Introduction
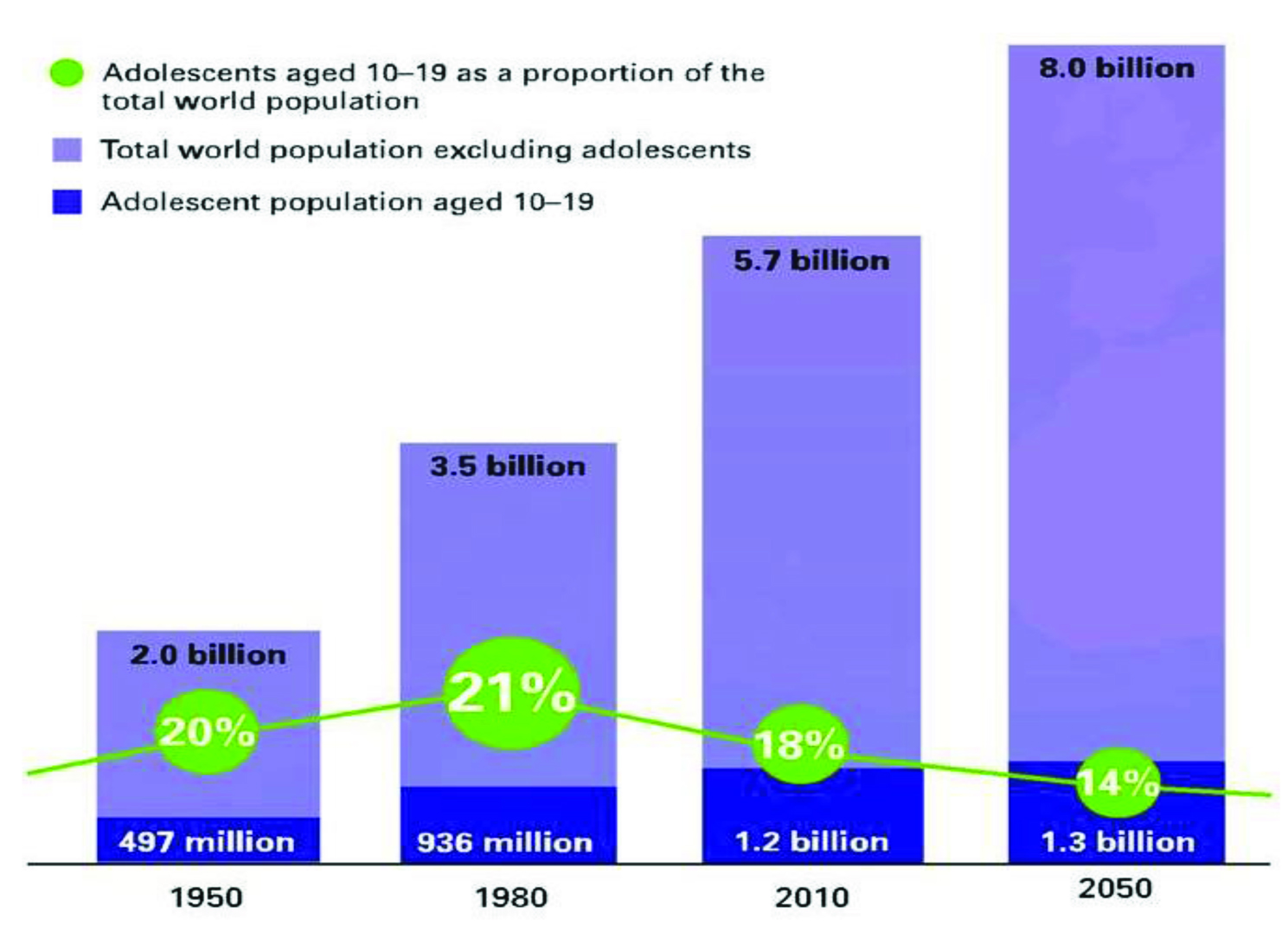
Adolescents are the young people aged between 10 to 19 y. It is a transitional stage of physical, physiological and psychological development from puberty to legal adulthood. Worldwide more than 1.2 billion are adolescents: this indicates that roughly one in every six persons is an adolescent [Table/Fig-1] [1]. About 21% of Indian population is adolescents (about 243 million) [2]. They are the future of the nation, forming a major demographic and economic force. They have specific needs which vary with gender, life circumstances and socio economic conditions. They face challenges like poverty, lack of access to health care services, unsafe environments etc. It is a period of preparation for undertaking greater responsibilities like familial, social, cultural and economic issues in adulthood.
Adolescent Health Problems
Adolescents are a group of apparently healthy individuals. The health status of an adolescent determines the health status in his/her adulthood. Many serious diseases in adulthood have their roots in adolescence. Also, many adolescents do die prematurely due to various reasons that are either preventable or treatable and many more suffer from chronic ill-health and disability. We can categorize the health needs of the adolescents broadly into three categories- physical, psychological and social. The main health issues faced by the adolescents include: Mental health problems, early pregnancy and childbirth, human immunodeficiency virus/sexually transmitted infection (HIV/STI) and other infectious diseases, violence, unintentional injuries, malnutrition and substance abuse.
Adolescents form a socially important segment of the population. Apart from physical health, a positive social health constitutes holistic health of the adolescents. Prevalence of sexual abuse, violence and physical abuse are increasing among the adolescents. For a long time, there was no organized system to govern and monitor the social needs of adolescents. The Committee on the Gopalakrishnan4Rights of the Child (CRC, WHO), published guidelines in 2013 on the rights of children and adolescents and issued guidelines on States’ obligations to recognize the special health and development needs and rights of adolescents and young people. This has been further envisaged in WHO report in 2014 titled “Health for the world’s adolescents” [3].
In India, data on adolescents from national surveys including National Family Health Survey III (NFHS-3), District Level Household and Facility Survey III and Sample Registration System call for focused attention with respect to health and social development for this age group. It has therefore been realized that, investing in adolescent health will yield demographic and economic dividends for India. In view of this, Government of India launched its first comprehensive programme for adolescents, ‘Rashtriya Kishor Swasthya Karyakram’, during January 2014 which has a sharp focus on adolescents’ sexual health. The programme envisages that all adolescents in India are able to realize their full potential by making informed and responsible decisions related to their health and well-being [4].
