Microleakage Evaluation Around Retrograde Filling Materials Prepared Using Conventional and Ultrasonic Techniques
Pragna Mandava1, Nagesh Bolla2, Jayaprakash Thumu3, Sayesh Vemuri4, Sunil Chukka5
1 Senior Lecturer, Department of Conservative Dentistry and Endodontics, SIBAR Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
2 Professor and HOD, Department of Conservative Dentistry and Endodontics, SIBAR Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
3 Professor and HOD, Department of Conservative Dentistry and Endodontics, St. Joseph Dental College, Eluru, Andhra Pradesh, India.
4 Professor, Department of Conservative Dentistry and Endodontics, SIBAR Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
5 Professor, Department of Conservative Dentistry and Endodontics, SIBAR Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pragna Mandava, Senior Lecturer, Department of Conservative Dentistry and Endodontics, SIBAR Institute of Dental Sciences, Guntur, Andhra Pradesh-533509, India.
E-mail:peggi.mandava@gmail.com
Introduction: The importance of the retrograde cavity preparation and the material used to restore is of utmost importance to achieve successful surgical endodontics.
Aim: The aim of the present study is to evaluate the apical micro-leakage of root end cavities filled with Mineral trioxide aggregate, Biodentine and light cure GIC using two different cavity preparation techniques that is conventional bur preparation and ultrasonic tip preparation.
Materials and Methods: Eighty extracted single rooted human teeth (except mandibular incisors) with one canal, fully developed apices and without any major carious lesion are collected for the study. The teeth were sectioned at CEJ to standardize the length. Roots are instrumented upto master apical file 40 K size and obturated with gutta percha and AH plus sealer in lateral condensation technique. The teeth were then resected apically at 90° angle axis to the long axis of the root removing 3 mm of the apex.
The teeth were divided in to four groups of 20 each-
• Group I- samples restored with MTA.
• Group II- samples restored with Biodentine.
• Group III- (Positive control group)- samples restored with Light activated GIC.
• Group IV - (negative control group)- no filling material.
Each group is divided into two subgroups (a, b) of ten teeth each
1. Retropreparation done with ultrasonic retrotip.
2. Retropreparation done with conventional bur.
The teeth were then immersed in 0.5% Rhodamine B dye for 48 h. The teeth were split longitudinally and the interface between the restored material and the canal wall is observed under Confocal laser scanning microscope. Depth of dye penetration was examined under stereomicroscope.
