuration on other side as type II. While measuring the diameter some arteries were very narrow (diameter < 0.5mm) defined as hypoplastic following Kamath [6]. Statistical analyses for arterial diameters were expressed as mean and 95% confidence interval (Mean ± standard deviation). Correlations between the diameters of arterial segments (P1 and PCoA of right and left sides) of different configurations were tried to find out, demonstrated by means of the pearson’s correlation and placed in scatter gram. A p value of less than 0.05 was considered to indicate a statistically significant difference.
Results
After study of 56 brains, 3 types of configurations of PCoA were found. Thirty two specimens (57.2%) were notified as type I, 21 specimens (37.5%) were type II and 3 specimens (5.4%) were type III. While comparing the bilateral configurations, each type again had different varieties. Thirty circles (53.6%) had bilateral equal configuration of PCoA (bilateral adult, fetal, and transitional type were in 27, 2 and in 1 specimen respectively). Rest of the specimens had different configuration of PCoA on either half of the hemisphere. Some unilateral type I, II and III were associated with hypoplastic or aplastic PCoA on the other side. So, considering the maximum possible variations in different types, 21 subtypes (Ia-Ie, IIa-IIi, IIIa-IIIg) were made to see their incidences in present study. The details are shown in [Table/Fig-1]; possible subtypes IIIb, IIIc, IIId and IIIf were not found in present study. In one specimen of bilateral fetal type (IIa), right sided P1 segment was normal while on left side it was absent [Table/Fig-2]. [Table/Fig-3,4] represents type II d and III e respectively. The diameters of different arterial segments were varied in different types of configuration in different specimens. The range of the diameters of P1, P2 segment and PCoA were 0.3- 2.5mm, 0.5-3.8mm and 0.2- 3.8mm respectively in the present study. The mean diameters and 95% confidence interval (Mean ± standard deviation) of each segment of right and left sides are shown in [Table/Fig-5], some cases have negative lower limit of confidence interval which indicate margin of error and these have appeared because of small sample size (limited number of available dissected cadavers within the three year time period) and could be overcome with sufficiently large sample size. The greatest diameter of PCoA was 3.8mm and 3.6mm on right side and left side respectively, found in fetal type configuration. The least diameter of all specimens was 0.3mm on both sides. There were significant correlations present between the calibres of P1and PCoA of both sides in different types. In type I significant correlation present between right and left P1(r = 0.962, p = 0.0001) [Table/Fig-6] and right P1 and left PCoA (r = 0.429, p =0.014) [Table/Fig-7]. In type II negative correlation between right and left PCoA (r = - 0.509, p =0.019) [Table/Fig-8] and in type III perfectly positive correlation between left PCoA and P1(r =1.000, p =0.0001). No statistically significant age related differences were found. Apart from variations of circle of Willis no other associated anomalies like Adult Poly Cystic Kidney or other vascular malformations like Aneurysm of Posterior Communicating Artery, Berry Aneurysm in the Circle of Willis or Collagen Vascular diseases were found in the cadvers.