In this review article, we aim to discuss the magnitude of adolescent health problems, existing adolescent health programmes, their services and the challenges in achieving universal coverage of wholesome adolescent health in India at present. Our review was based on published national and international literature yielded on systematic search using different sources. This is intended to create awareness among the stakeholders about the importance of strengthening the adolescent health services and to meet their felt needs.
Global Scenario
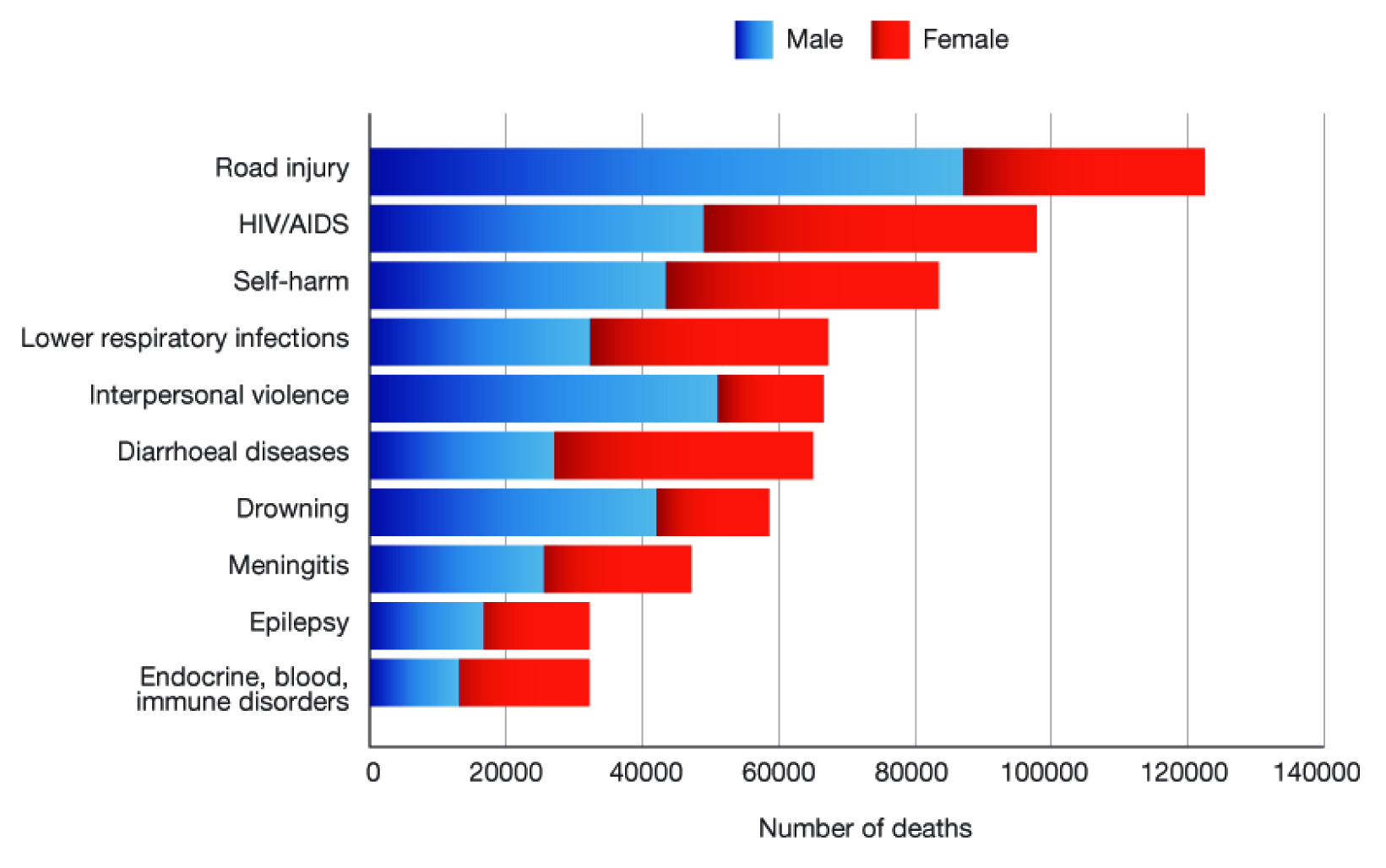
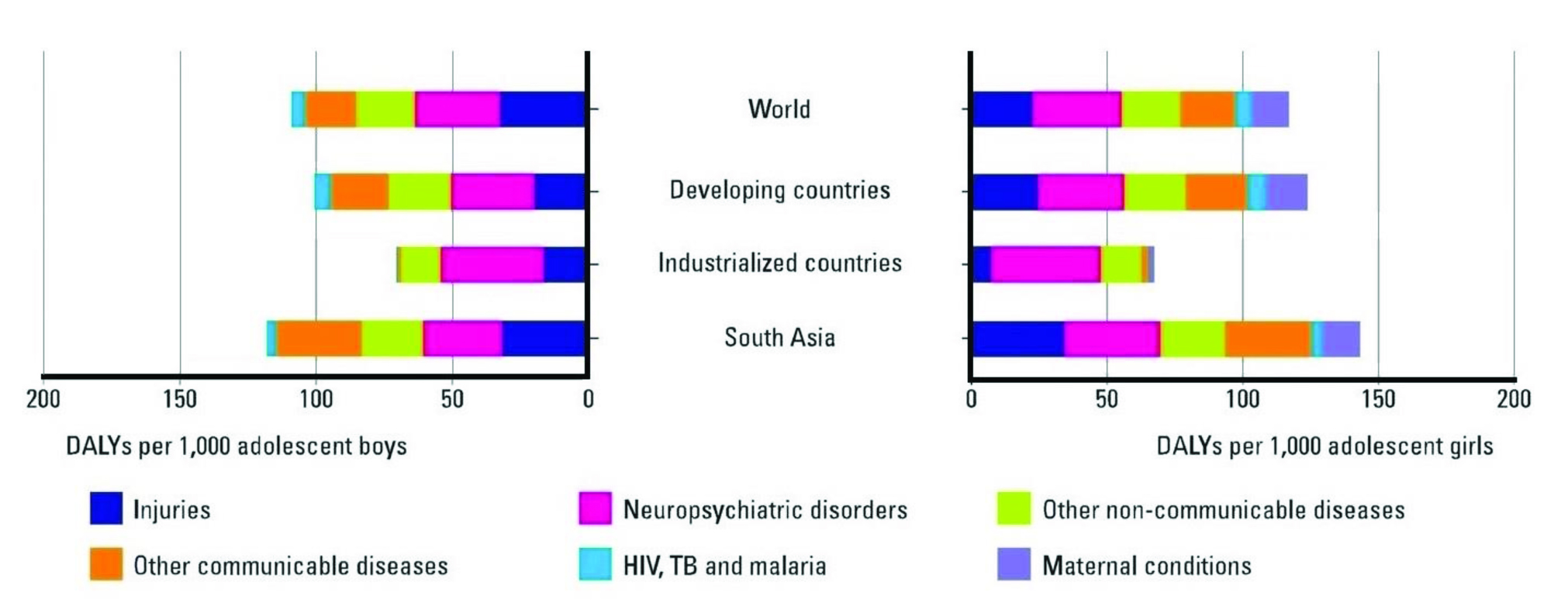
About 1.3 million adolescents died from preventable or treatable causes during 2012 as per WHO reports [5]. Road traffic injuries were the leading cause of death among adolescents [Table/Fig-2] [6]. About 15% of global maternal death occurs among adolescents girls [7]. The major causes for Disability Adjusted Life Years (DALY) in adolescents were given in [Table/Fig-3] [8]. Injuries and neuro-psychiatric disorders were the major issues in adolescents. There is an increasing trend in adolescent obesity due to great shift in diet and activity pattern [9]. Nearly 35% of the global burden of disease has roots in adolescence. Half of all mental health disorders in adulthood starts by 14 y of age, most cases are undetected and untreated [3].
