Multimodality Imaging of Hemangiomas-Pictorial Essay
T. Arul Dasan1, Basawaraj N.G.2, Sunita Madhukar Anvekar3
1 Associate Professor, Department of Radio Diagnosis, Bangalore Medical College and Research Institute, Bangalore, India.
2 Associate Professor, Department of Radiodiagnosis, BGS Global Institute of Medical Sciences, Bangalore, India.
3 Consultant Radiologist, Department of Radiodiagnosis, PD Hinduja Sindhi Hospital, Sampangiramnagar, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr T. Arul Dasan, # 20, Mchs Colony, 5C Cross, 16 Main, BTM Layout 2 Stage, Bangalore-560076, India.
E-mail: arul_dsn@yahoo.co.in
Both hemangiomas and vascular malformations are endothelial malformations that closely resemble normal vessels and can be found in all organs of the human body. This pictorial essay encompasses a spectrum of imaging appearances of hemangiomas and vascular malformations. Familiarity of the MR and CT findings can help differentiate these lesions, to confirm the suspected diagnosis, classify the anomaly and document the associated abnormalities.
Common benign vascular neoplasm, Hemangioma, Spectrum of imaging appearances
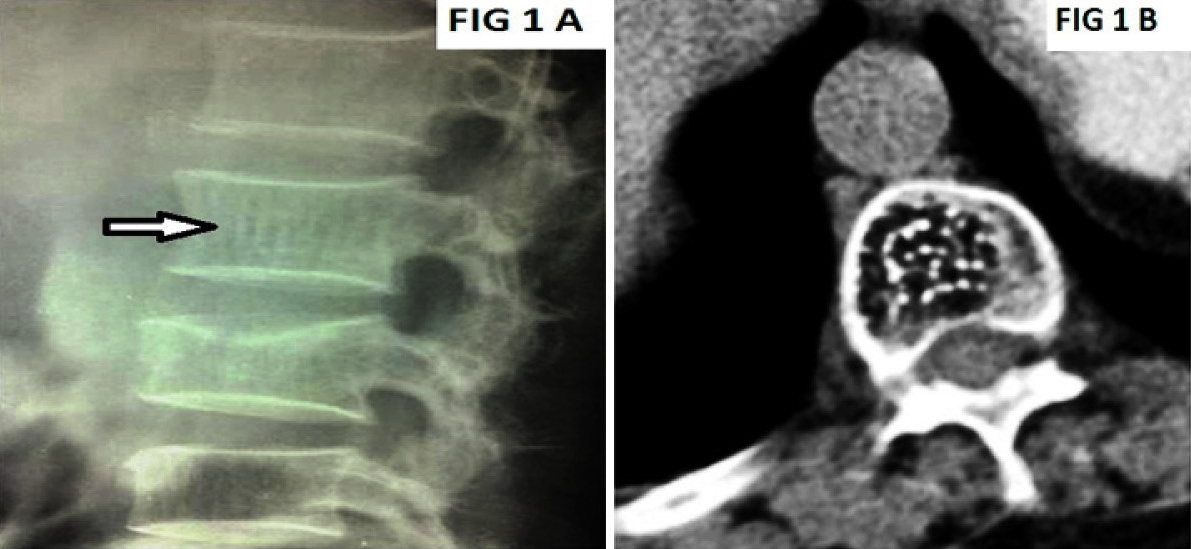
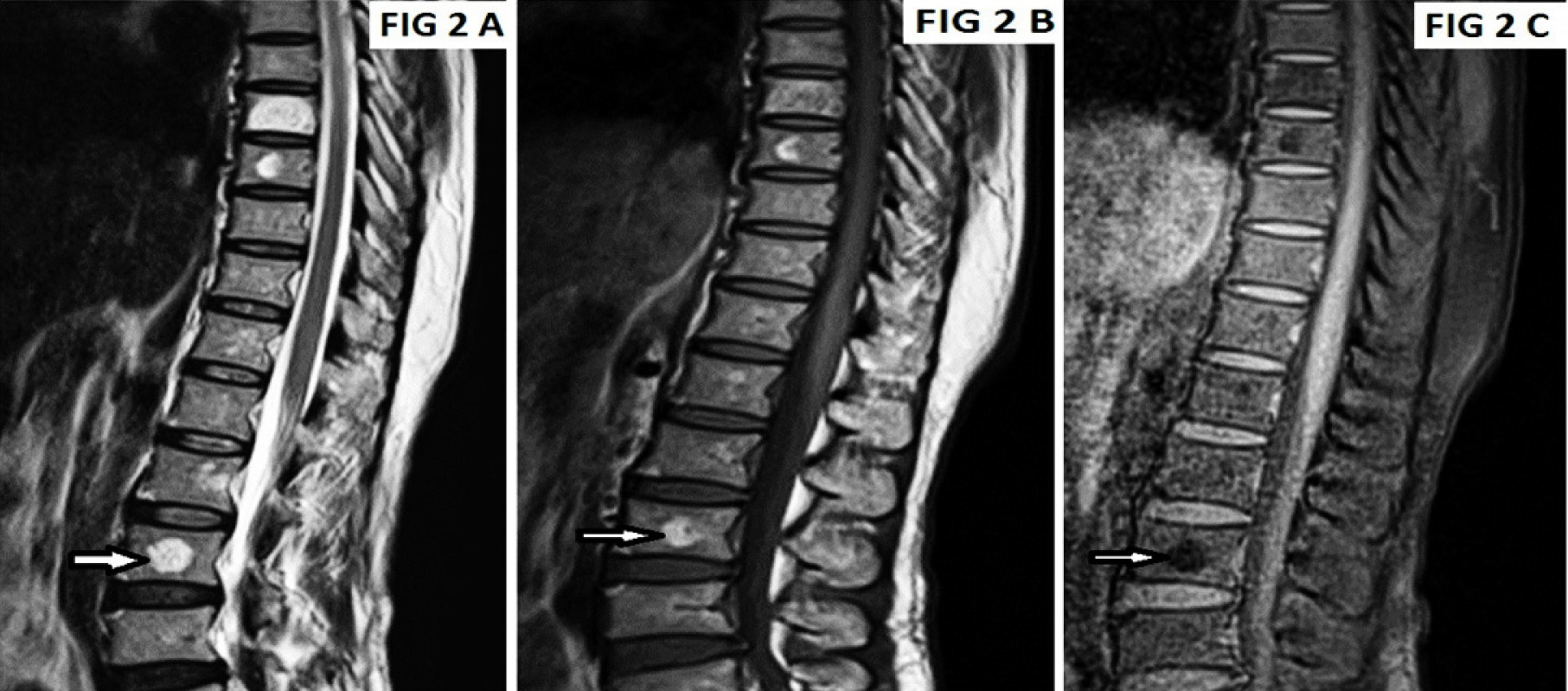
Conventional lateral radiograph of the lumbar spine [Table/Fig-1a] shows the classic corduroy cloth appearance (vertical striations) {white open arrow}, Axial CT of the lumbar spine [Table/Fig-1b] depicts polka dot appearance. Sagittal images of MRI spine T1WI [Table/Fig-2a], T2WI [Table/Fig-2b] and fat suppressed STIR images [Table/Fig-2c] show well defined oval lesions (white open arrow) involving lower thoracic and lumbar vertebrae appearing Hyperintense on T1WI and T2WI images and Hypointense on STIR images.