Types and Possible Subtypes of configurations with incidences of present study
| Type with Incidence | Configuration of PCoA | Subtype | Number of Specimens(n) | Incidence (%) |
|---|
| Right Side | Left Side |
|---|
| Type I (57.2%) | Adult | Adult | Ia. | 27 | 48.2 |
| Adult | Hypoplastic | Ib. | 2 | 3.6 |
| Adult | Absent | Ic. | 1 | 1.8 |
| Hypoplastic | Adult | Id.. | 1 | 1.8 |
| Absent | Adult | Ie | 1 | 1.8 |
| Type II (37.5%) | Fetal | Fetal | IIa. | 2 | 3.6 |
| Fetal | Adult | IIb. | 7 | 12.5 |
| Fetal | Transient | IIc. | 1 | 1.8 |
| Fetal | Hypoplastic | IId. | 3 | 5.3 |
| Fetal | Absent | IIe. | 1 | 1.8 |
| Adult | Fetal | IIf. | 1 | 1.8 |
| Transient | Fetal | IIg. | 1 | 1.8 |
| Hypoplastic | Fetal | IIh. | 3 | 5.3 |
| Absent | Fetal | IIi. | 2 | 3.6 |
| Type III (5.4%) | Transient | Transient | IIIa. | 1 | 1.8 |
| Transient | Adult | IIIb. | 0 | -- |
| Transient | Hypoplastic | IIIc. | 0 | -- |
| Transient | Absent | IIId | 0 | -- |
| Adult | Transient | IIIe | 1 | 1.8 |
| Hypoplastic | Transient | IIIf | 0 | -- |
| Absent | Transient | IIIg | 1 | 1.8 |
Type IIa configuration with left P1 aplasia,
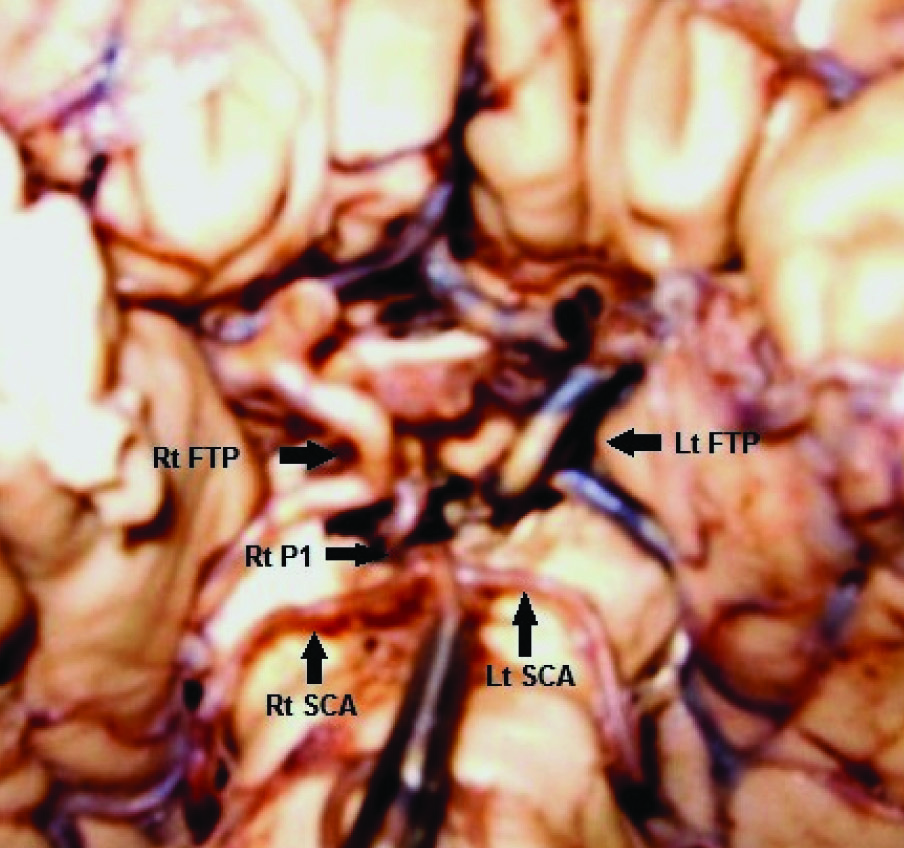
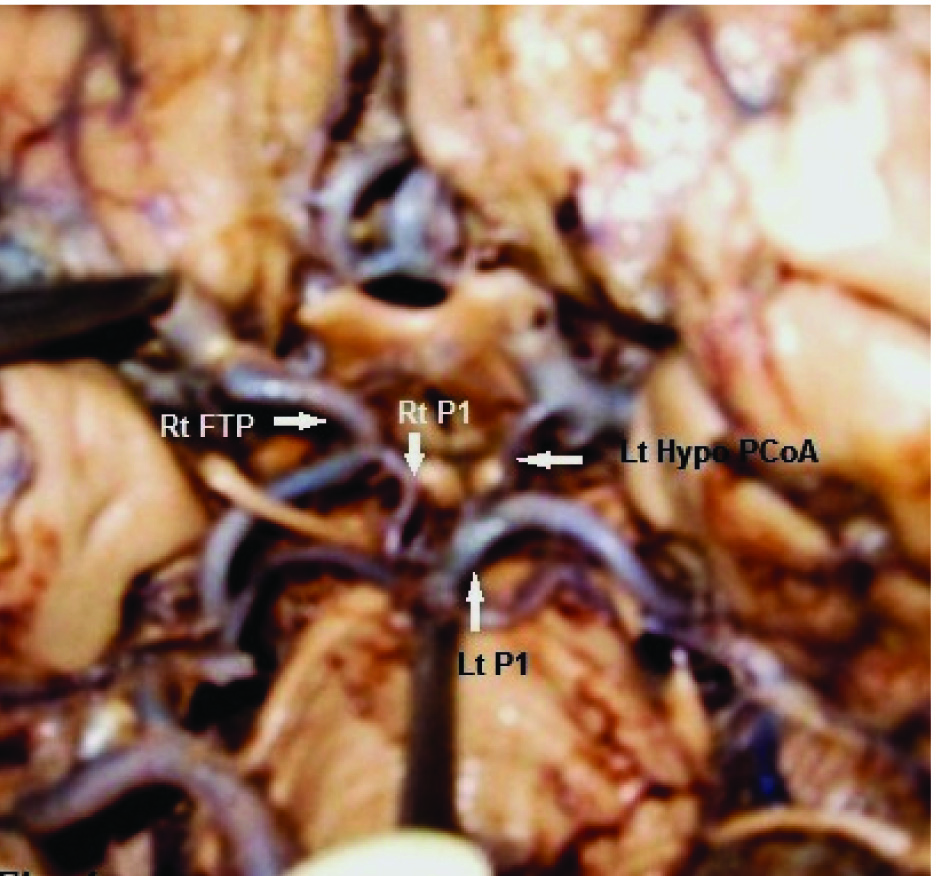
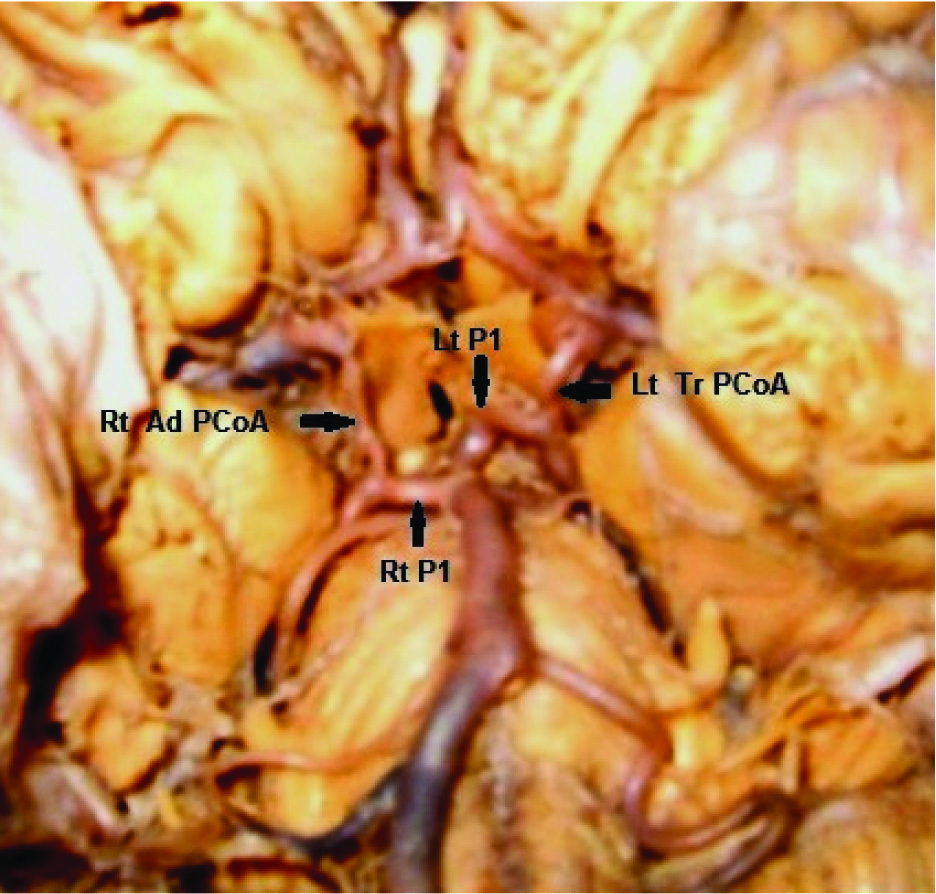
