Most patients regard tooth loss as mutilation. The edentulous state represents a compromise in the integrity of masticatory system and aesthetics. The treatment of edentulous patient presents a range of biomechanical problems that involve individual tolerance and perceptions. The establishment of vertical maxillo-mandibular relationship is a phase of prosthodontic treatment for edentulous patients in which it is difficult to arrive at definite conclusion from a practical viewpoint [1]. There are many aids that have been utilized in determining vertical dimension of occlusion [2,3].
The vertical dimension of occlusion is the distance measured between two points when the occluding members are in contact. Many methods have been proposed for determining the correct vertical dimension of occlusion, which include the use of interocclusal distance, swallowing threshold, patient’s judgment, maximum biting force, closest speaking space, cephalometric radiographs, certain anatomic landmarks and lip length [4]. Unfortunately, there is not a single universally accepted or completely accurate method. Therefore, many authors have recommended the use of pre-extraction records for determining the vertical dimension of occlusion of the edentulous patient [5–7].
The aim of the study is to find whether the measurement between the distance between the anterior attachment of the lingual frenum and the incisal edge of the mandibular central incisor on casts as a pre-extraction record is reliable. This is important for the purpose of establishing the mandibular occlusal plane as well as to determine the vertical position of the mandibular incisors in the complete denture patients.
The objective of this study is to give a range of numerical values from anterior attachment of lingual frenum to mandibular central incisors in a class I ridge relation in south Indian population which should aid in establishing the vertical dimension of the edentulous patient and also to locate the mandibular incisors in teeth arrangement of complete denture fabrication.
Materials and Methods
The study was carried out in Department of Prosthodontics, Rajah Muthiah Dental college and Hospital, Annamalai University, India. Prior to starting of the study the research proposal was put forward to ethical committee of the instituition and approval was obtained. The procedures in the study were in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975 that was revised in 2000.
Inclusion criteria
A total of 100 subjects comprising of 50 males and 50 females, aged between the age 21-28 y, with class I dental relationship were selected. Subjects with prosthesis, attrition, ankyloglossia, supra erupted and mobile teeth, and persons who have undergone orthodontic treatment were excluded in the study.
Subjects in this study were between 21-28 y was due to the fact that average of 23 y is considered to be a complete dentition. The total duration of the study was one year and six months.
Two mandibular casts were made for each subject to avoid error caused by single cast and also to obtain an average value for each patient. The casts were made from irreversible hydrocolloid impression material (Algitex, Dental products of India, Mumbai, India) using perforated metal stock trays. Trays were adjusted so that the lingual edges of the trays were approximately 2 to 3 mm short of the movable tissues of the floor of the mouth. All subjects were instructed to elevate the tongue and moisten the upper lip with the tip of the tongue, while the impressions were made [Table/Fig-1,2,3]. During impression fabrication, impression trays were held in place by placing the index fingers in first molar and second premolar regions bilaterally, to prevent movement of the trays. The impression material was mixed according to the manufacturer’s instructions. All impressions were poured in Dental stone type III (Goldstone, Asian chemicals, Rajkot, India).
