Recurrent aphthous stomatitis (also referred to as aphthae or canker sores) is one of the most common oral ailments. The disease is characterized by recurring painful ulcers of the mouth that are round or ovoid with a crater form base covered by a grey white pseudo membrane and surrounded by a distinct erythematous halo [1]. Evidence based studies suggest that recurrent aphthous stomatitis is reported to occur more commonly among women of high socio economic group under the age of 40 y [2].
As documented well in the literature, this disease entity is as a result of culmination of varied multi factorial aetiology which includes hereditary, environmental, infection due to various microorganisms, deficiencies of iron and vitamin B, etc [3]. Neverthless, the previous studies have proved that neither iron nor vitamin supplements has decreased the ulcer symptoms. The likelihood of association of microorganism and apthous ulceration is proven to be absurd [4]. As aetiology is poorly understood, treatment options are largely palliative and aimed at reducing symptoms thereby improving oral comfort. Reducing pain and healing time for recurrent aphthous ulcers restores the ability to eat swallow and improve the quality of life of those people suffering from this condition.
Research and development in the field of medicine has revolutionized therapeutics. Integrating ozone therapy is one such revolution in the treatment of oral diseases. Ozone is found to work effectively when applied topically to the affected cutaneous and mucosal sites. Neverthless, the ozone is unstable. This unstable form of ozone molecules is stabilized with the monounsaturated fatty acid such as oleic acid. This product obtained as ozonated oil is employed to treat the abnormal cutaneous and mucosal areas of the body [5,6]. There have been few studies on therapeutic effects of ozonated oil in recurrent aplhous ulceration. The application of ozonated oil has been widely used with better results achieved in oral diseases.
Sesame oil which is regarded as “queen of oils” is an edible oil which is extracted from sesame seeds. Literature supports the use of this oil as a house hold remedy to maintain the oral health. The evidence based research suggest the use of sesame oil in treating RAS patients owing to its inherent antimicrobial and anti- inflammatory activity which enhances in alleviating the pain symptoms there by fastening the wound healing [7,8].
With this back ground the present study was done to compare the effectiveness of ozonated oil and sesame oil for shortening of healing time and improving pain control.
Materials and Methods
The present study was carried out among the subjects reported to the Department of Oral Medicine, Oral Diagnosis and Radiology, Vishnu Dental College, Bhimavaram, Andhra Pradesh, India. The study was undertaken during the period from October 2013 to June 2014.
A randomized single blinded, placebo controlled study was carried out on 30 subjects of either sex above the age of 16 y. Diagnosis of aphthous ulcers was made on the basis of history and clinical symptoms. Each patient was explained about the need for the study and intervention to be conducted on them. A written informed consent was obtained from each subject before enrollment into the current study. Ethical approval was obtained for this study from the Institutional Research Ethics Committee. The present clinical study was performed in accordance with the ethical standards formulated in the Helsinki Declaration version 2000.
A total of 30 subjects were included in the study and were divided into three equal groups.
Group 1: Subjects receiving ozonated oil (Ozone forum, Pvt. Ltd, Mumbai)
Group 2: Subjects receiving sesame oil (Tilsona oil, natural sesame oil product available in market)
Group 3: Subjects receiving placebo agent. (Distilled water)
Blinding: Patients with recurrent aphthous ulcer were randomly assigned to one of the three treatment groups. The treatment agents and placebo agents were packed in identical looking containers and coded as A, B and C and distributed to Group I, II, III respectively. All the subjects participated in the study were blinded to the treatment and placebo agents.
Inclusion criteria: Patients of both sexes above the age range of 16 y were included in the study. Subjects having 1 to 5 ulcers, with duration of less than 48 hours of appearance located on reachable sites of oral mucosa that limited the activities such as talking, eating or carrying out oral hygiene were included in the study. The most painful ulcer identified by the patient was selected as the index ulcer for study.
Exclusion criteria: Subjects with less than two episodes of recurrent apthous ulcers, ulcers that lasted more than seven days in previous episode, patient with any systemic disease and under systemic or topical corticosteroid therapy, immunomodulating agent or patient using any of the medications were excluded from this study. Female subjects who were pregnant or breast feeding were also excluded.
Therapeutic regimen for both the study groups: Topical application of the medication with a cotton tipped applicator over the ulcers four times per day for five days. Patient was advised not to consume any solid or liquid diet half an hour before after the application of medication. During each application two drops (approximately 0.2 ml) of the agent was applied directly on the ulcer. After subsequent treatment days subjects were assessed for the parameters including: duration of pain reduction after application, healing of ulcer, onset of size reduction after application.
