A Rare Case of Heterotopic Pregnancy with Ruptured Left Rudimentary Horn Pregnancy
Setu Rathod1, Sunil Kumar Samal2
1Assistant Professor, Department of Obstetrics & Gynaecology, Mahatma Gandhi Medical College & Research Institute, Puducherry, India.
2Assistant Professor, Department of Obstetrics& Gynaecology, Mahatma Gandhi Medical College & Research Institute, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sunil Kumar Samal 4-D, Type II Staff Quarters, Mahatma Gandhi Medical College, Pillaiyarkuppam, Puducherry-607402, India.
E-mail: drsksamal1981@gmail.com
Heterotopic pregnancy(HP) occurs when intrauterine and ectopic pregnancies coexist. We report a case of HP at 14 wk of gestation presenting as ruptured left rudimentary horn ectopic pregnancy with live intrauterine gestation and was managed with emergency laparotomy followed by resection of left rudimentary non communicating horn of uterus. The intrauterine pregnancy continued uneventfully. A female baby was delivered vaginally at 41 wk following induction of labour.
Emergency laparotomy, Ectopic pregnancy, Intrauterine pregnancy
Case Report
We report a case of a 22-year-old primigravida at 14 wk of gestation following spontaneous conception, presenting with pain abdomen for one day.This pregnancy was confirmed by urine pregnancy test following 40 d of amenorrhoea and she had one previous ultrasound report showing intrauterine pregnancy at 6 wk of gestation. There was no history of bleeding, spotting or passage of fleshy mass per vaginum. She had a nonconsanguineous marriage since 8 months. There was no history of excessive vomiting, fever, burning micturition, pelvic inflammatory disease or previous tubal surgery.
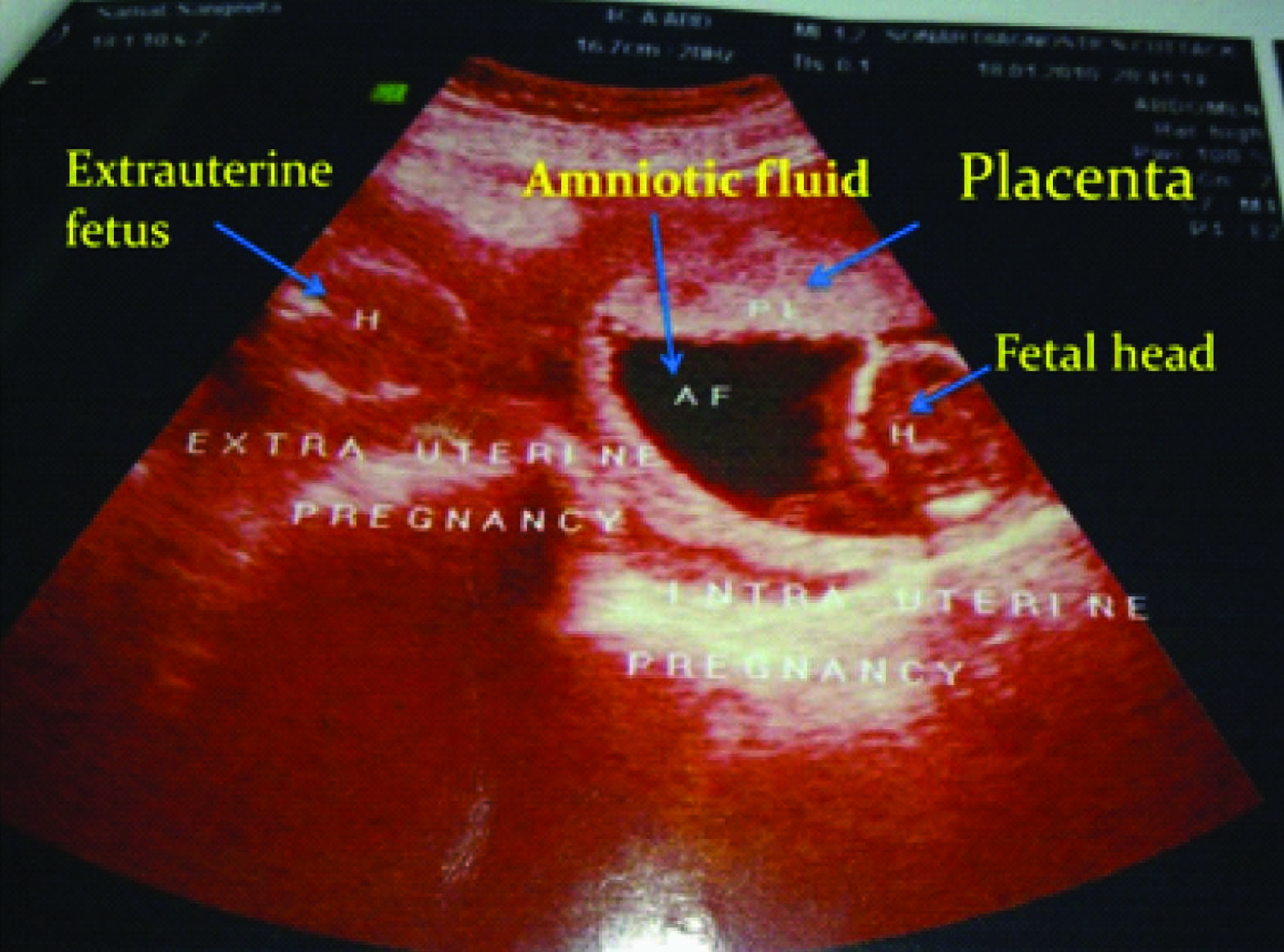
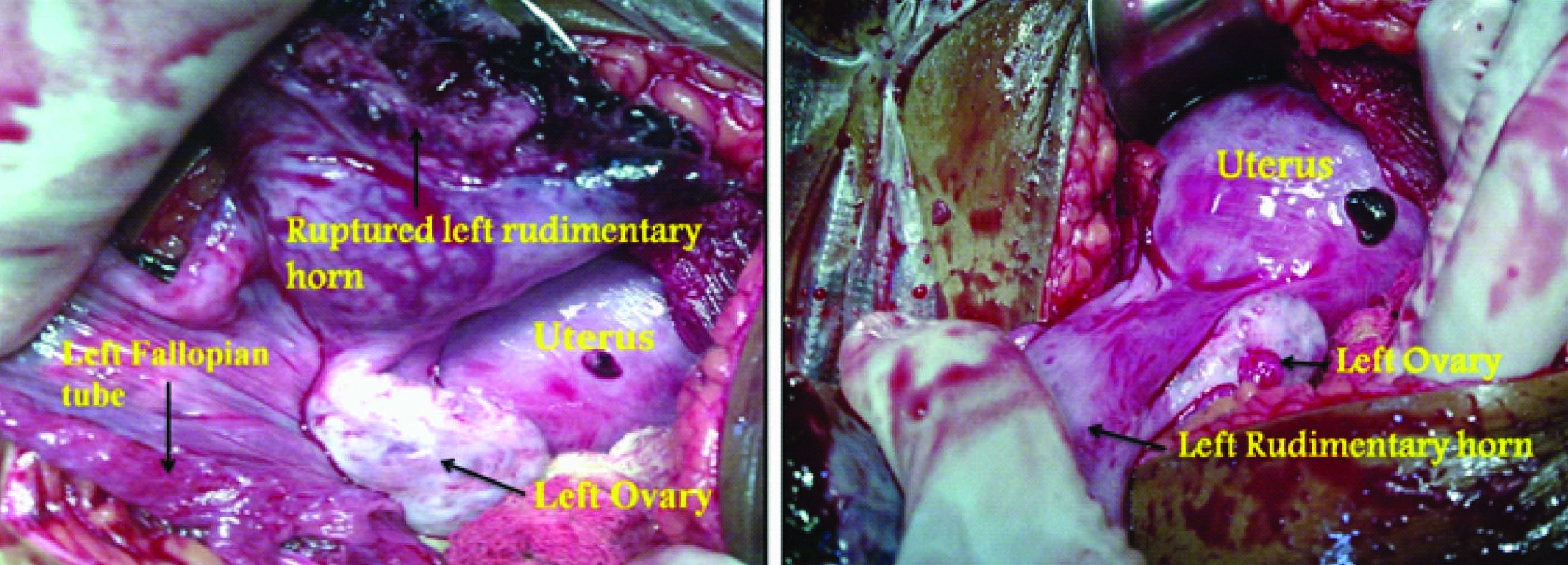
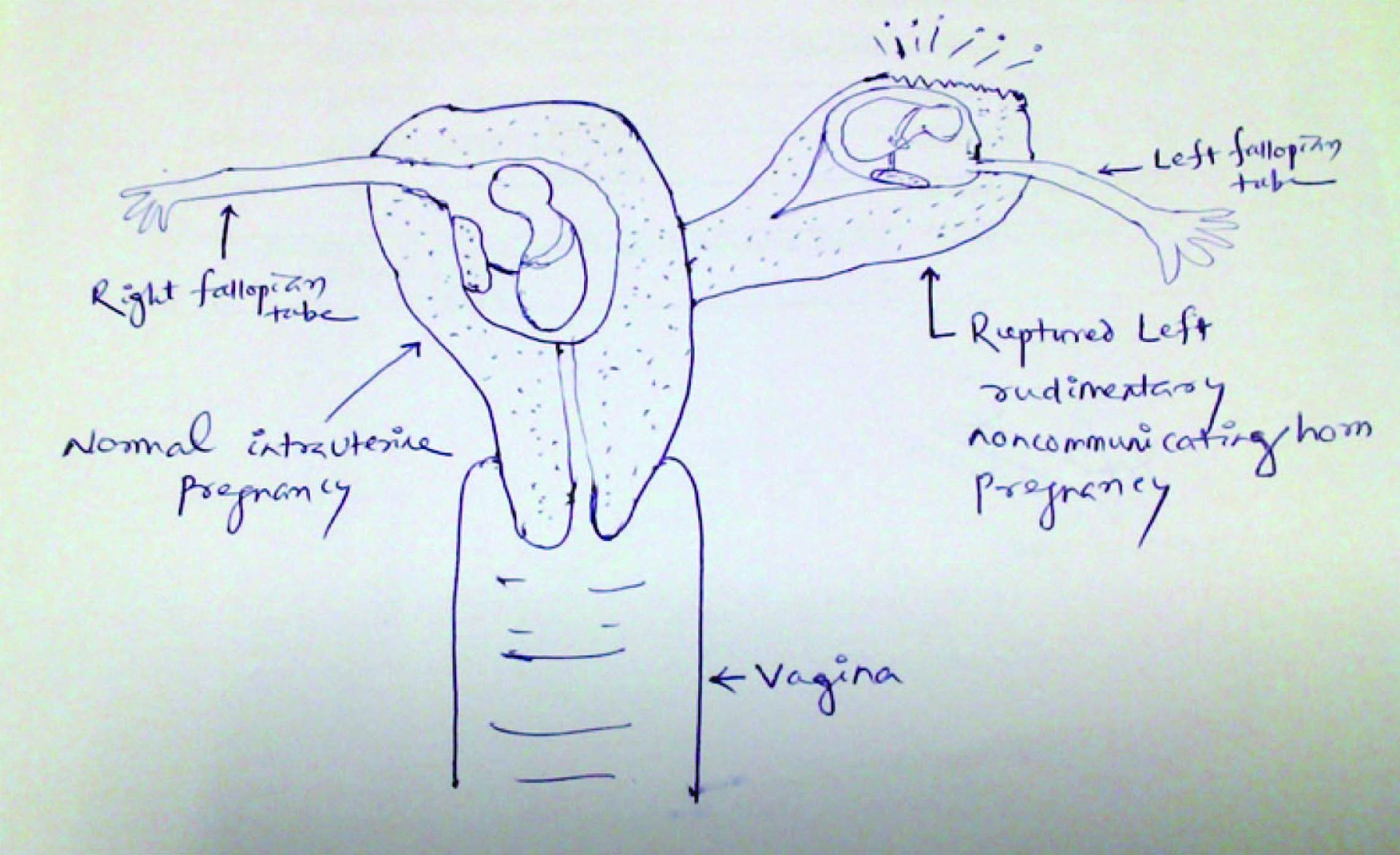