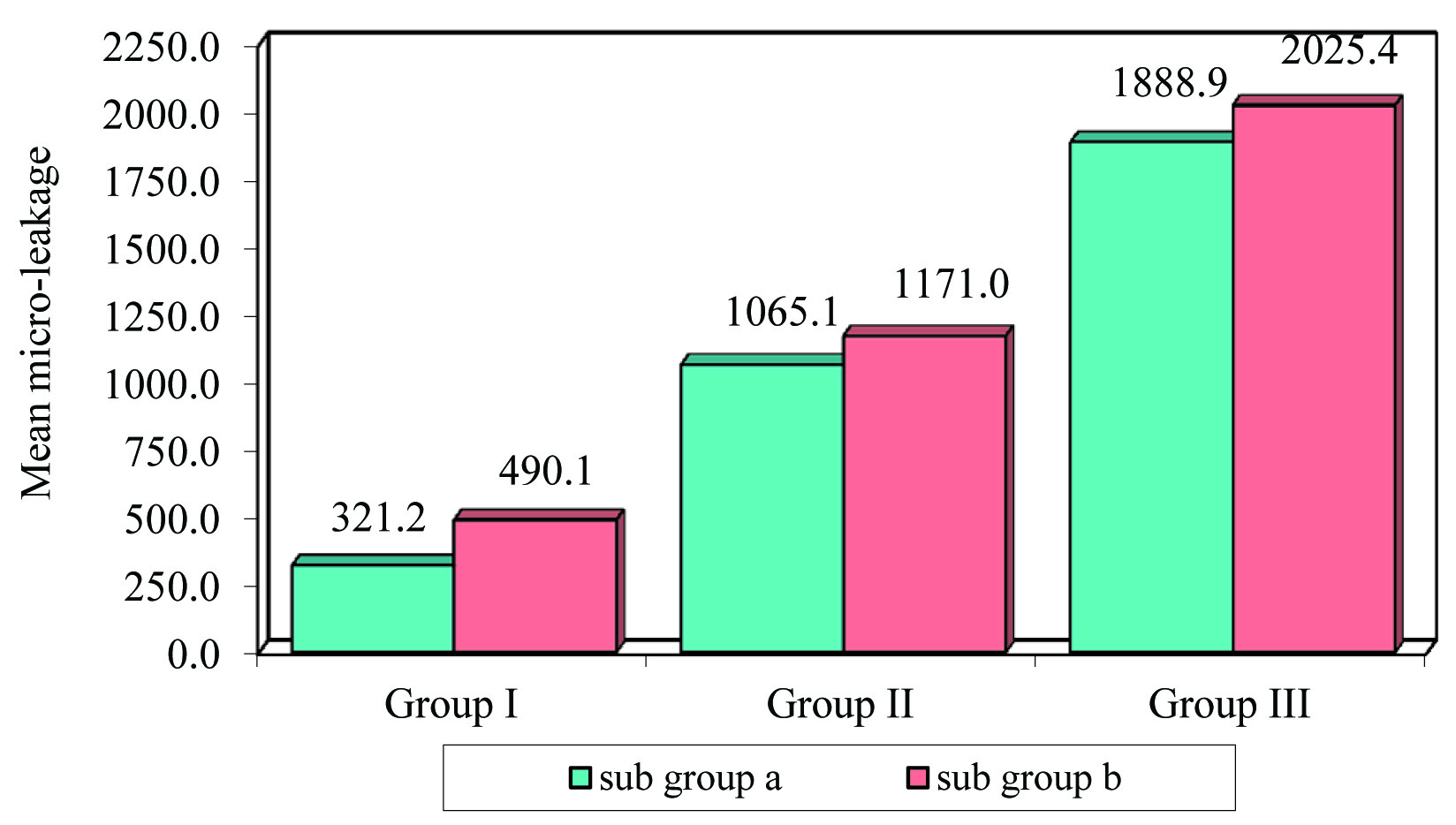
Results: The statistical analysis was performed by One way ANOVA, t test. Pair wise comparision was done by Newman – Keuls multiple post hoc test. The mean values of Dye penetration for Group Ia (321.23), Group Ib (490.11), Group IIa (1065.14), Group IIb (1170.96), Group IIIa (1888.90), Group IIIb (2025.35). The samples prepared with ultrasonic retrotip showed less microleakage but it is statistically not significant.
Conclusion: MTA showed significantly less microleakage when compared to Biodentine and light cure GIC and there is no statistical difference between the ultrasonic retrotip preparation and conventional bur preparation.
Biodentine, Endodontic surgery, MTA, Retrograde preparation, Ultrasonic
Introduction
The success of non surgical endodontics depends on thorough debridement, disinfection and complete obliteration of the root canal system by providing obturation that is fluid impervious [1]. In this context many new materials, techniques, concepts and instruments have developed to achieve the ultimate goal but in some cases the periapical pathosis remains unresolved [2].
In these cases where orthograde treatment seems unsuccessful or contraindicated surgical endodontics is resorted to save the tooth [3]. Endodontic surgery involves elevation of the flap, locating the root tip, root end resection, preparing the retrograde cavity and restoring it with biocompatible material which provides good seal at the apex [4]. Root end resection is indispensable in surgical endodontics. The root ends of the teeth could have variations in the root anatomy becoming source of treatment failure. All these considerations make it mandatory to eliminate the last apical three millimeters for maximum security [5].
The plane of sectioning the root is equally important consideration in technique of root resection. Inclined plane sectioning results in open dentinal tubules that may compromise healing of the lesion. 90o angulation has been proved to be most acceptable by earlier studies [6].
For making a cavity preparation in root end we can use various instruments like conventional slow speed handpieces, high speed Airotor handpiece with burs, sonics and ultrasonics. Although ultrasonic tips follow the root canal space better than conventional techniques but have shown to cause more rates of root fractures [7]. The depth of the pereparation ideally should be 3 mm as more than that does not bestow any greater benefits whereas lesser depth may jeopardize the long-term success of the apical seal [8].
