Leptospirosis is a worldwide zoonosis caused by spirochetes of the genus Leptospira [1,2]. The disease is endemic in some tropical and subtropical region and exposure to infection is widespread [3]. Leptospirosis is characterised by wide clinical variability, ranging from a mild flu-like illness to an acute life threatening condition, but only patients with the symptomatic forms of the disease are hospitalised [4]. Leptospirosis is a common cause of acute febrile illness in tropical climate and must be differentiated from other infection like typhoid, malaria, dengue, scrub typhus, viral hepatitis etc [5].
Early diagnosis of Leptospirosis is important since mortality rate is high in patient with severe Leptospirosis [5]. Diagnosis of Leptospirosis is often made by serological tests. The MAT is the serological test used in reference laboratories because of its high degree of sensitivity and specificity [2]. However, MAT is a complex test that requires significant expertise and large panel of live-cell suspensions, as well as, antibody levels detectable by MAT usually appear after day 6 or 7 of symptoms. Hence, interpretation of the results is difficult and results are usually not available quickly enough for patient management [2,5].
The early diagnosis of Leptospirosis is now possible by using different serological methods which are available commercially in the market such as an IgM ELISA, an IgM dipstick assay (LDS), latex agglutination test, lepto lateral flow test and the indirect hemagglutination assay (IHA) [2,6]. Therefore, rapid and easy to perform tests have emerged in recent years for the diagnosis of Leptospirosis. Majority of these rapid tests are immunochromatographic or particle agglutination tests. The introduction of such tests in the market needs their evaluation by comparing their results with the gold standard MAT or other tests like IgM ELISA [7]. Aim of the present study was to evaluate the usefulness of the diagnostic test kits (leptocheck WB, Latex agglutination test and SD leptospira) for the diagnosis of Leptospirosis by comparing their results with the ‘gold standard’ test, MAT and IgM ELISA.
Materials and Methods
Patients and sera: Serum specimens from 100 patients enrolled randomly in the study, conducted from July 2011 to October 2011. All the patients with acute Leptospirosis admitted in New Civil Hospital, Surat, Gujarat were included in this 4-months pilot study. Clinical suspicion of acute Leptospirosis was defined as fever and/or myalgia, tender liver, jaundice, acute renal failure, bleeding tendency, meningism and radiological lung infiltrates which accounted in the first week of fever. The study was approved by ethical committee of the institute. All the serum samples were tested for three commercially available rapid kits; Leptocheck WB, Latex agglutination test and SD leptospira. All the results were compared with IgM ELISA and MAT for confirmation of diagnosis.
MAT test: The MAT test was performed using standard procedure [8]. Serogroups included in the antigen panel were: L.Australis (Australis), L.Autumnalis (Bangkinang), L.Ballum (Ballum), L.Sejroe (Hardjo), L.Grippotyphosa (Grippotyphosa), L.Canicola (Canicola), L.Hebdomadis (Hebdomadis), L.Pomona (Pomona), L.Semeranga (Patoc1), L.Pyrogen (Pyrogen), L.Icterohaemorrhagiae (Icterohaemorrhagiae). All the strain were obtained from National Leptospirosis Reference Centre, RMRC, WHO collaborating centre, ICMR, Portblair. These serovars were maintained in semisolid 0.1% EMJH (Ellinghausen-McCullough-Johnson-Harris) agar by using Leptospira medium base supplemented with 10% enrichment (Difco,USA) at 28-30°C. Doubling dilution of serum in 96 well flat bottomed microtitre plates from 1 in 25 to 1 in 1600 was prepared by using phosphate buffer saline suspension as diluents. 50 μl of the specific serovar (Mc Farland 1.0) added to all wells. One of the wells with antigen only, without addition of antibody served as the antigen control. The final dilution after adding the antigen was 1 in 50 to 1 in 3200.The plate was covered with aluminium foil and incubated at 370C for 2 h in wet chamber or humid chamber to avoid dehydration. After 2 h of incubation, slide was examined by dark field microscopy at a magnification of 40X. The highest serum dilution showing approximately 50% agglutinated leptospires or reduction in the number of leptospiral cells as compared to the antigen control was taken as end point titer. MAT test is considered positive at titre of >100 for single serum samples [8,9].
Pan bio LeptospiraIgM ELISA test: Whole procedure was performed according to manufacturer’s instruction. Test sera and controls were diluted in 1:100 in serum diluents and 100 μl added into Leptospira (serovar patoc) antigen coated microwell. Then plate was incubated for 30 min at 37°C. After washing the plate with phosphate- buffered saline solution, 100 μl of HRP-conjugated anti-human IgM added and incubated for further 30 min at 37°C. Again washing the plate with buffered solution, 100 μl of the TMB (tetramethylbenzidine) substrate was added and incubated for 10 min at room temperature. Then reaction was stopped with 100 μl of 1M phosphoric acid. The absorbance value of each well was read at 450 nm wave length and reading was interpreted in terms of Pan-Bio units which in turn were calculated by the absorbance of positive control serum, negative control serum and cut-off of calibrators provided by the manufacturer. Pan Bio unit ≥11 was considered positive [2].