Vertebral hemangiomas (a) lateral view, (b) axial view
Vertebral hemangiomas (sagittal view)
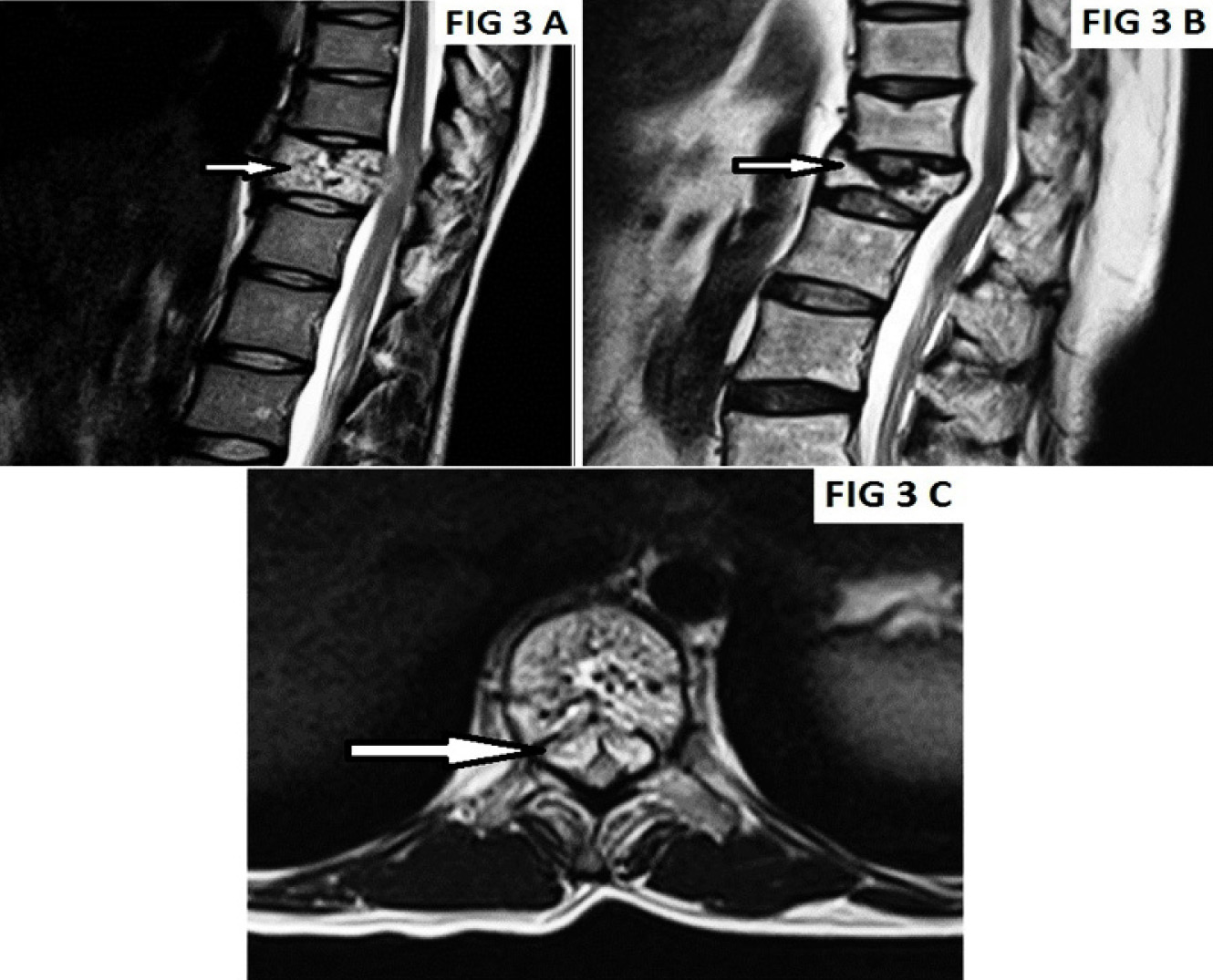
Sagittal T2W1 MRI images [Table/Fig-3a & b] show an aggressive hemangioma with associated epidural mass causing cord compression and vertebral collapse (White open arrow). Axial T1W1 images [Table/Fig-3c] show the compression collapse of the vertebral body and an epidural mass impinging the thecal sac with the cord (White open arrow).
Vertebral hemangiomas (a,b) sagittal view, (c) axial view
Imaging Findings
The thickened vertical trabeculae of hemangiomas cause parallel linear densities or a “jail bar” appearance (white open arrow) in the vertebral body on plain films. On axial computed tomography (CT), the remaining thickened trabeculae give a typical spotted appearance to the vertebral bodies [1]. MR is extremely sensitive in the detection of hemangiomas. On both T1-weighted and T2-weighted images, these lesions tend to have increased signal intensity [2]. Occasional hemangiomas within the bony confines can have a somewhat lower amount of adipose tissue and even appear diffusely hypointense [3]. MR is able to show paravertebral and epidural extension of tumour [1].