Data collection and outcomes: During the subject’s initial appointment, all the data required for the study were collected. This data includes demographic details, general examination details and patient’s past history of the lesions etc. The routine oral examination was carried out to identify the aphthous ulceration. An aphthous ulcer was diagnosed based on the presence of its appearance which is seen as a crateriform ulcer with a well defined round border surrounded by an erythematous halo.
The ulcers were evaluated clinically based on the ulcer size, severity of erythema, pain as reported by the patient and overall assessment of these clinical features. The evaluations were repeated on 2nd, 4th, 6th day of the treatment. On clinical examination, pain intensity was recorded using a visual analog scale (VAS) of 0-10 (with 1 mm division, where ‘0’ is no pain and ‘10’ is worst possible pain), size of each ulcer (a graduated periodontal probe was used to measure the ulcer size at the maximum diameter of the ulcer), and severity of erythema was recorded by using erythema grade scale (0-3).
After complete clinical examination of the ulcer pretreatment photographs were taken before the start of the treatment and were compared with the post treatment photographs which were taken at the patient’s consecutive visits to evaluate the effect of treatment.
Changes of the index ulcer’s size during the compared treatments were measured using a similar methodology to the one described by khandwala et al., [9].
Grade Description of Ulcer
Grade 4 = Aphthous ulcer cleared.
Grade 3= Marked improvement (the ulcer is barely perceptible with minimal or no pain and marked decrease in size).
Grade 2 = Moderate improvement (the ulcer is visible with moderate decrease in erythema and a moderate decrease in pain and moderate decrease in size).
Grade 1 = Slight improvement (the ulcer is visible with a slight decrease in size, minimal decrease in erythema and a slight decrease in pain).
Grade 0 = No change from the Day 1 = Aphthous ulcer worsened (greater erythema and/or pain or size).
Statistical Analysis
Descriptive and inferential statistical analysis was carried out in the present study. Results on continuous measurements were presented on Mean ± SD (Min-Max) and significance was assessed at 5 % level of significance. Statistical test Wilcokson signed rank test and Friedman test for comparison of the study and the control group and for comparision of parameters obtained at different time periods with the baseline values within the group itself was used. P-value of <0.05 was taken as statistically significant.
Results
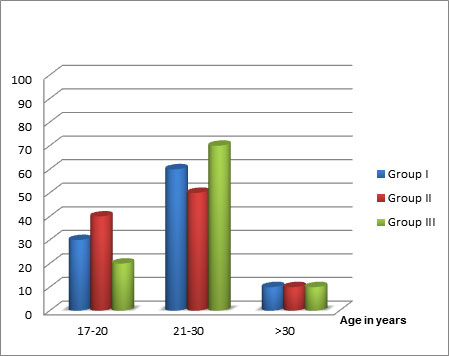
The mean age of subjects in Group I is 23.00±4.78, Group II is 22.30±4.27 and in Group III is 22.90±4.31 [Table/Fig-1,2].
Age distribution of patients studied in all the three groups
| Age in years | Group I | Group II | Group III |
|---|
| No | % | No | % | No | % |
|---|
| 17-20 | 3 | 30.0 | 4 | 40.0 | 2 | 20.0 |
| 21-30 | 6 | 60.0 | 5 | 50.0 | 7 | 70.0 |
| >30 | 1 | 10.0 | 1 | 10.0 | 1 | 10.0 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 |
| Mean ± SD | 23.00±4.78 | 22.30±4.27 | 22.90±4.31 |
Age distribution of patients studied in all the three groups
The gender distribution of subjects studied in Group I, were 8 (80%) females, 2 (20%) males.In Group II 6(60%) were females, 4 (40%) were males. In Group III, 7 (70%) were females, 3 (30%) were males [Table/Fig-3].