Type III e configuration. Lt FTP - Left Fetal type Posterior cerebral artery, Rt FTP - Right Fetal type Posterior cerebral artery, Rt P1 – Right pre communicating part of Posterior cerebral artery, Lt P1 – Left pre communicating part of Posterior cerebral artery, Lt Hypo PCoA – Left hypoplastic Posterior communicating artery, Rt SCA- Right Superior Cerebellar artery, Lt SCA- Left Superior Cerebellar artery, Rt Ad PCoA – Right Adult type Posterior communicating artery, Lt Tr PCoA – Left Transitional type Posterior communicating artery
Mean diameter (mm) and 95% confidence interval (in bracket) of arteries in three different types
| Types | PCA Mean diameter (mm) (95% CI) | PCoA Mean diameter (mm) (95% CI) |
|---|
| Right side | Left side | Right side Left Side |
|---|
| P1 | P2 | P1 | P2 |
|---|
| Type I | 1.99 (1.39, 2.59) | 2.11 (1.39, 2.83) | 2.01 (1.37, 2.65) | 2.10 (1.36, 2.84) | 1.23 (0.47, 1.99) | 1.22 (0.38, 2.06) |
| Type II | 1.24(-0.16, 2.64) | 2.85 (1.73, 3.97) | 1.72 (0.54, 2.90) | 2.63 (1.59, 3.67) | 2.23 (-0.43, 4.89) | 1.79 (-0.45, 4.03) |
| Type III | 1.6 (1.26, 1.94) | 1.9 (1.18, 2.62) | 1.63 (1.33, 1.93) | 1.83 (1.25, 2.41) | 0.93 (-0.87, 2.73) | 1.63 (1.33, 1.93) |
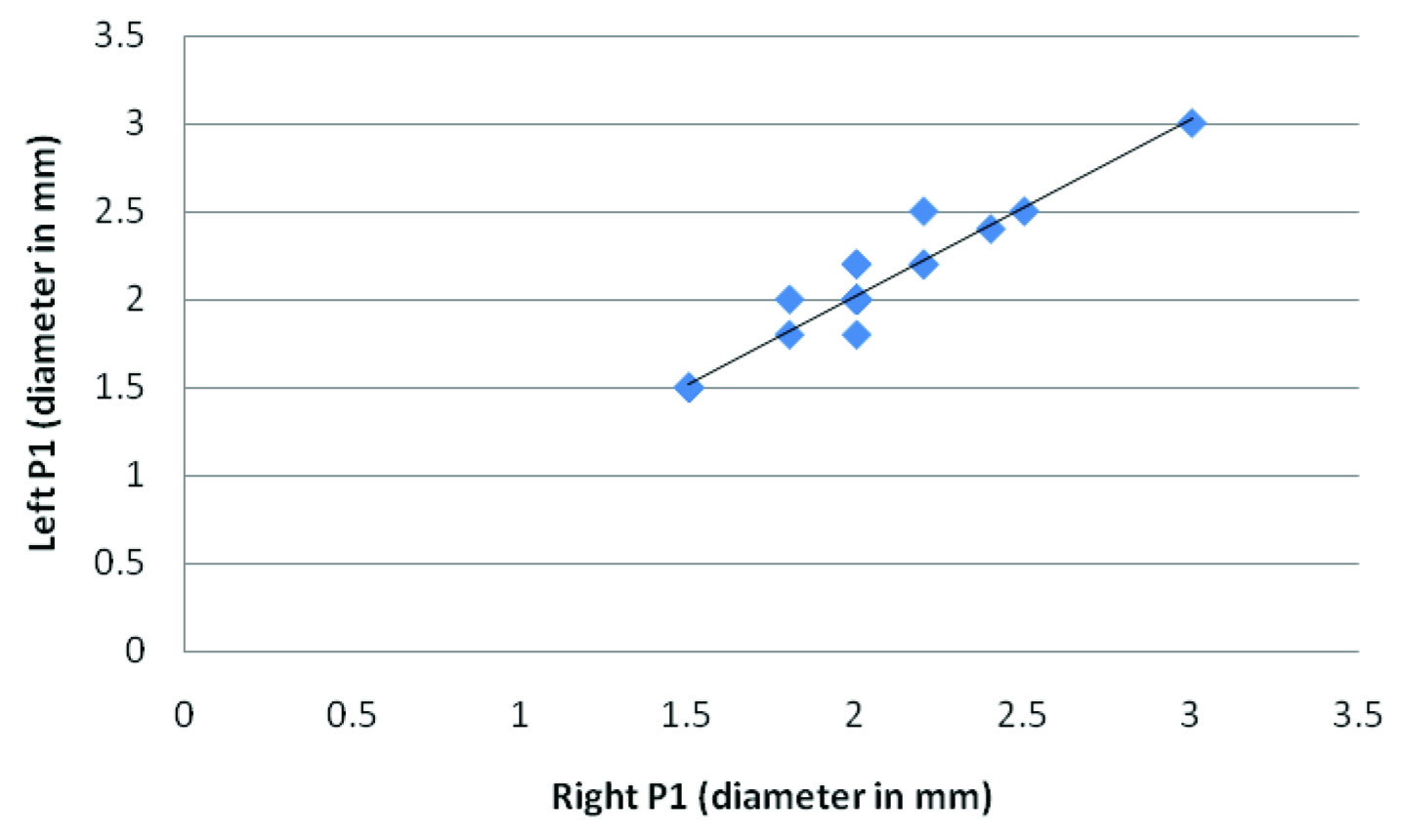
Scatter gram showing significant correlation between the diameters of Right P1 and Left P1 in type I