Tongue in elevated position touching central part of upper lip

Tongue in elevated position touching right lateral part of upper lip

Tongue in elevated position touching left part of upper lip

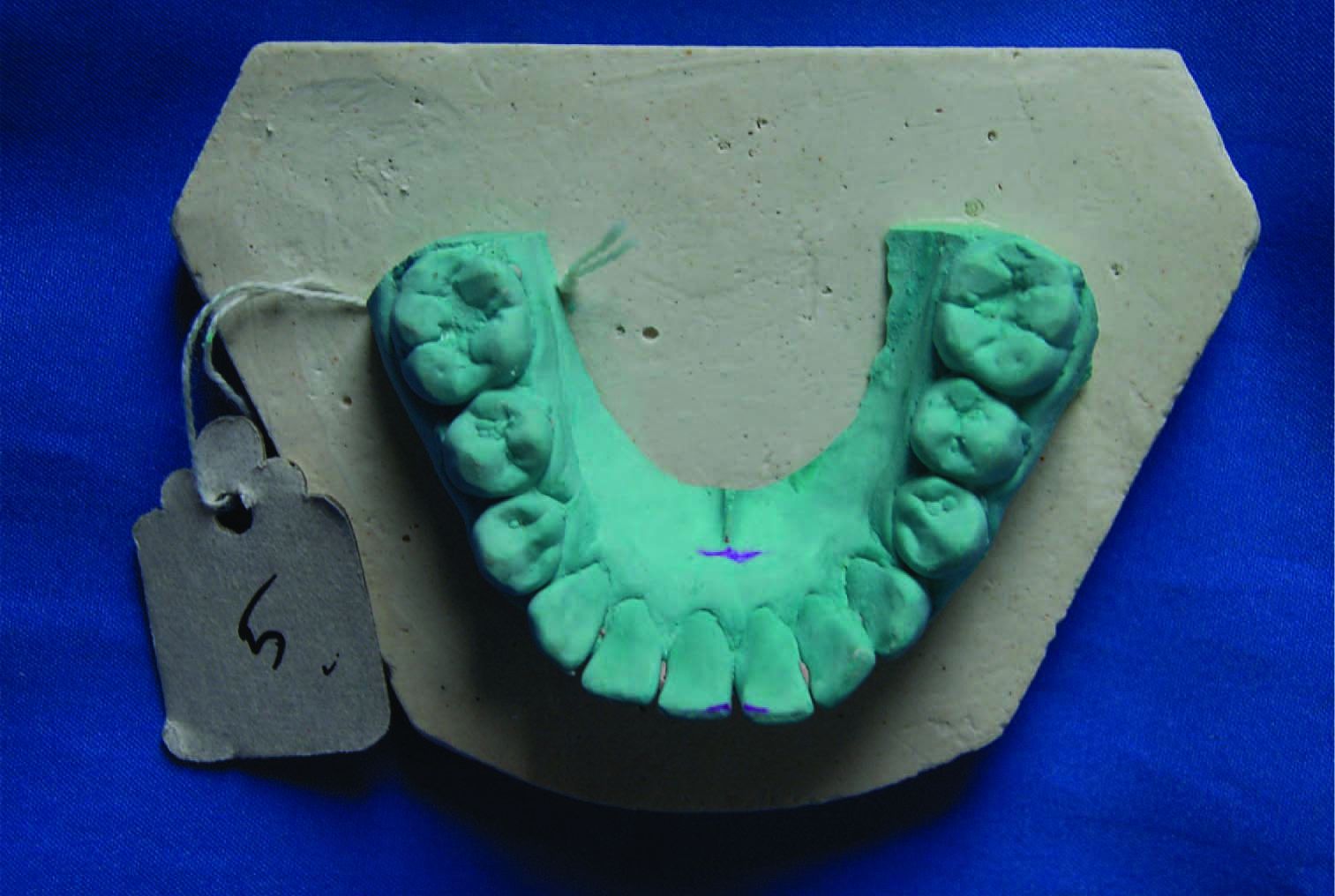
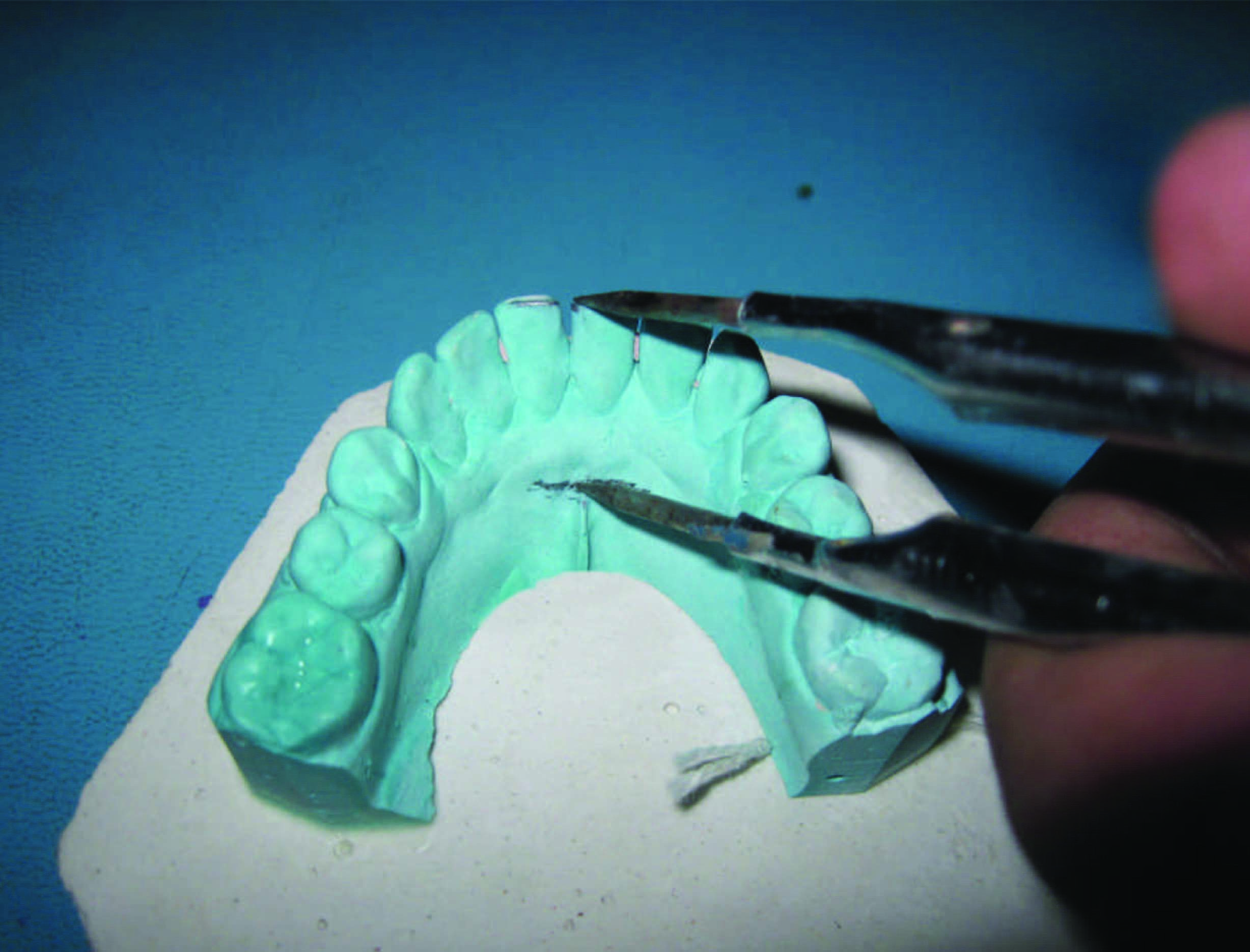
Casts were poured using Two pour technique, and all the casts were trimmed distal to the second molars. The cast was uniformly attached to plaster base made with a same rubber mould [Table/Fig-4]. All the models were marked with an indexing label in which white & green tag denotes the male and female models. In each subject the first model was denoted as X and the second model denoted by X°. The vertical distance between the anterior attachment of the lingual frenum and incisal edges of the mandibular incisors were measured on the casts for each subject. Two pencil marks were placed on the mandibular casts; a lower mark was placed on the frena, in the midline located in the sublingual sulcus. An upper mark was placed on an incisal edge of a right or left mandibular central incisor [Table/Fig-5]. These pencil marks were placed at the same position on the 2 casts of each subject. For uniform measurement in all subjects the upper mark was measured from the mesial edge of the 4th quadrant central incisor. The distance between the two horizontal marks was measured by divider [Table/Fig-6].