Root end filling is the procedure by which an inert non-toxic material is packed into the root canal through an apical cavity [9,10]. An ideal root end filling material should adhere to the preparation walls forming a tight seal in root canal system. It should be non toxic, well tolerated by the periradicular tissues and promote healing, should be radiopaque, easy to manipulate, dimensionally stable, non absorbable and not be affected by presence of moisture. Numerous materials have been suggested for use as root end fillings. The root end filling materials can be broadly classified as adhesive materials and non adhesive materials [11].
Aim
The aim of the present study is to evaluate the apical microleakage of root end cavities filled with Mineral trioxide aggregate (MTA), Biodentine and light cure GIC using two different cavity preparation techniques that is conventional bur preparation and ultrasonic tip preparation.
Materials and Methods
Eighty freshly extracted human single rooted teeth except mandibular incisors with completely formed apices and straight canals were stored in normal saline until use. The teeth were cleaned ultra-sonically, and sectioned at CEJ using a diamond disc mounted on a micromotor handpiece before starting the root canal preparation. Preoperative radiographs were taken and access cavities were prepared using a high speed Endoaccess bur. The pulp tissue was extirpated with a barbed broach. 15 K-flex file was used to confirm canal patency. The working length was determined by visualizing the file at the apex.
Canals were prepared with step back technique using 3% sodium hypochlorite and 17% EDTA as irrigants. The canals were enlarged upto No. 40 K file at the apical foramen. The specimens were stored in normal saline until obturation. Canals were dried using absorbent paper points and master cone selection was confirmed with radiographs. Canals were obturated with gutta percha by lateral compaction technique using AH plus sealer. Radiographs were taken to confirm the quality of obturation and the access cavities were sealed with composite resin restorative material after 24 hour.
The teeth were then stored in saline for one week and then were resected apically at 90° angle axis to the long axis of the root using cross cut fissure bur removing 3 mm of the apex.
The teeth were divided in to four groups of 20 each
Group I- samples restored with MTA.
Group II- samples restored with Biodentine.
Group III- (Positive control group) - samples restored with Light activated GIC.
Group IV - (negative control group)- no filling material.
Each group is divided into two subgroups (a, b) of ten teeth each
Retropreparation done with ultrasonic retrotip.
Retropreparation done with conventional bur.
The ultrasonic tip used in root end preparation was P 14D (Satelac) in P5 Satelac unit at medium power setting as recommended by the manufacturer. A straight fissure diamond point in slow speed contra angle handpiece under saline irrigation was used for conventional retropreparation.
Specimens were stored in moist cotton and then were coated with three coats of nail varnish except at the apical 1 mm and then were allowed to dry. The specimens were suspended in 0.5% Rhodamine B dye for 48 h. Following this the roots were rinsed for 15 min under tap water. The teeth were split longitudinally with a diamond disc using a water coolant.