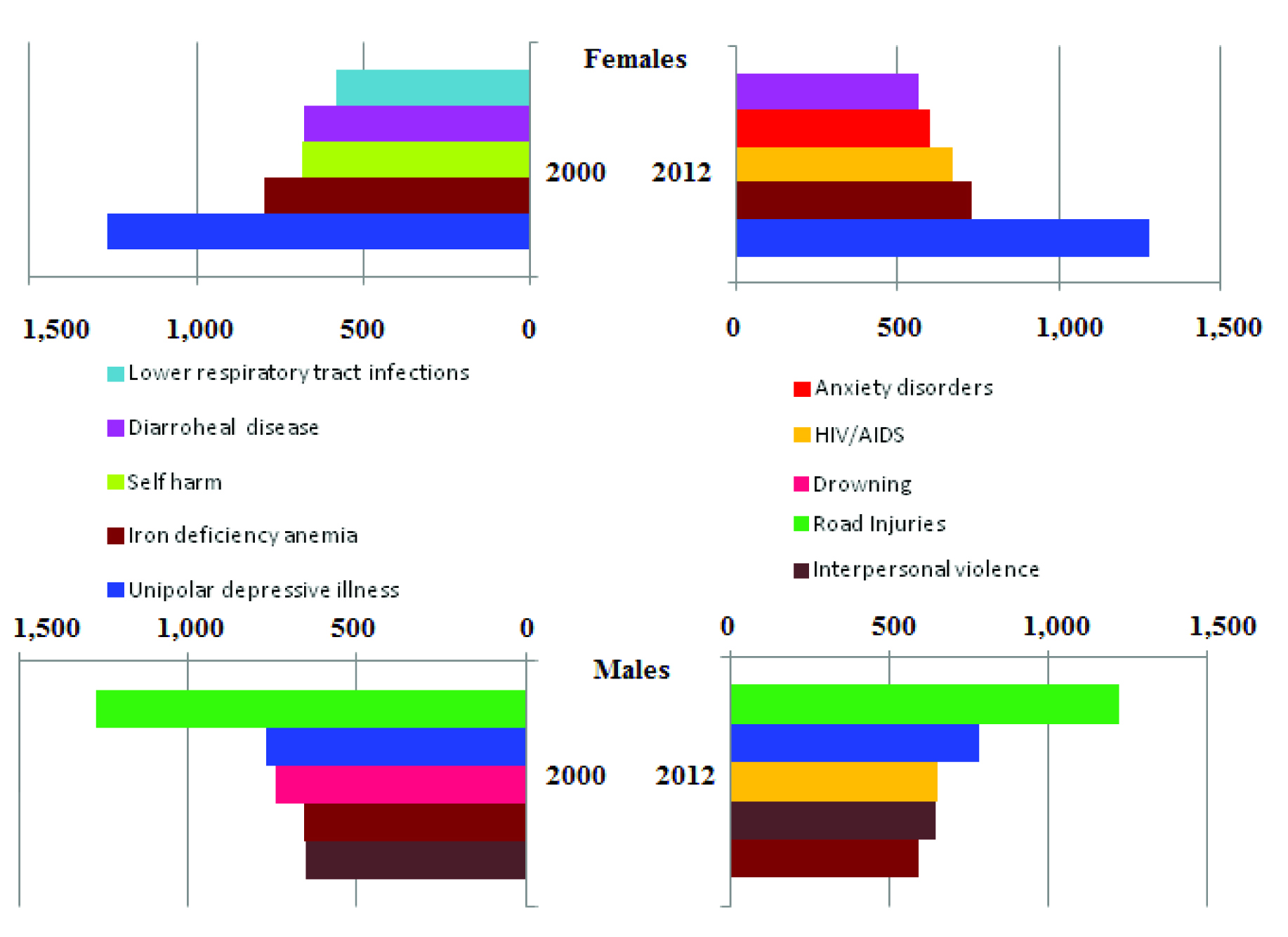
In the South East Asian Region (SEAR), unipolar depressive illnesses in females, and road traffic injuries in males were the major health issues and it remains at the top throughout the years. AIDS has emerged as a third leading cause of DALYs in adolescents in the last decade [Table/Fig-4] [10]. These issues need to be addressed for the wellbeing of adolescents.
Problem Status in India
India has the largest adolescent population in the world. The decadal comparison of State wise distribution of adolescent population is shown in [Table/Fig-5][11].The distribution of percentage of adolescents among the top and bottom five States are shown in [Table/Fig-6][11]. There were few studies done on the prevalence of diseases and their risk factors and disease pattern among adolescents in these States. Some of the major health problems of adolescent population are briefly discussed below.