Lateral radiograph of the skull [Table/Fig-4a] shows a large soft tissue opacity (White open arrow) overlying the temporo parietal region causing lytic destruction of the underlying bones of skull vault. Ultrasonography (US) with colour Doppler [Table/Fig-4b] shows a heterogeneous hyper echoic lesion with significant vascularity. Contrast enhanced CT [Table/Fig-4c] and CT Volume rendered image [Table/Fig-4d] shows, heterogeneous intensely enhancing Lesion causing lytic destruction.
Giant hemangioma of scalp

Imaging Findings
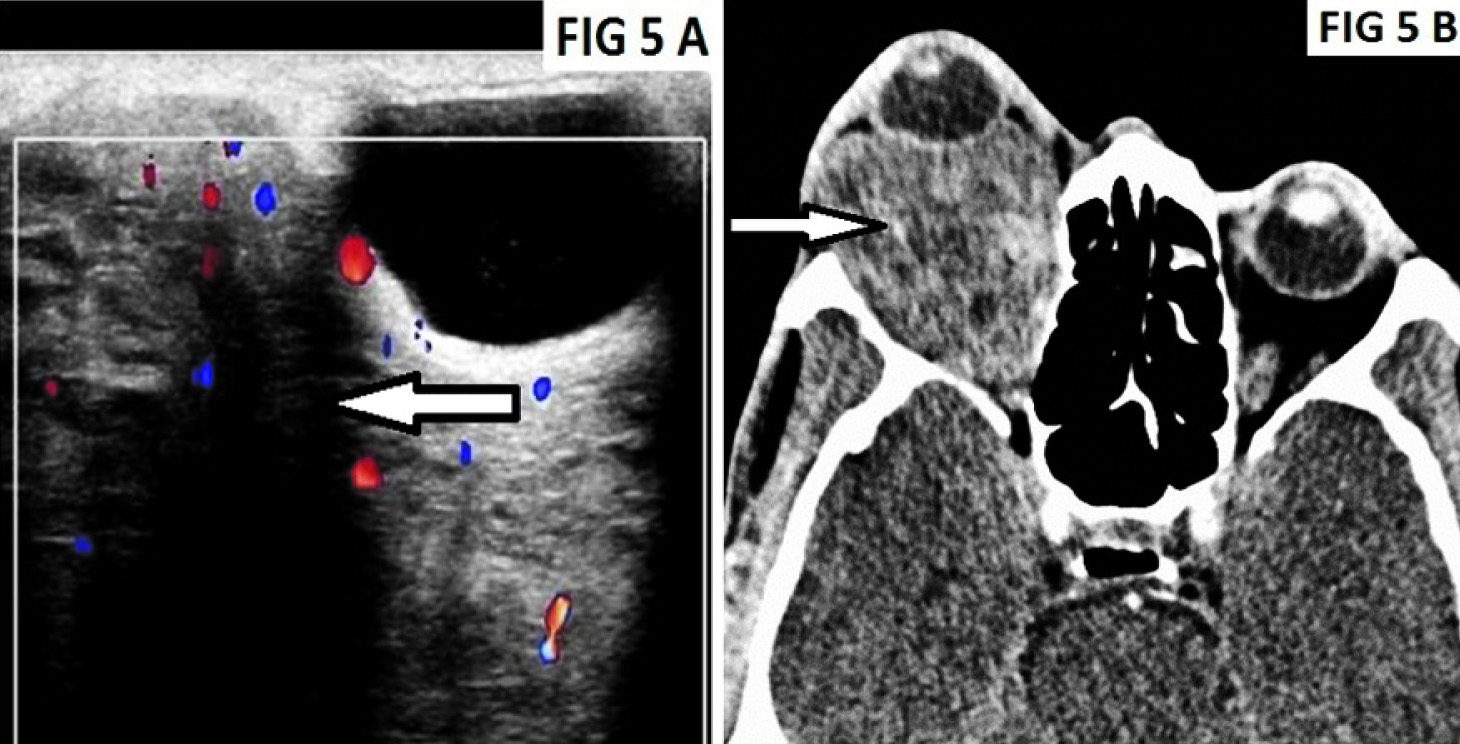
Nonenhanced CT usually shows a mass isodense with adjacent muscles with intense enhancement after intravenous contrast administration. Ultrasound shows a complex mass with calcifications and Doppler arterial signal with low resistive indices. On T1-weighted MR images, they appear as a poorly marginated and infiltrative mass with low to intermediate signal intensity. On T2- weighted images, the mass appears heterogenous with high signal vascular components and areas of fatty signals. Scintigraphy with blood pool agents show increased uptake [4,5].