Upper and lower markings placed on the cast
Distance between upper and lower mark measured by a divider
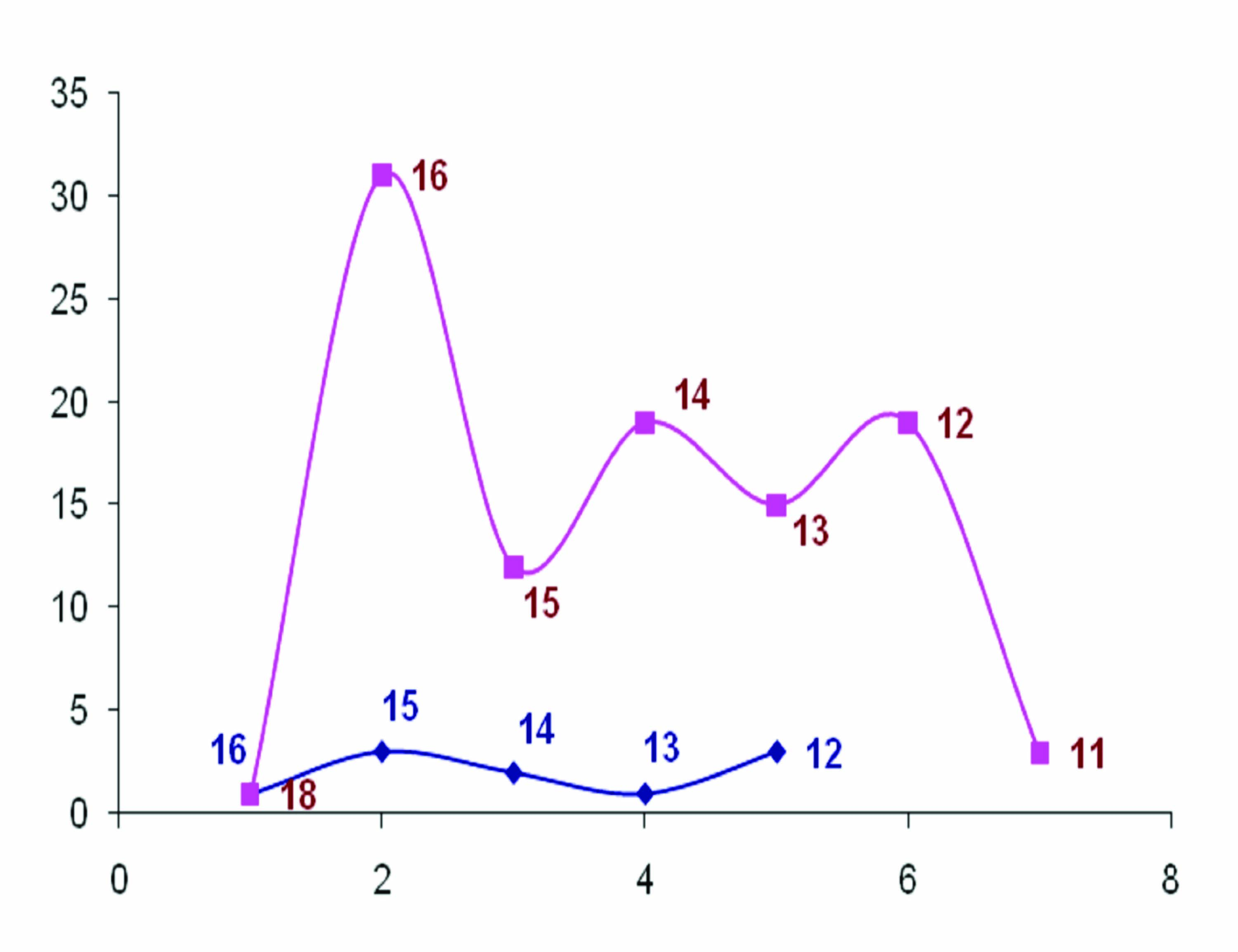
The divider mark is transferred to white sheet using carbon paper [3Table/Fig-7]. The value from the carbon mark is obtained using a digital vernier caliper (Mitutoyo vernier calipers, Japan) [Table/Fig-8]. The first model readings were measured by one clinician and the second model of all subjects were measured by another clinician to avoid observer error. The mean and the standard deviation (SD) of the two measurements for all subjects were calculated and statistically analysed. The values were denoted in a chart [Table/Fig-9] that shows the average readings lie between 12mm and 16mm.
Divider measurement transferred to a white sheet
Values of the measurements obtained via digital vernier caliper

Chart showing main study (indicated by pink) and pilot study (indicated by blue)
Result
The measurements, of all the subjects are presented in [Table/Fig-10]. Mean and Standard deviation were obtained using descriptive statistics tool by means of SPSS software version 18.