General examination revealed severe pallor with pulse rate-110/min, blood pressure-90/60 mm Hg. Other systemic examination revealed no abnormality. Abdominal examination revealed distended abdomen, suprapubic tenderness with shifting dullness present. There was no organomegaly or any mass felt per abdomen. On per speculum examination both cervix and vagina healthy with closed cervical os. Per vaginal examination revealed uterus14 week, all fornices were tender and full and cervical motion tenderness present. Investigation revealed her haemoglobin level as 8.0 gm/dl. Transabdominal ultrasonography showed moderate amount of fluid in the peritoneal cavity with a live intrauterine gestation of 14+1 wks. Another fetus of 14+4 wk seen without visualisation of cardiac activity with maternal bowel loops floating nearby with uterine wall not well-defined around it [Table/Fig-1]. Bilateral kidneys and ureters were normal. Provisional diagnosis of a heterotopic pregnancy with ruptured extra uterine pregnancy was made and planned for emergency laparotomy with concurrent hemodynamic stabilisation of patient’s condition. Intraoperatively ruptured left rudimentary non communicating horn pregnancy was found with hemoperitoneum of 1.5 litres. The left fallopian tube was healthy and found attached to left rudimentary horn [Table/Fig-2,3]. Both Samal2the ovaries with right fallopian tube were healthy and preserved. An extra uterine dead fetus of 14 wk gestation was found floating in the hemoperitoneum among bowel loops [Table/Fig-4]. Left rudimentary horn resection with left salpingectomy was done and the intrauterine live gestation was allowed to continue. Two units of blood was transfused postoperatively. Postoperative period was uneventful. The intrauterine pregnancy continued uneventfully. She delivered a healthy live baby vaginally following induction of labour at 41 wk of gestation. A sketch diagram is given below [Table/Fig-5] for better understanding of the case.