US with Colour Doppler of the right orbit [Table/Fig-5a] shows a well defined heterogeneous lesion (White open arrow) with internal vascularity, Contrast enhanced CT scan of the orbits [Table/Fig-5b] show a well defined heterogeneously enhancing lesion, causing axial proptosis of right globe with a speck of calcification within (White open arrow).
Imaging Findings
CT is the preferred modality for the initial imaging evaluation because it can be performed without sedation. Because hemangiomas are nonencapsulated, they are usually lobulated, irregularly marginated, and heterogeneous and demonstrate intense homogeneous enhancement at CT after the administration of contrast material [6]. At US, hemangiomas appear hyperechoic [7].
Axial T2WI MRI [Table/Fig-6a] and Axial TWI post gadolinium MRI [Table/Fig-6b] of the left submandibular region shows an ill defined heterogeneous lesion involving skin and subcutaneous tissue of left submandibular region (white open arrow) which appears hyperintense on T2W1 and shows intense enhancement in post contrast study (white open arrow). MR Angiography [Table/Fig-6c] showing arterial supply by left facial artery (white open arrow).
Facial and soft tissue hemangioma

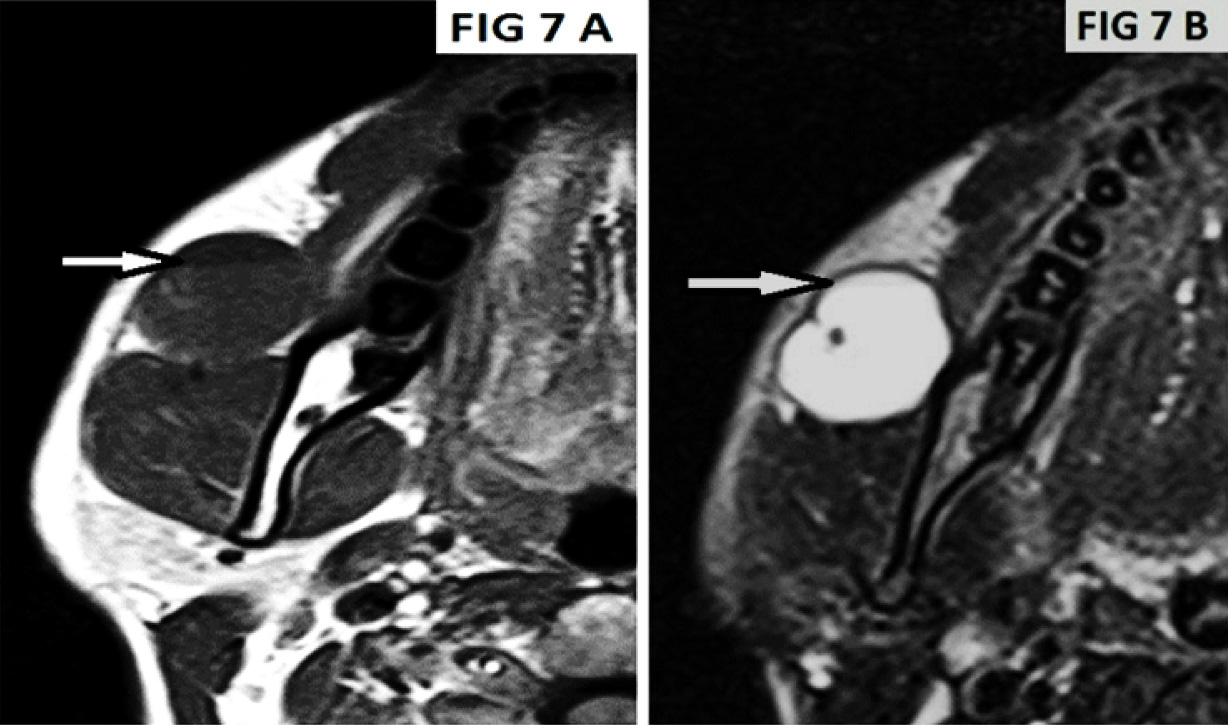
Axial T1WI MRI [Table/Fig-7a] and Axial T2WI MRI [Table/Fig-7b] in another patient shows a Well defined T1 hypointense and T2 hyper intense lesion in soft tissue of right submandibular region with fluid- fluid level (White open arrow) on T1 and T2WI images (suggestive of internal hemorrhage).