Reproductive and Sexual Health
Adolescents have diverse sexual and reproductive health problems. Some of the important determinants of adolescent reproductive and sexual health are given in [Table/Fig-7]. As per NFHS–3 data, 2.7% boys and 8 % girls reported sexual debut before the age Statesof 15 and most of the sexual activity happens in the context of marriage, this leads to early pregnancy due to social pressure. Even though contraceptive awareness is 94% among girls aged 15–19, only 23% of the married and 18% of the sexually active unmarried girls in this group, used a contraceptive once at least [13]. All the three NFHS shows almost equal prevalence (59.1%, 59.8% and 58.2%) of pregnant and mothered adolescent and there is a steady increase in percentage of first pregnancy among adolescents (11.7%, 12.4% and 14.4 %). Early marriage and low contraceptive usage are the reasons behind this trend.
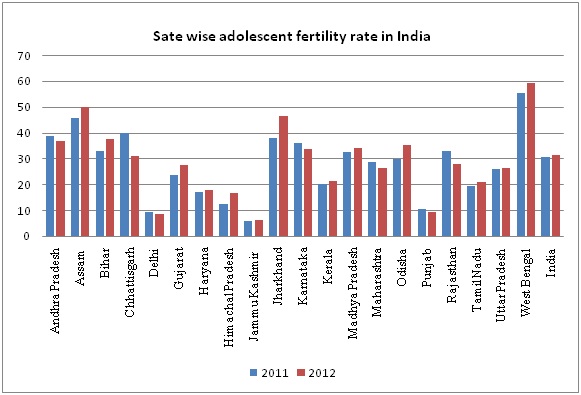
The State wise adolescent fertility rates during the period of 2011 and 2012 are shown in the [Table/Fig-8] [14,15]. Adolescent fertility rates contribute 17% to the total fertility rate in India and about 14% of births in women aged below 20 were unplanned [2]. Early and unplanned adolescent pregnancies are highly prone for adverse pregnancy outcomes like eclampsia, low birth weight, early neonatal death and congenital malformation [16]. In addition, 34% of ever-married adolescent girls (15–19 y) reported that they suffered physical, emotional or sexual violence inflicted by their partner [2]. There is a remarkable decline in these rates as age of marriage raises. So, early marriage also carries the risk of subjecting girls to all forms of violence.
In India 19% girls and 35% boys had comprehensive knowledge about HIV/AIDS. Only 15% young men and women (15-24 y) reported that they received family life or sex education [2]. Eventually due to inadequate knowledge they are at greater risk of exposure to unprotected sex, unethical sexual practice and STIs. In the age group of 15–19 y, among those who had sexual intercourse, 10.5% of girls and 10.8% of boys reported having STI or symptoms of STI and 0.07% of girls and 0.01% of boys were found to be HIV positive [13]. The awareness regarding transmission of STIs is low among adolescents. This, in addition to social stigma the diseases were often undisclosed, left untreated leading to complications like infertility, pelvic inflammatory disease and cancer.
Nutritional Health
Adolescents have increased nutritional requirements demanding diet rich in protein, vitamins, calcium, iodine, phosphorus and iron due to rapid growth spurt and increased physical activity. NFHS-3 data shows, in the age group 15–19 y, 47% girls and 58% boys were thin, 56% girls and 30% boys were anemic, 2.4% girls and 31.7% boys were overweight and 2/1000 adolescent girls and 1/1000 adolescent boys suffer from diabetes. They are also highly prone for eating disorders like anorexia nervosa or binge eating due to body dissatisfaction and depression.
Use of mass media is higher among adolescents (male 88.2% and female 71.5%) [12]. It plays an important role in habit picking and decides their lifestyle pattern. Its influence is clearly shown in a study from Chennai done in the age group 11 to 17 y reporting that, 90% eat either food or snacks while watching TV, 82% buy food products and snacks based on advertisement, 59% skipped outdoor activities for TV, 42% follows diet and 42% exercise to get the body like their favorite media personality [17]. Television viewing in childhood and adolescence is associated with overweight, poor fitness, smoking and raised cholesterol in adulthood [18].
Mental Health
Mental health problems are one of the most neglected issues among adolescent. Mortality and morbidity due to mental disorders in adolescents increased and topped in recent years. A study from Goa, among 16 to 24 y old, shows 3.9% of youths reported suicidal behaviours with females four times more prone than males. This suicidal behaviour is independently associated with factors like absenteeism, independent decision making, premarital sex, sexual abuse, physical abuse from parents and mental disorders [19]. In India suicide among adolescents is higher than any other age groups that is 40% of suicide deaths in men and 56% of suicide deaths in women occurred in 15–29 y of age [20].
The prevalence rate of child and adolescent psychiatric disorders in the community has been found to be 6.46% and in schools, it was 23.33% and the reporting systems of psychiatric disorders in children are found to be inadequate [21,22]. From the above studies it is evident that a considerable proportion of adolescent have mental health problems.
Accidental and Intentional Violence
In India, in 2001-03, deaths due to unintentional injuries constituted nearly 20% of the total deaths in 5–29 age groups [23]. About 77.5% of adolescents are at risky behaviours, ignores traffic rules leading to road-traffic accidents and deaths, as reported in a study from Delhi [24]. Sexual abuse is one of major problems faced by adolescent girls and boys equally. These problems mostly go unnoticed as the victim suffers in silence because of fear and social stigma. This indirectly affects the physical health, mental health and the academic performance [25].
Substance Abuse
Substance abuse is yet another serious issue as adolescents are ignorant about its consequences. NFHS–3 data shows, in the age group 15–19, about 11% of adolescent boys and 1% of adolescent girls had consumed alcohol, in that 3% consume it daily. About 29% boys and 4% girls use some kind of tobacco. The average age at tobacco use initiation was earliest at 12.3 y and alcohol usage at 13.6 y among adolescents [26]. About 11% of cannabis users were introduced to it before the age of 15 [2]. Initiating cannabis at this age is strongly associated with the development of Schizophrenia spectrum disorders in adulthood [27].
Status in Tamil Nadu
As per 2011 Census, there were about 1.24 crore adolescents in Tamil Nadu and more than half of them living in the rural areas. Literacy level among adolescent (97.70%) in Tamil Nadu is higher than the State’s literacy rate (80.09%). Even though the literacy rate is high, majority (63.16%) of the adolescents in rural areas were employed, particularly 27.16% in the agricultural sector. In the urban areas, only 36.83% of the adolescents were employed. The fertility rate in rural areas (20.1) was high when compared to urban areas (18.5). Tamil Nadu’s parameters as far as adolescents were concerned, were in line with the national scenario where more youths live in rural areas than in urban areas and the literacy rate is also higher in the group when compared to overall literacy level [28].