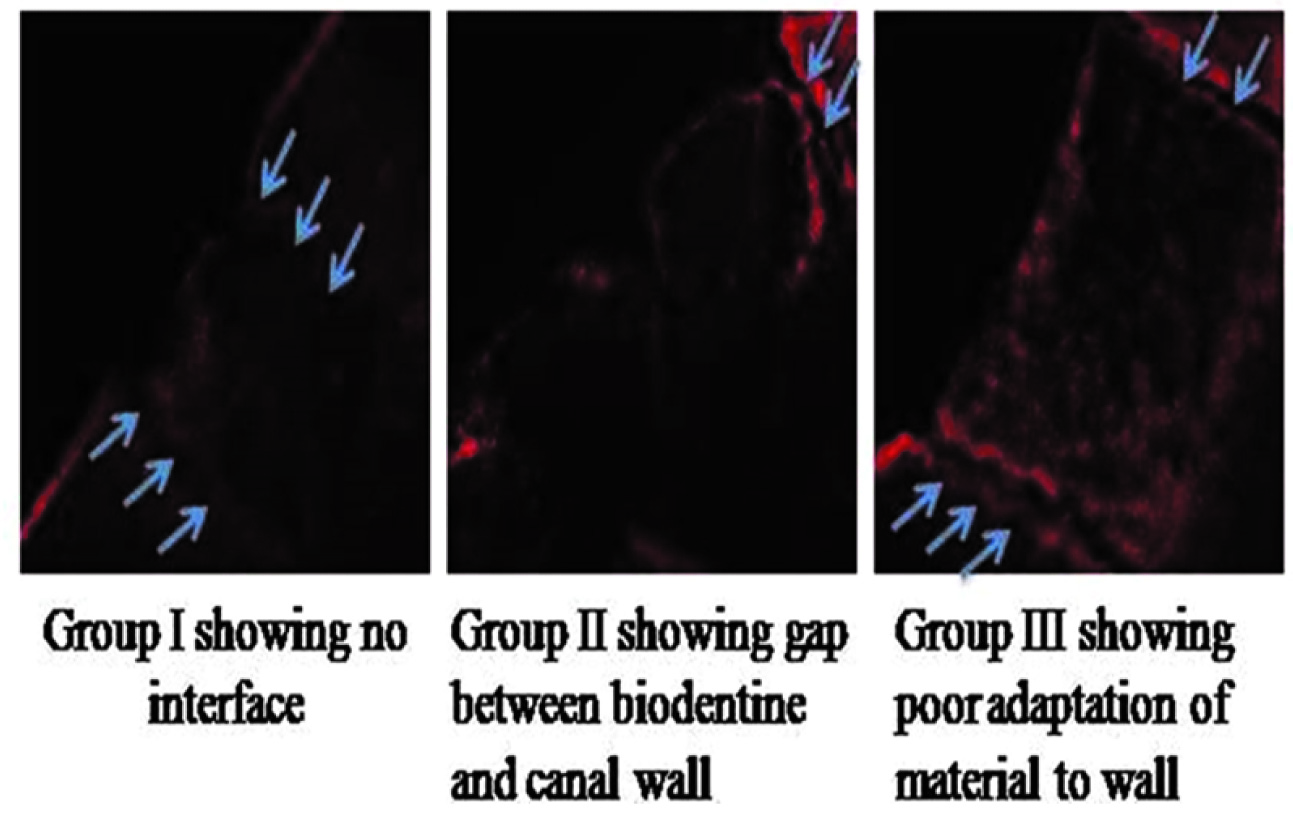
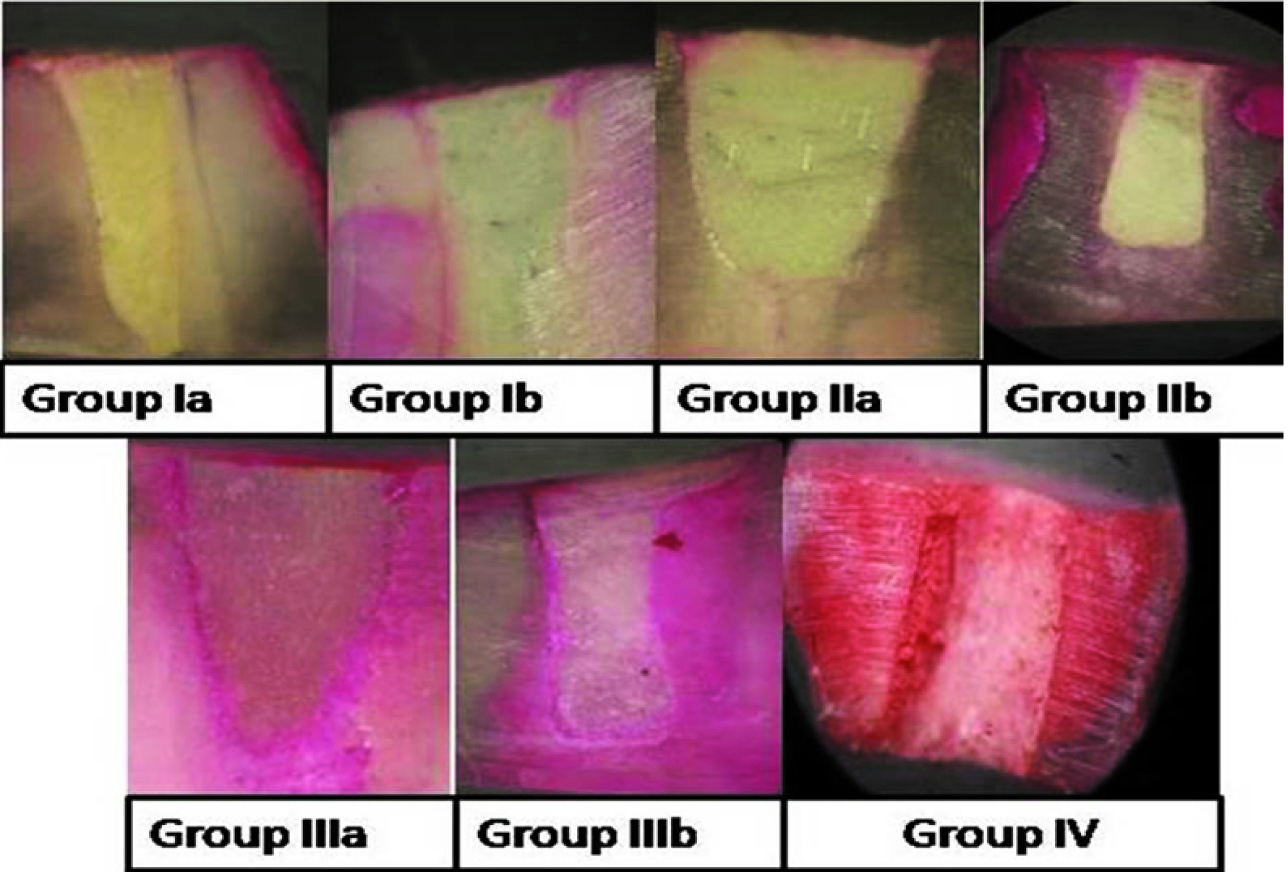
The interface between the restored material and the canal wall is observed under Confocal laser scanning microscope [Table/Fig-1]. Depth of dye penetration was examined under stereomicroscope and microleakage associated with different root end filling materials was evaluated in millimeters [Table/Fig-2].
Confocal images of the samples
The degree of dye penetration was identified according to ISO specification 1405:20037:
0 = no penetration;
1 = penetration to the enamel or cementum aspect of the preparation wall;
2 = penetration to the dentin aspect of the preparation wall, but not including the pulpal floor; and
3 = penetration including the pulpal floor of the preparation.
Results
The statistical analysis was performed by One-way ANOVA, t-test. Pair wise comparison was done by Newman – Keuls multiple post hoc test. [Table/Fig-3] shows the comparison of microleakage of all the three groups and their subgroups. The mean values of Dye penetration for Group Ia (321.23), Group Ib (490.11), Group IIa (1065.14), Group IIb (1170.96), Group IIIa (1888.90), Group IIIb (2025.35) [Table/Fig-1]. The overall comparison of the mean values of three groups and their subgroups indicate that within each group, though the microleakage values of ultrasonic prepared samples is less than conventional bur preparation, it is statistically not significant. But there was a statistically significant difference between MTA group and the remaining groups irrespective of the technique of retrograde preparation.
Comparison of sub groups a and b in main groups I, II, III with respect to micro-leakage
Discussion
Periradicular surgery includes surgical debridement of pathological periradicular tissue, root-end resection, preparation of a root-end cavity, and placement of a root-end filing to seal the root canal [12].
Plane of sectioning also affects the degree of microleakage so the root end resection angle of 90° was selected for this study. 90° angulation has been proved to be most acceptable by earlier studies [13]. The inclined plane sectioning at 30 or 45o angle could have disadvantages like open dentinal tubules, errors in post operative radiographs, more mechanical stresses, loss of dentin, cementum and bone that could result in compromised healing [14]. Apical ramifications and lateral canals are very common near the root tip. So, the Preferred depth of root resection is 3mm. Resection at the depth of 3 mm reduces the apical ramifications by 98% and lateral canals by 93% [14].