Scatter gram showing significant correlation between the diameters of Right P1 and Left P1 in type I (r = 0.962, p = 0.0001)
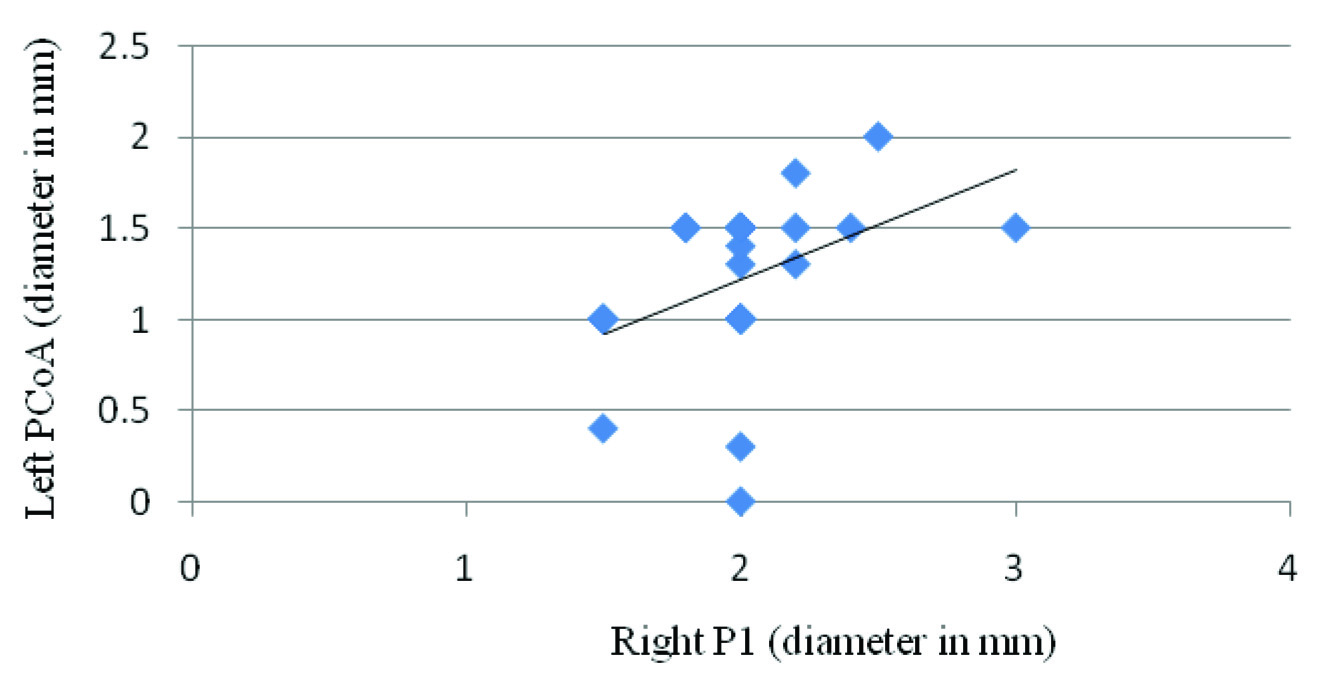
Scatter gram showing significant correlation between the diameters of Right P1 and Left PCoA in type I (r=0.429, p=0.014)
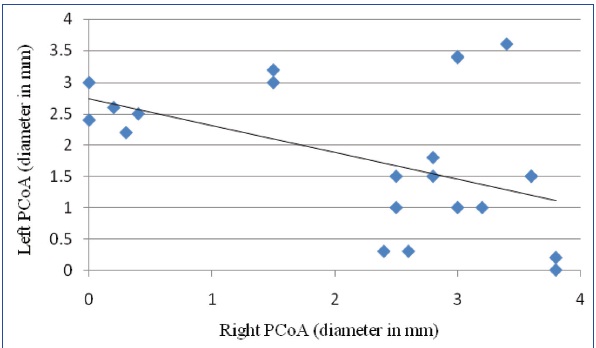
Scatter gram showing negative correlation between the diameters of Right PCoA and Left PCoA in type II (r = -0.509 p = 0.019)
Discussion
According to Willis description (bilateral adult configuration) blood supply via PCA is purely from basilar artery if there is no obstruction occurs. But in present study it carries blood from vertebro-basilar system in 57.2% of the cases (type I), from carotid system in 3.6% of the cases (type II a) and from both systems in 1.8% of the cases (type III a) bilaterally. This result indicates that the blood flow via PCA is not limited only by vertebrobasilar system. The arterial pattern of both hemispheres is same in 62.6% of the cases in present study. In rest 37.4% of cases it is different on right and left hemisphere. In the current study it is noticed that in 7.2% of the cases, the both arterial system is involved for one hemisphere blood supply in combination with either system (carotid – type II c, II g / vertebro-basilar system – III e, III g) on opposite side. More interestingly a high percentage (30.3%) of the cases have been found where carotid system contributes in one hemisphere and vertebro-basilar system in other hemisphere (type II a, II b, II d, II e, II f, II h, II i). Such unilateral FTP will produce a substantial left and right asymmetry in perfusion maps of cerebral hemisphere (done by perfusion images) which mimics cerebrovascular disease as the blood supply via PCA of two hemispheres are by two different arterial system [7]. So, knowledge of such variation in high percentage is important for clinicians as well as for radiologist to avoid the misinterpretation and to understand the fact that asymmetry in perfusion images might not result from pathology but from anatomical variation [7].
From previous study reports [5,6,8–10,] authors can get an idea about the incidences of different types of configurations only, but comparison of one hemisphere’s configuration with its other half has not been studied yet. Vasovic L et al.,[11] reported the incidences of bilateral adult type configuration, bilateral fetal type configuration, adult-fetal configuration and adult-transitional configuration are 68.18%, 7.27%, 13.63% and 10.91% respectively, but in their study they have omitted about the fetal-transitional configuration which is present in 3.6% cases in the present study. Unilateral hypoplasia or aplasia of PCoA with adult, fetal or transitional configuration of other side are also not present in previous study [11] which is very important as the P2 segment of both hemisphere carries blood from the two different arterial system. In that sense present study is unique and could not be compared with others. According to previous literature [4,5,10,12,13] incidences of unilateral fetal type ranges from 6%–25% but in present study it is 33.9% [Table/Fig-9]. Presence of such embryonic or fetal type communicating artery protects the brain tissue in case of ischemia of vertebrobasilar system and there will be damage of primary visual area of one side without any damage to the other side in occlusion of basilar artery where such unilateral fetal type PCoA is present [14]. On the other hand, that chances of ischemic attacks are more in compare to normal in FTP, especially when P1 segment is absent as a large area of brain is provided with blood by only ICA [15]. So, in early diagnosis of cerebral insufficiency in intrauterine stage, hypothetically it could be thought of as arterio-grafting to establish the collateral circulation where it is deficient.