Adolescent Health Programmes and Its Ministries
Adolescent health programmes are implemented by various ministries under the government of India. They provide different types of services targeting adolescent health problems in different areas. Adolescent health programmes, their ministries and the services provided are described in [Table/Fig-9] [29-41].
Challenges Concerning Adolescent Health
Though adolescence is usually a healthy period, several risk factors of adult diseases which begin in adolescence can be prevented with proper interventions during this period, though with challenges. Exclusive data pertaining to the adolescent health issues in Indian scenario is not available and hence we used the data pertaining to South East Asia Region for comparison in which India is a major constituent country. The data about important adolescent’s health issues in different areas are limited. Hence detailed investigation and reports on adolescent’s health issues is the need of the hour.
Reproductive and Sexual Health
From the studies done in the past, it is evident that adolescent have no proper knowledge regarding STIs and an educational intervention shows significant improvement in the knowledge level of the participant. At this age, curiosity about sexuality increases, they start showing sexual interest in opposite sex. Media also plays a major role in exposing them to sexually explicit materials which make them perpetrators of sexual violence.
Mental Health
In the past decade mental health problems have emerged as an important cause of adolescent morbidity. Alcohol use disorder and psychiatric problems are the important cause of Years Lost due to Disability [5]. Focus towards these problems in adolescent health programmes happens to be less when compared to Reproductive and Sexual Health. So it is essential to give equal importance to other key areas like mental health services and Behavioural Change Communication towards healthy lifestyle.
Nutritional Problems
Nutritional requirement are higher among adolescents than any other period of life. Inadequate diet intake at this age leads to stunted growth and delayed sexual maturation [42]. Lot of junk food products are promoted by celebrities with catchy advertisements leading to adaptation of unhealthy food habits. Media influences the diet and lifestyle among adolescents and leads to nutritional disorders by making them sedentary and giving false hopes. Habits like dieting and exercising inspired by a media celebrity cannot be taken as a positive impact, often they do it in an incorrect way and consume low quality protein supplements without proper guidance which may lead to complications like renal failure. Instead of taking balanced diet they starve and end up in anorexia nervosa. These issues can be reduced by routine screening and nutritional education.
Substance Abuse
Habits like smoking and alcoholism have lifelong impact and potential to cause health problems like coronary heart disease and diabetes in adulthood. Even though there is legal restriction, alcohol and tobacco products are available generously for under-18 age group. Primordial prevention from substance abuse with strict enforcement of law can prevent occurrence of such diseases. A study done in Chennai reported that parental substance abuse and lack of parental supervision leads to adolescent substance abuse [43]. Parents must know their responsibility and take every effort to monitor their children activities and should set a good example to their children.
Road Traffic Accidents
Road traffic injuries emerged as a leading cause of death among adolescents. Rash driving, driving without license, drunken driving and use of mobile phones while driving are factors associated with road traffic injuries in young drivers. This can be prevented by strict enforcement of law and by conducting awareness campaign targeting adolescents insisting the need for following safety rules.
Challenges in Parenting
Parents have greater responsibility in guiding their children but due to cultural barriers they neglect to talk about physical and physiological changes, in consequence of this, growing children learn about sexuality and secondary sex characteristics from their peer groups or other inappropriate sources leads to abnormal social behaviour. Most of the children’s psychiatric disorders were unidentified because of parent’s ignorance and negligence.
Challenges in Existing Adolescent Health Services
With so many programmes available, the services have not reached the target group adequately because resources like materials, money and man power are limited. There is no direct access, space for privacy and ideal timing (restrictions in days and time) for the target population. Service providers are not given proper training. For the health care providers it is usually an extra burden because no man power has been allotted separately for adolescent health services. Adolescents have little knowledge about the need of health services. They are scared of revealing personal issues to another person and getting examined by opposite sex health worker. So they themselves act as major obstacle for the services to reach them.
Though Adolescent Friendly Health Services (AFHS) based adolescent clinics are said to address all the health needs of adolescents, the delivery of services mainly targets reproductive and sexual health and all other issues are not adequately focused. Even with this great focus on ARSH, NFHS data shows no significant decrease in adolescent pregnancy. In fact there is an increasing trend in first pregnancy in adolescent and the birthrate in the age group 15 to 19 y is still 31.5 per thousand adolescent girls, which is high for the efforts and inputs given by the health system [15].
Adolescent health services are not comprehensive, so many schemes exist but these schemes were placed under different ministries and some of the schemes provide the same services as others which may result in unnecessary duplication. In 2014 Ministry of Health & Family Welfare (MoHFW), launched a comprehensive programme (Rashtriya Kishor Swasthya Karyakram), but similar services provided by MoHFW and other ministries are not going to be terminated. To avoid such confusions and to be cost effective, all the services for adolescents should come under a single programme. It is also essential to develop a screening tool specific for Indian adolescents. This has been already implemented in United States by National Adolescent and Young Adult Health Information Centre, University of California [44]. Innovating such tools based on our requirements can be very useful in diagnosing diseases and to search for and eliminate any risk factors as early as possible.
Having critically analyzed the problems and the services for the adolescents two questions arise in our minds: Are we going in the right direction? Is it enough to deal with the target population alone? To address this current scenario, we should consider redefining our approach; the target population should include elders like parents and teachers also in defining, planning, implementing and evaluating specific programmes for adolescents.
Recommendations
While planning it is important to identify the felt needs of the adolescents and the services should be demand driven. It is equally important to create awareness among the adolescents about the significance and the need of the services and to motivate them to avail the services. The following recommendations shall be considered for improving adolescent health services.
1. Introduce age appropriate sex education with abuse prevention skills at schools, colleges and also in the community to bridge the knowledge gap in adolescent. With this approach, sexual abuse, early sex debut and unsafe sexual practice can be reduced and the contraceptives usage can be increased. This in turn prevents unwanted pregnancy, AIDS/STIs and its complications.
2. Take step to delay age of marriage through advocacy, counseling and strict enforcement of law. Adults should be educated to prevent early marriage, teenage pregnancy and its complications.
3. Educate Adolescents and parents regarding the nutritional requirements and to adapt diet appropriate for age.
4. Psychological disorders and social misbehaviour can be greatly reduced by giving top priority and effective implementation of mental health services at all levels. Educate parents and teachers to improve the quality of relationship with children to ensure a safe, secure and appropriate environment.