Carr has stated that, with the recent development of miniaturized ultrasonic tips, major shortcomings of rotary-type bur retropreparations appear to have been addressed. He also stated that the very small size of ultrasonic tips enables the surgeon to make conservative Class I cavity preparations down the long axis of the root and to extend the preparation buccolingually and through the isthmus without materially weakening the apical root structure. According to previous studies the ultrasonic root end preparation produced more conservative cavities when compared to conventional micromotor handpiece bur [15].
The ultrasonic retrotip has many advantages over the conventional bur preparation. The cavity with ultrasonic tip is along the long axis of the root thus causing minimal destruction to the morphology of the canal. The cavities prepared are conservative and precise. Moreover the cutting bevel obtained is perpendicular to the long axis of the root thus having the advantage of decreased number of exposed dentinal tubules at the resected surface and so the microleakage is also minimized [16].
The Mineral Trioxide Aggregate (MTA) was developed by Torabinejad, et al., The composition of MTA is tricalcium silicate, tricalcium aluminate, tricalcium oxide, silicate oxide. The powder particles are hydrophilic and small. When they come in contact with the moisture the hydration reaction occurs that results in colloidal gel structure which solidifies in the mineralized tooth structure [17].
White ProRoot MTA which was used in the present study was introduced in 2002, the main characteristic of which was the near-elimination (<0.5 mass %) from the original formulation of iron, depleting the set MTA of aluminoferrite, which was responsible for the gray coloration. This colour was problematic in some circumstances where the cosmetic appearance of the treated tooth was affected adversely. For reasons which are not clear, the aluminum content was also much reduce, while the arsenic content was reduced, presumably on toxicity concerns.
The smaller particle size of White MTA means it has a greater specific surface area, which in turn causes an increase in the wetting volume, water-binding capacity and hydration rate. At the same water–powder ratio, White MTA will be thicker, which together with an increase in the cohesiveness, a better workability is expected in comparison with Gray MTA [18].
Biodentine is the third material considered in the study. It uses novel active biosilicate technology to ensure superior mechanical properties. It has got short setting time of around 12 min, which is achieved by the bigger particle size, addition of Calcium chloride to the liquid component and decreasing the overall liquid content.
In the present study, the microleakage of MTA was comparatively less than Biodentine and Light cure GIC. These results were in accordance with other studies in which MTA showed better marginal seal than other retrograde filling materials like amalgam, GIC, IRM, light cure GIC, Super EBA, etc. [4,8,12,14,17–20]. This may be because of the formation of the hydroxyapatite like crystals at the interface between material and canal wall due to which the material shows superior adhesion preventing the penetration of the dye and thus showed least microleakage [19]. Moreover, MTA is hydrophilic so it undergoes setting expansion when it is cured in moist environment and thus the presence of moisture in the surgical field doesnot affects its setting or the properties [20].
Though statistically not significant the cavities prepared with ultrasonic retrotips showed less leakage than that prepared with the conventional burs. This result is also in accordance to previous studies which showed that ultrasonic retrotips showed cleaner cavities and are free of smear layer, which may be responsible for good marginal fit and thus showed lesser microleakage. The cavities prepared with the conventional bur in slow speed handpiece result in formation of considerable amount of debris and smear layer when compared to the ultrasonic tips. These remnants are permeable to fluids and toxins thus preventing the intimate contact of the material to the cavity walls. This may be the reason of greater microleakage seen in cavities prepared with conventional bur in slow speed handpiece. It was also proposed that when using a material that does not achieve a hermetic seal, preparation of the cavity with diamond coated ultrasonic tips is indicated to improve the seal and marginal fit [21] .
Conclusion
Following conclusions were drawn from this study:
The statistical analysis shows that all materials showed microleakage but there is significantly less microleakage in MTA when compared to Biodentine and light cure GIC.
There is no statistical difference between the ultrasonic retrotip preparation and conventional bur preparation.
The above discussion on the basis of this study concludes that MTA with ultrasonic preparation is the better material as root end filling material to prevent microleakage.