Discussion
A HP involves coexisting pregnancies at two different implantation sites. The most common combination is an intrauterine and an extra uterine gestation, most of which are in the tube (90%), but implantation in the cervix, ovary, interstitial segment, abdomen, and previous caesarean scar have been reported [1] . The incidence of HP is approximately 1 in 3,900 pregnancies [2] . The incidence has risen substantially due to increasing use of exogenous gonadotropins and assisted reproductive technique (ART) and is about 1.5/1000 pregnancies resulting from ART [3] .
HPs often escape early diagnosis because both serum beta-hCG concentration and Ultrasonography can be misleading. Serial beta-hCG levels are not helpful because the intrauterine pregnancy causes the beta-hCG level to rise appropriately and when Ultrasonography reveals an intrauterine pregnancy, the possibility of an ectopic pregnancy generally is excluded which has happened in our case. Consequently, diagnosis is delayed and over half of all HPs are recognised only after tubal rupture occurs [1] . Patients who have undergone ART procedures have a much higher incidence of heterotopic pregnancy than those who have a spontaneo conception [4] . Possible aetiology includes the hydrostatic force used to deliver the embryo into the cornual or tubal area, the tip of the catheter directing transfer towards the tubal ostia, or reflux of uterine secretions leading to retrograde tubal implantation [5] . HP can occur without any identifiable risk factors, and the detection of intra-uterine pregnancy does not exclude the possibility of the simultaneous existence of ectopic pregnancy. Shetty SK et al., reported a case of HP with tubal rupture with no identifiable risk factors [6] . Gruber I et al., reported that previous tubal surgery is a risk factor for HP [7] . In our case, heterotopic pregnancy occurred following spontaneous conception and no identifiable risk factors were found.