5. All PHC’s has to be equipped to deliver AFHS beyond existing days and time restriction. A separate sophisticated wing to treat adolescent at secondary and tertiary care level can be established.
6. Medical officers and the health workers at all level should be given exclusive training in handling adolescents. Health workers of same gender should address the problem of boys and girls separately.
7. Facilitate better relationship of trust and confidence in adolescent to get accurate and detailed information related to their health problems.
8. Counseling should be strengthened by well trained healthcare providers and involve parents and elders of the family in home-based counseling.
9. Encourage community participation in mobilizing adolescents to build life skills and to take active part in community programs.
10. Strict enforcement of laws related to traffic rules, prohibiting sale of tobacco, alcohol and other substance of abuse to minors. Restricting advertisement related to junk food products is essential.
11. Online consultation and counseling can be considered. It will be accessible and gives a feel of security and confidentiality for adolescent population.
12. Universal coverage of Adolescent friendly clinics is highly recommended. Through that, routine screening of adolescent for health problems, and their risk factors by creating a standardized protocol can be initiated and the services required can be provided.
13. To avoid unnecessary wastage of resources, AFHS should come under one roof. It should be accessible, assure confidentiality, appropriate and specific for the locality, with well trained health workers with a diplomatic approach and at convenient timings.
Proportion of adolescents and World population
Source: progress for children; A report card on adolescents. UNICEF [1]
Top 10 causes of death among adolescents by sex
Source: Health for World’s adolescents. WHO [6]
Major causes of mortality and morbidity among adolescents in selected regions
Source: progress for children: A report card on adolescents. UNICEF [8]
Decadal comparison of major causes of DALYs in adolescents by sexes in SEAR
Source: Health for world’s adolescents: Disability Adjusted Life Years. WHO [10]
Decadal comparison of State wise distribution of adolescent population
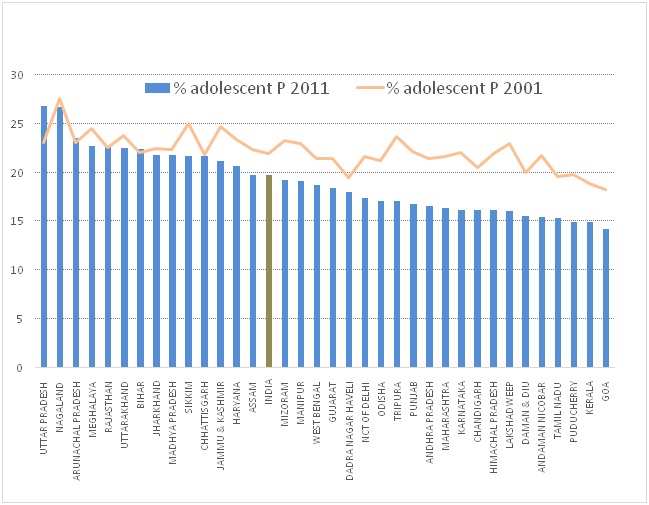
Adolescent’s percentage in the top and bottom five States
| Top Five State | % Adolescent | Bottom Five State | % Adolescent |
|---|
| Uttar Pradesh | 24.5 | Kerala | 16.3 |
| Rajasthan | 22.9 | Tamil Nadu | 17.2 |
| Uttarakhand | 22.5 | Karnataka | 18.9 |
| Bihar | 22.5 | Maharashtra | 19.0 |
| Jharkhand | 22.2 | Andhra Pradesh | 19.3 |
Reproductive and sexual health status of Indian adolescents
| S. No | Factors | Male (%) | Female (%) |
|---|
| 1 | Sexual debut before the age of 15+ | 2.7 | 8.0 |
| 2 | Contraceptive awareness (15-19)+ | 96.0 | 94.0 |
| 3 | Ever used Contraceptives+ | 29.4 | 40.4 |
| 4 | Condom used during first time+ | 19.0 | 3.0 |
| 5 | Births by age 18 (2008-2012)* | - | 21.7 |
| 6 | Comprehensive knowledge of HIV among adolescents+ | 34.5 | 18.6 |
| 7 | STI/ symptoms of STI in sexually active adolescents+ | 10.8 | 10.5 |
| 8 | Prevalence of HIV among adolescents+ | 0.01 | 0.07 |
*UNICEF [12] + NFHS 3 [13]
State wise adolescent fertility rates during 2011 and 2012
Adolescent health programmes, ministries and their services
| Sl. No | Ministries and Adolescent Health Programmes | Services |
|---|
| 1 | Ministry of health and family welfare |
| a | Adolescent reproductive and sexual health (ARSH) | Preventive, promotive, curative and counseling services for reproductive and sexual problems. |
| b | School health programme | Nutritional interventions, promoting health lifestyle, counseling and immunization |
| 2 | Women & Child Development |
| a | Kishori shakti yojana | Services improving health, nutritional and educational status of girls |
| b | Balika samridhi yojana | Services to raise the age of marriage and to improve enrollment and retention of girls at school |
| c | Rajiv Gandhi Scheme for Empowerment of Adolescent Girls | Iron and Folic Acid supplementation, nutrition & health education, ARSH, life skill education and vocational training for girls aged 16 and above under National Skill Development Program |
| d | Integrated program for street children | Shelter, nutrition, education, health care and recreation facilities to street children. Child Help Line Service (1098) |
| 3 | Human Resource Development |
| a | Sarva Shiksha Abhiyan | Free and compulsory education to 6-14 years age group |
| b | Mahila samakhya programme | Provides equal educational opportunities for women |
| c | Adolescent education program | Creates awareness and positive attitude to develop skills to enable them to respond to real life situations |
| 4 | Youth Affairs & Sports |
| a | Nehru yuva Kendra sangathan | Empowerment of rural youth |
| b | The national service scheme | Personality development of students through community service |
| c | National Program for Youth and Adolescent Development | Leadership qualities and personality development of youth |
| 5 | Others |
| a | Narcotic Drugs & Psychotropic Substances Act, 1985- AH Strategy | Prohibition on sale to minors |
| b | National AIDS Control Programme Phase –III | Appropriate referral of HIV/AIDS and RTI/STI cases |
Conclusion
To achieve wholesome adolescent health, we need to have a multidimensional approach covering all the adolescent health problems with special emphasis on mental health, behaviour change communication towards healthy lifestyle and positive social environment to acquire life skills. Adolescent friendly clinics need to be widely established throughout India and should achieve universal coverage. Screening of adolescent on regular basis could be an effective tool to control the existing disease and to update occurrence of any new diseases. Empower and involve adolescents in decisions that affect them and facilitate them with every opportunity for developing into a successful adult. Offering such opportunities to the growing children gives them a chance to build a safe, happy, healthy and productive nation in the future.