[1]. Ozata F, Erdilek N, Tezel H, A comparative sealability study of different retrofilling materialsInt Endod J 1993 26(4):241-45. [Google Scholar]
[2]. Sousa CJ, Loyola AM, Versiani MA, Biffi JC, Oliveira RP, Pascon EA, A comparative histological evaluation of the biocompatibility of materials used in apical surgeryInt Endod J 2004 37(11):738-48. [Google Scholar]
[3]. Holt GM, Dumsha TC, Leakage of amalgam, composite, and super-EBA, compared with a new retrofill material: bone cementJ Endod 2000 26(1):29-31. [Google Scholar]
[4]. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR, Dye leakage of four root end filling materials: effect of blood contaminationJ Endod 1994 20(4):159-63. [Google Scholar]
[5]. Gagliani M, Taschieri S, Molinari R, Ultrasonic root-end preparation: influence of cutting angle on the apical sealJ Endod 1998 24(11):726-30. [Google Scholar]
[6]. Sauveur G, Boccara E, Colon P, Sobel M, Boucher Y, A photoelastimetric analysis of stress induced by root-end resectionJ Endod 1998 24(11):740-43. [Google Scholar]
[7]. Min MM, Brown CE Jr, Legan JJ, Kafrawy AH, In vitro evaluation of effects of ultrasonic root-end preparation on resected root surfacesJ Endod 1997 23(10):624-28. [Google Scholar]
[8]. Gilheany PA, Figdor D, Tyas MJ, Apical dentin permeability and microleakage associated with root end resection and retrograde fillingJ Endod 1994 20(1):22-26. [Google Scholar]
[9]. Gartner AH, Dorn SO, Advances in endodontic surgeryDent Clin North Am 1992 36(2):357-78. [Google Scholar]
[10]. Roux D, Domejean-Orliaguet S, Saade M, Leakage associated with intermediate restorative material and glass-ionomer cement retrograde fillings: a human and sheep teeth comparison with 2 different aging proceduresOral Surg Oral Med Oral Pathol Oral Radiol Endod 2002 93(1):81-87. [Google Scholar]
[11]. Ingle John I, Bakland Leif K, Endodontics 2002 5th edElsevierB. C. Decker [Google Scholar]
[12]. Gondim E, Zaia AA, Gomes BP, Ferraz CC, Teixeira FB, Souza-Filho FJ, Investigation of the marginal adaptation of root-end filling materials in root end cavities prepared with ultrasonic tipsInt Endod J 2003 36(7):491-99. [Google Scholar]
[13]. Tidmarsh BG, Smith MG Arroow, Dentinal tubules at the root ends of apieected teeth: a scanning electron microscopic studyInternational Endodontic Journal 1989 22:184-89. [Google Scholar]
[14]. Kokate Sharad R, Pawar Ajinkya M, An in vitro comparative stereomicroscopic evaluation of marginal seal between MTA, glass inomer cement & biodentine as root end filling materials using 1% methylene blue as tracerEndodontology [Google Scholar]
[15]. Lin CP, Chou HG, Kuo JC, Lan WH, The quality of ultrasonic root-end preparation: a quantitative studyJ Endod 1998 24(10):666-70. [Google Scholar]
[16]. Bernardes RA, Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR, Evaluation of Apical Cavity Preparation With a New Type of Ultrasonic Diamond TipJ Endod 2007 33:484-87. [Google Scholar]
[17]. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR, Physical and chemical properties of a new root-end filling materialJ Endod 1995 21(7):349-53. [Google Scholar]
[18]. Darvell BW, Wu RC, “MTA”—An Hydraulic Silicate Cement: Review update and setting reactionDental materials 2011 27:407-22. [Google Scholar]
[19]. Gerhards F, Wagner W, Sealing ability of five different retrograde filling materialsJ Endod 1996 22(9):463-66. [Google Scholar]
[20]. Aqrabawi J, Sealing ability of amalgam, super EBA cement, and MTA when used as retrograde filling materialsBritish Dental Journal 2000 188:266-68. [Google Scholar]
[21]. Juan-Ignacio Rosales-Leal, Victoria Olmedo-Gaya, Manuel Vallecillo-Capilla, Juan-de-Dios Luna-del Castillo, Influence of cavity preparation technique (rotary vs. ultrasonic) on microleakage and marginal fit of six end-root filling materialsMed Oral Patol Oral Cir Bucal 2011 16(2):e185-89. [Google Scholar]