Gender distribution of patients studied in all the three groups
| Gender | Group I | Group II | Group III |
|---|
| No | % | No | % | No | % |
|---|
| Female | 8 | 80.0 | 6 | 60.0 | 7 | 70.0 |
| Male | 2 | 20.0 | 4 | 40.0 | 3 | 30.0 |
| Total | 10 | 100.0 | 10 | 100.0 | 10 | 100.0 |
Pain incidence in VAS score: The mean pain score at base line for the patients of Group 1 was 8.10 ± 0.70. The mean pain scores on day 2, 4 and 6 were 6.50±0.90 4.10±1.00 and 1.50±0.70, respectively. The mean pain score at base line for the patients of Group 2 was 8.20±0.79. After treatment the mean pain scores on day 2, 4 and 6 were 5.70±0.82, 3.50±0.97and 1.80±0.79 respectively. The mean pain score at base line for the patients of Group 3 was 7.90±0.74. After treatment the mean pain scores on day 2, 4 and 6 were 7.60±0.52, 7.40±1.07 and 4.60±0.70respectively. These data [Table/Fig-4,5,6] depicts a significant reduction in pain in Group 1 and Group 2 when compared with Group 3. (p-value < 0.05 using Wilcokson signed rank test)
pain in vas score Group I
| Time interval | Mean VAS ±SD | Difference from baseline | p-value |
|---|
| Pretreatment | 8.10±0.70 | — | — |
| DAY 2 | 6.50±0.90 | 1.60±0.20 | 0.007 S |
| DAY4 | 4.10±1.00 | 4.00±0.30 | 0.004 S |
| DAY 6 | 1.50±0.70 | 6.60±0.00 | 0.005 S |
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
pain in vas score Group II
| Time interval | Mean VAS ±SD | Difference from baseline | p-value |
|---|
| Pretreatment | 8.20±0.79 | — | — |
| DAY 2 | 5.70±0.82 | 2.50±0.03 | 0.004 S |
| DAY4 | 3.50±0.97 | 4.70±0.18 | 0.004 S |
| DAY 6 | 1.80±0.79 | 6.40±0.00 | 0.004 S |
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
pain in vas score Group III
| Time interval | Mean VAS ±SD | Difference from baseline | p-value |
|---|
| Pretreatment | 7.90±0.74 | — | — |
| DAY 2 | 7.60±0.52 | 0.30±0.22 | 0.083 NS |
| DAY4 | 7.40±1.07 | 0.50±0.33 | 0.059 NS |
| DAY 6 | 4.60±0.70 | 3.30±0.04 | 0.005 S |
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
Incidence of the ulcer healing: (grade description of the ulcer)The overall ulcer healing as described according to khandawala et al., is considered in the present study. The results revealed significant reduction of ulcer in Group 1 on day 2 (2.00±0.82) and day 4 (3.20±0.79) when compared to Group 2 and 3. On day 6 significant reduction is observed in both Group 1 (3.70±0.48) and 2 (3.10±0.74) when compared to Group 3 value (p-value < 0.05 using Friedman test) [Table/Fig-7].
Assessment of ulcer healing in all the three groups
| GROUPS | DAY 2 Difference from Baseline | DAY4 Difference from Baseline | DAY 6 Difference from Baseline | Friedman test |
|---|
| Mean±SD | Mean±SD | Mean±SD | p-value |
|---|
| GROUP I | 2.00±0.82 | 3.20±0.79 | 3.70±0.48 | 0.002 Significant |
| GROUP II | 0.90±0.74 | 2.40±0.52 | 3.10±0.74 | 0.001 Significant |
| GROUP III | 0.20±0.42 | 0.30±0.48 | 0.40±0.52 | 0.687 Not Significant |
Friedman test. Statistically significant if p<0.05
Discussion
Recurrent aphthous ulceration (RAU) seems to be an age old disease which is mainly related to the host’s immune reaction. There is no definite cure for this condition. These ulcerations are the most common oral disorders which affects 20% of the population atleast once or twice in their lives [10,11].
Recurrent aphthous ulceration is a painful and debilitating problem for patients, particularly when multiple ulcers occur simultaneously. In case of recurrent aphthous stomatitis, the diagnosis is truly based upon the clinical appearance of the lesion and no single laboratory test exists to confirm its diagnosis. Nevertheless, a thorough clinical history and examination helps to identify a secondary cause if any [2].
As the exact aetiology of aphthous ulceration is poorly understood treatment options are largely palliative and aimed at reducing symptoms thereby improving patient’s oral condition [11]. One such novel method in the field of medicine which is totally aimed at reducing the size of ulcer and comforting the patient is ozone therapy. There are few reports of ozone as a treatment modality in curing the chronic ulcers of leg in the literature. The earliest report was dated in 1957 and then Thwaites and Dean in 1985 who reported the beneficial effects of ozone on the healing of leg ulcers [12].