Facial and soft tissue hemangioma of right submandibular region
Imaging Findings
Most hemangiomas have typical MR appearance of low signal Intensity (similar to that of muscle) on T1-weighted images and high signal intensity (greater than that of subcutaneous fat) on T2-weighted images, which reflects the preponderance of fluid-filled cystic spaces [8].
Axial Non Contrast CT of brain [Table/Fig-8a] shows well defined hyperdense (White open arrow) lesions involving bilateral high parietal lobes, Axial T1WI MRI [Table/Fig-8b] of Brain shows Irregular hyper intense lesion in the left frontoparietal region, the lesion shows surrounding complete hypointense peripheral rim (Open White arrow) on Axial T2WI MRI [Table/Fig-8c] and blooming on Gradient sequences suggestive of hemosiderin (White open arrow) [Table/Fig-8d]. These findings are suggestive of Type I Cavernous angioma.

Imaging Findings
Recently three types of CA imaging appearances according to MR features were classified:
Type I
The presence of haemorrhage in cavernoma cavities; the hyperintense MR signal on T1-weighted images from the whole lesion structure. On T2-weighted images CA has hypo- or hyperintense signal from the central part of the lesion with low signal from the haemosiderin rim on the periphery.
Type II
“popcorn-like” lesion with a well-delineated, complex reticulated core with mixed MR signal intensities due to haemorrhages in different stages of evolution and calcifications.
Type III
The reflection of old haemorrhages; cavernous angioma has iso- or hypointense MR signal on T1-weighted images and diffuse hypointense signal on T2-weighted images [9].
Sources of The Images
All the images used in this study have been sourced from hospitals attached to Department of Radiodiagnosis, Bangalore Medical college and Research Institute (BMCRI).
The Following two Hospitals have been the sources of all the images:
Victoria Hospital, Bangalore, India.
Bowring and Lady Curzon Hospitals, Bangalore, India.
[1]. Neoplastic Disease of the Spine and Spinal Cord; chapter 26, p1514-15, Atlas, Scott W: Magnetic Resonance Imaging of the Brain and Spine 2009 4th EditionLippincott Williams & WilkinsCopyright © [Google Scholar]
[2]. Ross JS, Masaryk TJ, Modic MT, Vertebral hemangiomas: MR imagingRadiology 1987 165:165-69. [Google Scholar]
[3]. Tekkok IH, Acikgoz B, Saglam S, Vertebral hemangioma symptomatic during pregnancy—report of a case and review of the literatureNeurosurgery 1993 32:302-06. [Google Scholar]
[4]. Resnick D, Kyriakos M, Greenway GD, Tumours and tumour-like lesions of soft tissues. In: Resnick D, Kransdorf NJ,edsBone and joint imaging 2005 3rd edUSAElsevier Saunders:1219-20. [Google Scholar]
[5]. Kao SCS, Radiology of soft tissues in children. In: Grainger RG, Allison DJ, Adam A, Dixon AK,edsDiagnostic Radiology 2001 4th edChinaChurchill Livingstone:2154-56. [Google Scholar]
[6]. Bilaniuk LT, Orbital vascular lesions: role of imagingRadiol Clin North Am 1999 37:169-83. [Google Scholar]
[7]. Vu BL, Harris GJ, Orbital vascular lesionsOphthalmol Clin North Am 2000 13:609-31. [Google Scholar]
[8]. Siegel MJ, Glazer HS, St Amour TE, Rosenthal DD, Lymphangiomas in children: MR imagingRadiology 1989 170:467-70. [Google Scholar]
[9]. Kornienko VN, Pronin IN, Cerebrovascular Diseases and Malformations of the BrainIn: Diagnostic Neuroradiology ©2009 Springer-Verlag Berlin Heidelberg:311[e-ISBN 978-3-540-75653-8] [Google Scholar]