Measurements of MODEL 1 and 2 of the patients
| Patient no. | Model 1 (in mm) | Model 2 (in mm) | Patient no. | MODEL 1 (in mm) | Model 2 (in mm) | Patient no. | Model 1 (in mm) | Model 2 (in mm) | Patient no. | Model 1 (in mm) | Model 2 (in mm) |
|---|
| 1 | 16.13 | 16.11 | 26 | 16.67 | 16.34 | 51 | 16.52 | 16.29 | 76 | 11.15 | 11.77 |
| 2 | 16.88 | 16.79 | 27 | 14.00 | 14.50 | 52 | 14.05 | 14.40 | 77 | 12.24 | 12.51 |
| 3 | 15.75 | 16.38 | 28 | 15.65 | 15.97 | 53 | 16.40 | 16.78 | 78 | 16.32 | 16.19 |
| 4 | 18.19 | 18.21 | 29 | 12.64 | 12.34 | 54 | 14.20 | 14.63 | 79 | 14.80 | 14.80 |
| 5 | 16.09 | 16.34 | 30 | 14.81 | 14.79 | 55 | 16.50 | 16.35 | 80 | 13.19 | 13.43 |
| 6 | 12.67 | 12.64 | 31 | 12.59 | 12.27 | 56 | 14.26 | 14.69 | 81 | 15.39 | 15.63 |
| 7 | 12.53 | 12.84 | 32 | 16.32 | 16.19 | 57 | 13.82 | 13.55 | 82 | 16.11 | 16.00 |
| 8 | 16.72 | 16.81 | 33 | 14.80 | 14.80 | 58 | 15.67 | 15.34 | 83 | 16.94 | 16.53 |
| 9 | 16.97 | 16.94 | 34 | 11.19 | 11.43 | 59 | 14.00 | 14.30 | 84 | 13.33 | 13.30 |
| 10 | 12.36 | 11.81 | 35 | 15.39 | 15.63 | 60 | 12.65 | 12.97 | 85 | 14.13 | 14.28 |
| 11 | 16.86 | 16.42 | 36 | 13.11 | 13.00 | 61 | 12.44 | 12.74 | 86 | 16.65 | 16.97 |
| 12 | 15.46 | 15.20 | 37 | 16.94 | 16.53 | 62 | 15.72 | 15.81 | 87 | 12.64 | 12.34 |
| 13 | 12.44 | 11.61 | 38 | 16.33 | 16.30 | 63 | 16.97 | 16.94 | 88 | 16.72 | 16.81 |
| 14 | 14.50 | 14.00 | 39 | 14.13 | 14.28 | 64 | 12.36 | 12.61 | 89 | 14.97 | 14.94 |
| 15 | 16.94 | 16.67 | 40 | 13.99 | 14.11 | 65 | 14.86 | 14.42 | 90 | 11.36 | 11.61 |
| 16 | 12.20 | 12.25 | 41 | 15.98 | 15.66 | 66 | 16.46 | 16.20 | 91 | 16.86 | 16.82 |
| 17 | 16.15 | 15.90 | 42 | 13.66 | 13.36 | 67 | 12.44 | 12.61 | 92 | 12.62 | 12.29 |
| 18 | 15.90 | 15.65 | 43 | 16.63 | 16.49 | 68 | 15.50 | 15.00 | 93 | 13.05 | 13.70 |
| 19 | 16.62 | 16.29 | 44 | 13.58 | 13.49 | 69 | 13.94 | 13.67 | 94 | 12.40 | 12.28 |
| 20 | 14.05 | 13.70 | 45 | 13.15 | 13.77 | 70 | 12.20 | 12.25 | 95 | 15.20 | 15.13 |
| 21 | 16.40 | 16.28 | 46 | 12.24 | 12.51 | 71 | 14.99 | 14.71 | 96 | 16.50 | 16.35 |
| 22 | 14.20 | 13.13 | 47 | 16.32 | 16.03 | 72 | 15.98 | 15.66 | 97 | 14.26 | 14.59 |
| 23 | 16.50 | 16.35 | 48 | 14.66 | 14.29 | 73 | 13.66 | 13.36 | 98 | 13.82 | 13.05 |
| 24 | 14.26 | 13.89 | 49 | 16.48 | 16.17 | 74 | 12.63 | 12.49 | 99 | 16.67 | 16.34 |
| 25 | 13.82 | 13.05 | 50 | 14.91 | 14.73 | 75 | 13.58 | 13.49 | 100 | 12.00 | 12.50 |
Total =1450.16; Mean = μ=14.5016; n=100
Standard deviation= ∑X2/n-μ2 = 2.2245
The mean, Standard Deviation of the distance between the anterior attachment of the lingual frenum and incisal edges of mandibular central incisors among the 100 subjects was 2.2245 mm.
Mean ± S.D = (14.50 ± 2.2245)
After obtaining the results, the results were indeed applied to 10 complete denture patients. From this present study it was found that the location of mandibular occlusal plane, position of the mandibular central incisor and determination of vertical dimension of occlusion could be easily achieved with high degree of accuracy with very less chair side time consumption.