Owing to its varied inherent clinical properties, Ozone (O3) is renowned as one of the best bactericidal, antiviral and antifungal agents. This form of ozone is being used empirically as a clinical therapeutic agent for chronic wounds, such as trophic ulcers, ischemic ulcers and diabetic wounds [13,14]. Ozone is a gas with an allotropic form of oxygen with three atoms which is obtained by subjecting oxygen to silent electrical discharges through special equipment called ozonizers. As it is very reactive and unstable with a half-life of just a few minutes, it cannot be stored. So, it is dissolved in an oil base, with a life span measured in years. O3 is profitably and practically employed as ozonized sesame oil. Because of their antimicrobial, immunostimulating, analgesic, antihypoxic and detoxicating properties, ozonated oils have been empirically used for treating aphthous ulceration [15,16].
Sesame oil has been used as healing oil for thousands of years because of its inherent antimicrobial and natural anti-inflammatory activity which enhances in alleviating the pain symptoms there by fastening the wound healing [7].
In the present study the mean age of subjects studied in all the groups were with in the range of 18-25 y with female predominance, which correlates with highest incidence of aphthous ulceration in females.
In the present study patients treated with ozonated oil showed significant reduction of ulcer size, erythema and pain in successive treatment days in comparison to pretreatment period than the other two groups. On comparision between the groups there was significant reduction of overall ulcer healing on 2nd and 4th day of evaluation in Group 1. On day 6 significant reduction is observed in both Group 1 and 2 when compared to Group 3. No significant difference was observed in subjects within the placebo group. The results imply that ozone has inherent healing effects than sesame oil and placebo.
Few studies have explored the therapeutic effectiveness of ozonated oil in recurrent aphthous ulceration. Richard Logan, has documented the clinical application of topical ozone to the ulcer using Healozone appliance which provided an effective means of producing resolution of clinical symptoms because of its wide variety of antimicrobial, immunostimulating, analgesic property [17].
Hee su kim et al., conducted an in-vitro study to evaluate the therapeutic effects of topical ozonated oil on acute cutaneous wound healing in a guinea pig model. The results showed there is an Increased expression of PDGF, TGF-β, and VEGF which accelerated the wound healing [5]. Ozone leads to a higher expression of cytokines that are important for wound healing, especially TGF -β an important substance for regulation and coordination in the initial wound healing phase. A comparative study conducted by Heyam S Ali et al., for assessing the efficacy of sesame oil based propolis paste in patients with recurrent aphthous ulceration showed significant reduction of pain, size of aphthous ulcers and complete healing. The high effectiveness of the sesame oil could be attributed to the longer duration of adherence of its base to the site of ulcer that allows the active ingredients to diffuse completely and to act for a long period of time [18].
Signs and symptoms in Group 1 and Group 2 had reduced when compared to Group 3 which was noted by reduction in the VAS scores throughout treatment and post-treatment period. Although significant pain reduction was present in both the groups, the rate of pain reduction was faster in ozonated oil group, emphasizing the therapeutic efficacy of ozone.
Our results are similar to the study conducted by Maria del Carmen Sori Gort suggesting that the diverse biochemical properties of ozone help in alleviating RAS pain [13]. Faleh A Sawair conducted a cross-sectional survey to determine prevalence and type of treatments used by patients with RAS, 39.5 % of the subjects used sesame oil, this is attributed to the fact that innate anti -inflammatory property of sesame oil aids in pain relief [19].
While comparing the effectiveness of ozonated oil with sesame oil, ozone with its wide variety of inherent properties has proven to be choice of treatment in completely relieving the ulcer pain and ulcer size when compared with that of its counter medication (i.e. sesame oil).
None of the patients in our study reported any serious adverse effects. In the ozonated oil group, three patients experienced a transient bitter sensation shortly following the application of the ozonated oil.
Conclusion
The use of ozonated oil in treating recurrent aphthous ulcer is found to achieve better results in significantly showing effective changes in the ulcer size reduction, duration of complete healing and pain relief. Nevertheless, small sample size remains the main limitation in the current study. The study has to be carried out in a larger sample to make ozone (ozonated oil) an effective and novel treatment approach for recurrent aphthous ulcer. Ozone provides a new path in recurrent aphthous ulcer treatment owing to its wide range of inherent properties which benefits the patient, with its cost effective and ease of use.
Cure for sure, relieve to believe. Confront to comfort - “Ozone on a high zone”.
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
Wilcoxon signed rank test. Statistically significant if p<0.05; S: significant; NS: not significant
Friedman test. Statistically significant if p<0.05