Comparison of unilateral and bilateral fetal type configuration
| Name of Authors | Number of Specimens (n) | Unilateral fetal type | Bilateral fetal type |
|---|
| Saeki & Rhoton [5] (1977) | 50 | 20% | 2% |
| Krabbe Hartkamp et al., [4] (1998) | 150 | 25% | 7% |
| Sahni et al., [12] (2007) | 280 | 6.8% | 0.3% |
| Krishnamurthy et al., [13] (2008) | 89 | -- | 2.2% |
| De Silva et al., [10] (2010) | 225 | 6.1% | 1.3% |
| Present Study (2013) | 56 | 33.9% | 3.6% |
As the third cranial nerve is closely related with PCoA, so aneurysm of the artery is the most common cause of third nerve palsy. In present study no aneurysm is present but greater diameter of PCoA has been found. Dilatation of PCoA can compress the oculomotor nerve and paresis may occur [16]. Greatest diameter of right and left PCoA in present study is 3.8mm and 3.6mm respectively which is closely matched with the report of Pai (right PCoA=4mm)[9] and Kamath (left PCoA=3.5mm)[6]. The mean diameter and 95% confidence interval (CI) of P1and PCoA of right and left sides are very much corroborative with Krabbe-Hartkamp [4] but grossly differs in P2 and FTP. According to present result mean diameter of P2 and FTP are 2.33mm and 2.01 mm respectively whereas previous author [4] has found 1.9mm and 1.7mm respectively. On the other hand, Confidence Interval of P2 and FTP shows 1.25mm, 3.41mm and -0.45mm, 4.47mm in present study which is not matched with previous one [4] where Confidence Interval for P2 is 1.8mm, 1.9mm and for FTP is 1.7mm,1.8mm. Collateral potential is believed to be dependent on presence and size of the vessel, which vary among normal individuals. The hemodynamic balance is usually disturbed by variation in the calibre of the communicating arteries which could be fatal in case of stroke [17]. After occlusion of a cerebral artery brain tissue can recover fully if blood flow is quickly restored via collateral channel and symptoms will be transient (transient ischaemic attack or TIA). After comparing the of present study with previous [4], it can be suggested that due to presence of greater diameter of FTP and high percentage of fetal configuration, Indian population are protected from the attack of TIA and infarction.
Embryological Explanation
Initial PCA represent a branch of primitive ICA. Afterwards the definitive PCA appear by division of basilar artery when vertebrobasilar system develops and blood flow through the P1 segment starts [18]. In that stage, all arterial segments of the circle have equal diameter [3]. The ratio in the flow of blood between carotid and vertebrobasilar system is continuously altered until the growth of the brain has been settled. Occipital lobe gets separate blood supply from vertebrobasilar system when its functional demand increases [8]. Around 22nd 24th weeks, the PCoA and / or the P1 may enlarge and either artery get chance to increase its size according to most favourable hemodynamic situation, thus adult or fetal configuration may develop [19]. In 29-40 wk of gestation the prominent configurations becomes adult and fetal types, 53-59% and 33-34% respectively [8,10]. Other opinion suggests that variation of the segmental calibres are due to amplitude of neck movements in later years of life or due to genetic factors [20,21].
Conclusion
The knowledge about the predominant arterial system for origin of PCA of both cerebral hemispheres is a must before planning for the treatment of different neurological cases. An attempt has been made to assess the possible subtypes of bilateral configuration of posterior bifurcation of posterior communicating artery which could be helpful for treatment modalities. The study would be a complete one if we could see the changes of arterial system by serial radiologic study from its fetal to adult stage in a human brain and its blood flow kinetics.