Discussion
Correct registration of the vertical dimension of occlusion is essential in the fabrication of complete dentures. Alteration of the vertical dimension of occlusion can affect aesthetics, speech difficulties, muscle discomfort and temporo mandibular joint problems. Centric jaw relation record is of utmost importance in recording vertical dimension as it a three dimensional record and boos bimeter is an accurate instrument to record vertical dimension [11]. But it is time consuming and requires special equipment. Open rest position of lips together with the corner of the lips (commissures) is also an important method in determining posterior occlusal plane [12]. This technique is easier but subjective variations are very common with this technique and hence not a reliable method.
Other techniques which are reliable methods of recording pre extraction vertical dimension at occlusion include Chin–nose measurement and Sorensen profile scale. Chin-nose method has an advantage that it is convenient, cost effective and easy method of recording vertical dimension and more importantly it is accurate as measurements are made from immovable tissues [13]. Other methods used in recording vertical dimension is as follows Dakometer, Turner’s cut out technique, Swenson’s clear resin mask , measurement of closing forces technique, tactile sensation, facial dimension, phonetics, deglutition and physiological rest position. Aesthetic appearance is a very crucial guide in establishing vertical dimension when no pre-extraction records are available [14,15].
Profile tracings by means of lead wires were also used as pre extraction record for determining vertical dimension [16]. Many authors confer that the only way to precisely record the vertical dimension of occlusion of an edentulous patient would be with the record obtained before extraction [16]. The use of distance between the anterior attachment of the lingual frenum and the incisal edges of the mandibular central incisor is one of the pre extraction records which could be used while constructing complete dentures [6,10,17,18].
The present study had been previously conducted in 3 different ethnical groups. The results of those three studies are as follows:
Bissasu [10] found that the mean measurements of the distance between the anterior attachment of the lingual frenum and the incisal edges of the mandibular central incisor were 10.26 mm in Syrian population (nine males and nine females). He also noted that this measurement could be used for locating the position of the central incisor and also to locate vertical dimension at occlusion
Rahman et al., [17] have determined the mean value of distance between the anterior attachment of the lingual frenum and the incisal edges of the mandibular central incisor was 10.7 mm in males and 10.9 mm in females in Iraqi population (15 males and 15 females). They have concluded that because the position of the incisal edges of mandibular incisors was stable, the position of the anterior attachment of the lingual frenum could be considered relatively stable when the frenum was recoded during function.
According to Parimala and Prithviraj [18] in a group of 100 dentulous subjects in Bangalore city, India, the mean vertical distance between anterosuperior most point on the lingual frenum and mesioincisal edges of mandibular central incisors was 12.3 mm. they have recommended that this average vertical distance of 12.3 mm can be used to establish the level of lower occlusal plane and vertical positioning of mandibular anterior teeth in complete denture patients if no other pre-extraction records are available.
The results of the present study strongly correlates with previous studies of Bissasu [6,14], Rahman [17], Parimala BK and Prithviraj DR [18]. The results of this study revealed that the mean SD of the distance between anterior attachment of the lingual frenum and the incisal edges of the mandibular central incisors among the 100 subjects was 14.50 ± 2.2245 mm. The sample size is sufficient enough to arrive at a statistically significant result when compared to previous studies.
The results of this study indicate that the distance between the anterior attachment of the lingual frenum and the incisal edges of mandibular central incisors was reliable when the frenum was recorded during function. Because, the position of the incisal edges of mandibular incisor was stable, the position of the anterior attachment of the lingual frenum can be considered relatively stable when the frenum was recorded during function.
The results from this study was verified with 10 complete denture patients and the value measured between anterior attachment of the lingual frenum and mandibular incisal edge ranges between 12-16mm. Moreover, it was found that those dentures which had higher or lower values of the distance between anterior attachment of the lingual frenum and mandibular incisal edge (i.e., less than 12 mm or greater than 16 mm) showed compromised aesthetics as well as function.
Conclusion
The two inferences of this study for a Class I ridge relation complete denture patient was:
The numerical value 14±2mm can aid in fabricating of mandibular occlusal rim to the maximum value, i.e., 16 mm, or to minimum of 12 mm thereby reducing the chair side time while establishing the vertical dimension.
The complete denture can be fabricated more appreciable by arranging the mandibular anterior teeth in 12 to 16mm from the anterior attachment of the lingual frenum.
Also, further study is needed to find out the reliability for other population and Class II & III ridge relations.