Exclusive data pertaining to the adolescent health issues in Indian scenario is not available when compared to the developed countries. Nation and States wise detailed investigation and reports on adolescent’s health issues, is the need of the hour. This will help to create better awareness among the stakeholders about the importance of strengthening adolescent health services under a single agency in order to meet their felt needs.
*UNICEF [
12] + NFHS 3 [
13]
[1]. Progress for Children: A report card on adolescents. Socio-demographic profile of adolescents: Number 10 April 2012 UNICEF. Figure: 2.1 Page 6 [Internet]. [cited 2014 November 20]. Available from: http://www.unicef.org/publications/files/Progress_for_Children_-_No._10_EN_04232012.pdf [Google Scholar]
[2]. Strategy Handbook. Rashtriya Kishor Swasthya Karyakram.Adolescent Health Division Ministry of Health and Family Welfare Government of India. January 2014 [Internet]. [cited 2014 September 8]. Available from: https://www.dropbox.com/s/0oj4p422y7st4ku/RKSK%20Strategy%20Handbook.pdf [Google Scholar]
[3]. Adolescents: health risks and solutions. Media centre Fact sheets WHO 2014 [Internet]. [cited 2014 September 8]. Available from: http://www.who.int/mediacentre/factsheets/fs345/en/ [Google Scholar]
[4]. Launch of Rashtriya Kishor Swasthya Karyakram and National Consultation on Adolescent Health. Ministry of Health and Family Welfare [Internet] 2014. [cited 2014 September 8]. Available from: http://rksklaunch.in/rkskl-strategy.html [Google Scholar]
[5]. Maternal, newborn, child and adolescent health. Adolescent health epidemiology WHO [Internet] 2014. [cited 2014 September 8]. Available from: http://www.who.int/maternal_child_adolescent/epidemiology/adolescence/en/ [Google Scholar]
[6]. Mortality, morbidity and disability in adolescence: Health for the world’s adolescents. Top 10 causes of death among adolescents by sex WHO 2014 [Internet]. [cited 2014 November 20]. Available from: http://apps.who.int/adolescent/second-decade/section/section_3/level3_2.php [Google Scholar]
[7]. C Abouzahr, C. Women’s health meeting: trends and projections for mortality and morbidity [Internet] 2013. [cited 2014 September 8]. Available from: http://icpdbeyond2014.org/uploads/browser/files/maternal_mortality_trends_and_projections.pdf [Google Scholar]
[8]. Progress for Children: A report card on adolescents. Adolescent Mortality, Morbidity and Health-Related Behaviours. Number 10 April 2012. UNICEF. Figure: 4.1. Page 18 [Internet]. [cited 2014 November 20] Available at http://www.unicef.org/publications/files/Progress_for_Children_-_No._10_EN_04232012.pdf [Google Scholar]
[9]. B Popkin, P Gordon-Larsen, The nutrition transition: worldwide obesity dynamics and their determinants. International Journal of Obesity [Internet]. 2004;28:2-9. [cited 2014 September 8]. Available from: http://www.cpc.unc.edu/projects/nutrans/publications/Popkin%20Nutr%20Trans%20IJO%202004.pdf [Google Scholar]
[10]. Health for world’s adolescents: Disability Adjusted Life Years: Combining Mortality and Morbidity. WHO May 2014 [Internet]. [cited 2014 November 20]. Available from: http://public.tableausoftware.com/profile/digitalteam#!/vizhome/shared/FPXZ7PPMR [Google Scholar]
[11]. C Chandramouli, Release of social and cultural tables: Age. Data highlights. August 2013. Census of India 2011 [Internet]. [cited 2014 December 8]. Available from: http://www.slideserve.com/varden/social-and-cultural-tables-age [Google Scholar]
[12]. Statistics. Adolescents: UNICEF. India [Internet] 2013. [cited 2014 September 8]. Available from: http://www.unicef.org/infobycountry/india_statistics.html [Google Scholar]
[13]. National Family Health Survey (NFHS-3), 2005–06: India: Volume I. International Institute for Population Sciences (IIPS) and Macro International. Mumbai: IIPS. September 2007. [cited 2014 November 20]. Available from: http://www.rchiips.org/nfhs/NFHS-3%20Data/VOL-1/India_volume_I_corrected_17oct08.pdf [Google Scholar]
[14]. SRS Statistical Report 2011. Sl. No.12, SRS Statistical Report Tables, Vital Statistics Ministry of Home Affairs [Internet]. [cited 2014 December 8]. Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Report/12SRS%20Statistical%20Report%20Table%20-%2020111.pdf [Google Scholar]
[15]. SRS Statistical Report 2012. Sl. No.12, SRS Statistical Report Tables, Vital Statistics Ministry of Home Affairs [Internet]. [cited 2014 December 8]. Available from: http://www.censusindia.gov.in/vital_statistics/SRS_Report_2012/12_SRS_statistical_report_tables_2012.pdf [Google Scholar]
[16]. T Ganchimeg, E Ota, N Morisaki, M Laopaiboon, P Lumbiganon, J Zhang, Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multi-country studyBJOG 2014 121(s1):40-48. [Google Scholar]
[17]. R Priyadarshini, S Jasmine, S Valarmathi, S Kalpana, S Parameswari, Impact of media on the physical health of urban school children of age group 11-17 yrs in Chennai - A cross sectional studyIOSR Journal of Humanities and Social Science 2013 9(5):30-35. [Google Scholar]
[18]. R Hancox, B Milne, R Poulton, Association between child and adolescent television viewing and adult health: a longitudinal birth cohort studyThe Lancet 2004 364(9430):257-62. [Google Scholar]
[19]. A Pillai, T Andrews, V Patel, Violence, psychological distress and the risk of suicidal behaviour in young people in IndiaInt J Epidemiol 2009 38(2):459-69. [Google Scholar]
[20]. V Patel, C Ramasundarahettige, L Vijayakumar, J Thakur, V Gajalakshmi, G Gururaj, Suicide mortality in India: a nationally representative surveyThe Lancet 2012 379(9834):2343-51. [Google Scholar]