Most of the reported cases of HPs were singleton intrauterine with extrauterine pregnancies. Alsunaidi MI et al., reported a rare case of spontaneous triplet pregnancy [8] . The signs and symptoms of HP are similar to those of ectopic pregnancy but, unfortunately, are often dismissed. Treatment of HP is complicated by the coexisting intrauterine pregnancy. Expectant management is inappropriate because neither serum beta-hCG level nor Ultrasonography can accurately determine the fate of the ectopic pregnancy and the risk of rupture. Systemic or local methotrexate injection is contraindicated due to the detrimental effects on the normal intrauterine pregnancy [1] . Selective embryo reduction by direct local injection of potassium chloride [9] or hyperosmolar glucose [10] in to the ectopic gestational sac under ultrasound or laparoscopic guidance can be done. Otherwise, surgical treatment by salpingostomy or salpingectomy is considered as the treatment of choice [11] . In our case, the extra uterine pregnancy was in the rudimentary non communicating left horn which is a rare form of ectopic pregnancy. Since the diagnosis of HP was made late at 14 wk after the rupture of left rudimentary horn followed by severe internal bleeding, emergency laparotomy with resection of left rudimentary horn of uterus was done. Tal J et al., reported 66% survival rate of the intrauterine pregnancy of a patient with a diagnosis of heterotopic pregnancy after surgical treatment [12] . Such a catastrophe can be prevented by early diagnosis through extensive adnexal scanning during initial antenatal visits.