[21]. S Malhotra, B Patra, Prevalence of child and adolescent psychiatric disorders in India: a systematic review and meta-analysisChild and adolescent psychiatry and mental health 2014 8(1):22 [Google Scholar]
[22]. M Rani, S Karunanidhi, Prevalence of depressive symptoms among urban adolescents in South IndiaJ Indian Assoc Child Adolesc Ment Health 2010 6(2):33-43. [Google Scholar]
[23]. J Jagnoor, W Suraweera, L Keay, R Ivers, J Thakur, P Jha, Unintentional injury mortality in India, 2005: nationally representative mortality survey of 1.1 million homesBMC public health 2012 12(1):487 [Google Scholar]
[24]. R Sharma, V Grover, S Chaturvedi, Health-risk behaviours related to road safety among adolescent studentsIndian J Med Sci 2007 61(12):656-62. [Google Scholar]
[25]. V Patel, G Andrew, Gender, sexual abuse and risk behaviours in adolescents: a crosssectional survey in schools in GoaNatl Med J India 2001 14(5):263-66. [Google Scholar]
[26]. V Tikoo, A Dhawan, R Pattanayak, A Chopra, Assessment of Pattern and Profile of Substance Use among Children in India [Internet] 2013. [cited 2014 September 8]. Available from: http://www.ncpcr.gov.in/view_file.php?fid=17 [Google Scholar]
[27]. DM Anglin, CM Corcoran, AS Brown, H Chen, Q Lighty, JS Brook, Early cannabis use and schizotypal personality disorder symptoms from adolescence to middle adulthood.Schizophr Res 2012 137(1-3):45-49. [Google Scholar]
[28]. B Sivakumar, Most of Tamil Nadu’s adolescents and youth live in rural areas, shows census. TNN | Nov 2, 2014 [Internet]. [cited 2014 December 8]. Available from: http://timesofindia.indiatimes.com/city/chennai/Most-of-Tamil-Nadus-adolescents-youthlive-in-rural-areas-shows-census/articleshow/45008956.cms [Google Scholar]
[29]. Implementation guide on RCH II: Adolescent reproductive and sexual health strategy. National Rural Health Mission. Service Delivery Package. Page 11-12 May 2006 [Internet]. [cited 2014 November 20]. Available from: http://countryoffice.unfpa.org/india/drive/ImplementationGuideFinal-RCH2ARSH.pdf [Google Scholar]
[30]. School Health Programme (SHP). Ministry of health and family welfare. Chapter 4.0: Key Elements. Page 7 [Internet]. [cited 2014 September 8]. Available from: http://www.mohfw.nic.in/showfile.php?lid=660 [Google Scholar]
[31]. Kishori Shakti Yojana. Ministry of women and child development. National Portal of India, 05 Jan, 2012 [Internet]. [cited 2014 September 8]. Available from: http://india.gov.in/kishori-shakti-yojana-ministry-women-and-child-development [Google Scholar]
[32]. Guidelines for the Balika Samriddhi Yojana. Ministry of women and child development. [Internet]. [cited 2014 September 8]. Available from: http://wcd.nic.in/BSY.htm [Google Scholar]
[33]. Rajiv Gandhi Scheme For Empowerment Of Adolescent Girls (RGSEAG) -‘SABLA’- The scheme. Ministry of women and child development 2010 Page 2 [Internet]. [cited 2014 September 8]. Available from: http://wcd.nic.in/SchemeSabla/SABLAscheme.pdf [Google Scholar]
[34]. An Integrated Programme for Street Children [Internet]. [cited 2014 September 8]. Available from: http://wcd.nic.in/streetchildscheme.htm [Google Scholar]
[35]. Sarva Shiksha Abhiyan. Ministry of human resource development. Department of School Education & Literacy, Elementary education 2007 [Internet]. [cited 2014 September 8]. Available from: http://ssa.nic.in/ [Google Scholar]
[36]. Mahila samakhya. Sectors Education Initiatives towards specific segments of the society. [Internet]. [Updated till December 9, 2012; cited 2014 September 8]. Available from: http://www.archive.india.gov.in/sectors/education/index.php?id=16 [Google Scholar]
[37]. Adolescent education programme. Ministry of human resource development. Department of School Education & Literacy, Elementary education 2011 [Internet]. [cited 2014 September 8]. Available from: http://mhrd.gov.in/adolesence_education [Google Scholar]
[38]. Nehru Yuva Kendra Sangathan. Ministry of Skill Development, Entrepreneurship, Youth Affairs & Sports 2012 [Internet]. [cited 2014 September 8]. Available from: http://www.nyks.org/aboutus/About-nyks.html [Google Scholar]
[39]. National Service Scheme. Ministry of youth affairs and sports. [Internet]. [cited 2014 September 8]. Available from: http://nss.nic.in/objectives.asp [Google Scholar]
[40]. National Programme for Youth and Adolescent Development. Ministry of Skill Development, Entrepreneurship, Youth Affairs and Sports [Internet]. [cited 2014 September 8]. Available from: http://yas.nic.in/sites/default/files/NPYAD%20Scheme%20Guidelines%20_1.pdf [Google Scholar]
[41]. Adolescent Health. National Health Mission Components: RMNCH+A: Adolescent Health 2013 [Internet]. [cited 2014 September 8]. Available from: http://nrhm.gov.in/nrhm-components/rmnch-a/adolescent-health/adolescent-health/background.html [Google Scholar]
[42]. J Stang, M Story, Guidelines for adolescent nutrition services 2005 1901st Edition:p21-34.University of Minnesota Chapter 3, Nutrition needs of adolescents [Google Scholar]
[43]. RM Anitha, BWC Sathiyasekaran, Mental Health symptoms and substance use among urban school going adolescentsJ. Indian Assoc Child Adolesc Ment Health. 2013 9(4):102-35. [Google Scholar]
[44]. Summary of Recommended Guidelines for Clinical Preventive Services for Young Adults ages 18-26: Risk Factors and Recommended Screening Tests. UCSF Division of Adolescent and Young Adult Medicine. Guidelines as of 02/2014. [Internet]. [cited 2014 September 8]. Available from: http://nahic.ucsf.edu/wp-content/uploads/2014/04/FINAL-Screening-Guidelines-4.11.pdf [Google Scholar]