Ultrasound showing both intra and extra uterine foetuses
Rupture left rudimentary non communicating horn of the uterus
Extra uterine foetus of 14 wk of gestation

Sketch for heterotopic pregnancy occuring in an unusual location (Rudimentary horn)
Conclusion
In summary, we presented a case of live intrauterine pregnancy with ruptured left rudimentary horn pregnancy following spontaneous natural conception which is extremely rare. Hence, a high index of suspicion should be done to ensure early diagnosis and management following a timely intervention that can result in a successful outcome of intrauterine pregnancy which can prevent catastrophic events like rupture and hemorrhagic shock.
[1]. MA Fritz, L Speroff, Ectopic Pregnanccy. In: Fritz MA, editor. Clinical Gynecological Endocrinology and Infertility 1977 8th EditionNew DelhiWolters Kluwer Health/Lippincott Williams & Wilkins:1408-09. [Google Scholar]
[2]. PJ Cheng, HY Chueh, JT Qiu, Heterotopic pregnancy in a natural conception cycle presenting as hematometraObstet Gynecol 2004 104:1195 [Google Scholar]
[3]. HB Clayton, LA Schieve, HB Peterson, DJ Jamieson, MA Reynolds, VC Wright, A comparison of heterotopic and intrauterine-only pregnancy outcomes after assisted reproductive technologies in the United States from 1999 to 2002FertilSteril 2007 87:303-87. [Google Scholar]
[4]. AJ Voedisch, CE Frederick, AF Nicosia, TG Stovall, Early pregnancy loss and ectopic pregnancy. In: Bereck JS, editor. Berek & Novak’s Gynecology 2012 15th EditionNew DelhiWolters Kluwer Health/Lippincott Williams & Wilkins:645 [Google Scholar]
[5]. JO Schorge, JI Schaffer, LM Halvorson, Ectopic Pregnancy. In: Schorge JO, editor. Williams Gynaecology 2008 1st EditionNew New YorkMcGraw Hill Medical:170 [Google Scholar]
[6]. SK Shetty, AK Shetty, A case of heterotopic pregnancy with tubal ruptureJ Clin Diagn Res 2013 7(12):3000-1. [Google Scholar]
[7]. I Gruber, J Lahodny, K Illmensee, A Losch, Heterotopic pregnancy: Report of three casesWien Klin Wochenschr 2002 114(1):229-32. [Google Scholar]
[8]. MI Alsunaidi, An unexpected spontaneous triplet heterotopic pregnancySaudi Med J 2005 26:136-38. [Google Scholar]
[9]. LJ Salomon, H Fernandez, A Chauveaud, S Doumerc, R Frydman, Successful management of a heterotopic Caesarean scar pregnancy: potassium chloride injection with preservation of the intrauterine gestation: case reportHum Reprod 2003 18:189 [Google Scholar]
[10]. H Strohmer, A Obruca, R Lehner, C Egarter, P Husslein, W Feichtinger, Successful treatment of a heterotopic pregnancy by sonographically guided instillation of hyperosmolar glucoseFertilSteril 1998 69:149 [Google Scholar]
[11]. JS Goldstein, VS Ratts, T Philpott, MH Dahan, Risk of surgery after use of potassium chloride for treatment of tubal heterotopic pregnancyObstetGynecol 2006 107:506 [Google Scholar]
[12]. J Tal, S Haddad, N Gordon, I Timor-Tritsch , Heterotopic pregnancy after ovulation induction and assisted reproductive Technologies: A literature review from 1971 to 1993Fertil Steril 1996 66:1-12. [Google Scholar]