Rapid Leptocheck Test (Lot no.: 51080): Case and control sera (10μL) were used and tested according to the manufacturer’s instruction. It utilizes the principle of immunochromatography, a unique two-site immunoassay on a membrane. As the test sample flow through the membrane of the test device, the anti-human IgM colloidal gold conjugate forms a complex with IgM antibodies in the sample. This complex moves further on the membrane to the test window ‘T’ where it is immobilized by the broadly reactive leptospira genus specific antigen coated on the membrane, leading to the formation of a red to deep purple coloured band at the test region. ‘T’ which confirms a positive test result. If there is no band at the test region, it indicates negative result. At the ‘C’ window, the anti-rabbit antibodies is coated and the unreacted conjugate and the unbound complex if any move further on the membrane and are subsequently immobilized here and forming a red to deep purple coloured band. If there is no control band, it suggests the test is invalid [10].
Leptorapide (Latex agglutination test- Lot no. 230511-01): Whole test was performed according to the manufacturer’s instruction. 5 μl of Leptorapide reagent was added by dispensing pipette on the agglutination card. Then add 5 μl of test sera with new dispensing pipette to the 5 μl Leptorapide reagent and mix. Agglutination card was rotated gently for 2-3 min and a result was interpreted by using score card. A positive/negative result will appear within 3 min of mixing. Score extent of agglutination according to the scale [11].
SD LeptospiraIgM/IgG (Lot no. 99004): Whole test was performed according to the manufacturer’s instruction. Allow all kit components and specimen to room temperature prior to testing. Test device was removed from foil pouch and placed it on a flat, dry surface. 5μl of serum or plasma specimen was added into the square sample well marked as “S”. Four drops of assay diluent was added to the assay diluent well which is round shaped. Test results were interpreted within 20 min [12].
Results
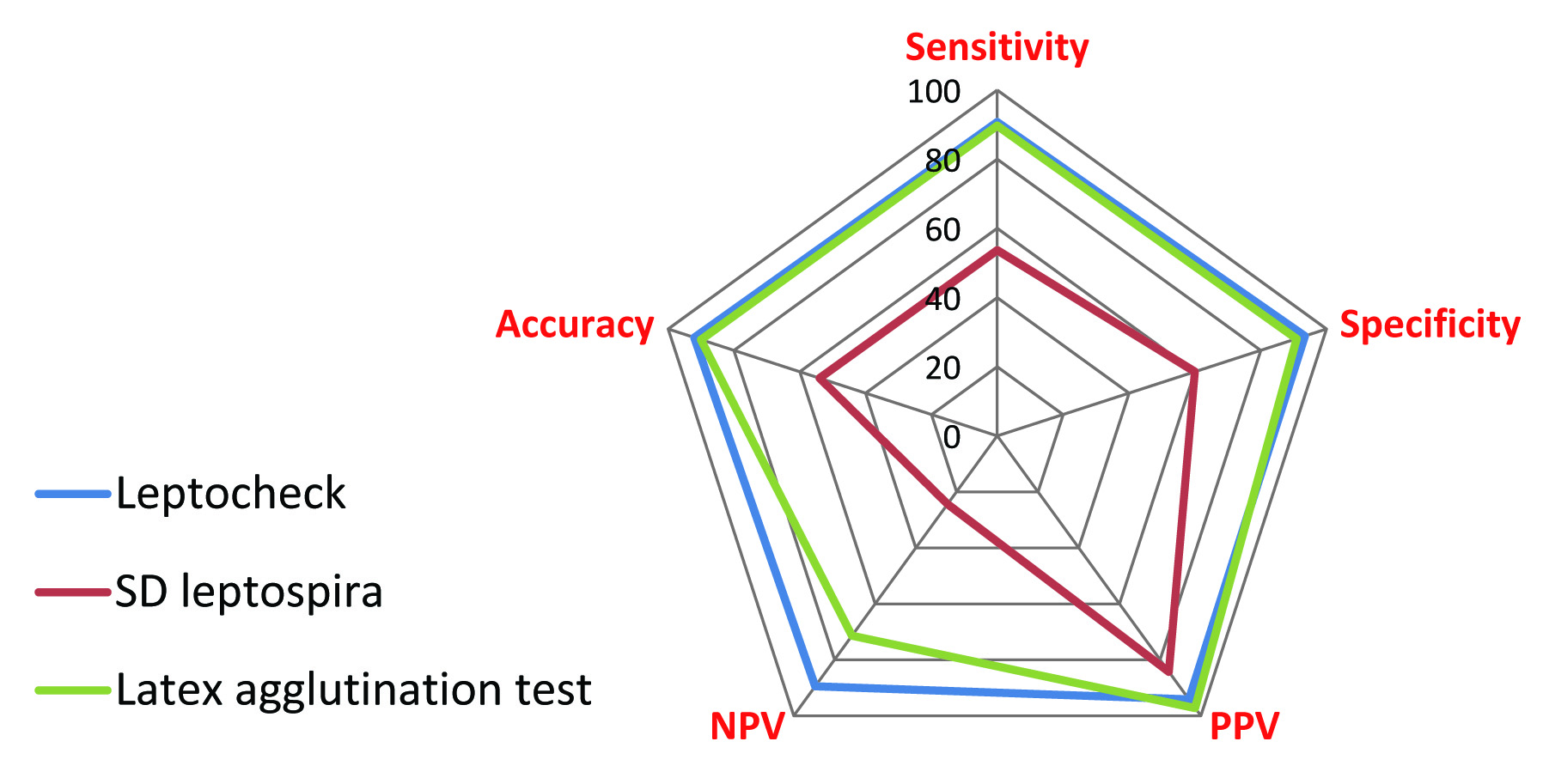
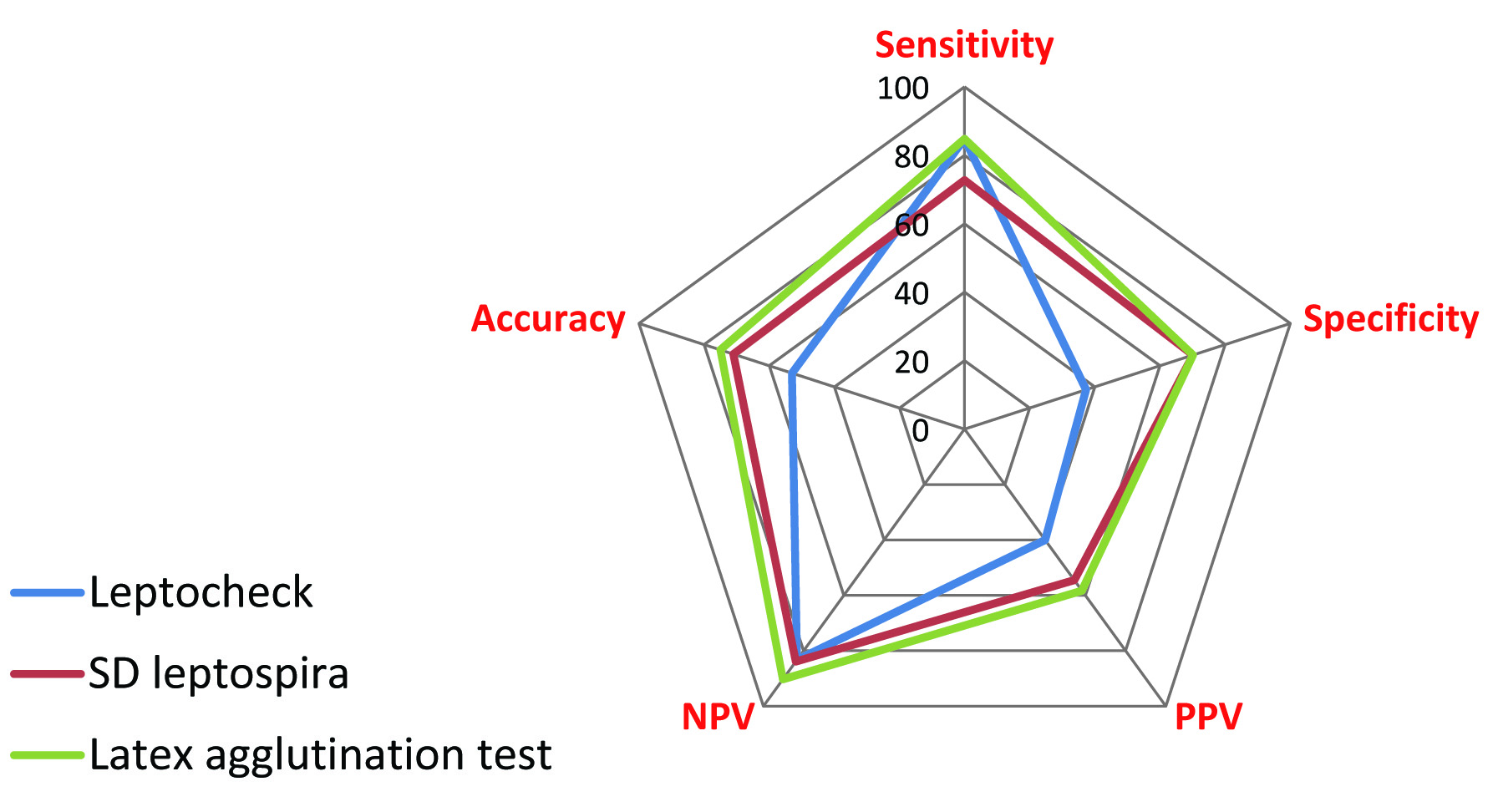
Total 100 samples were evaluated. 80 were IgM ELISA positive and 20 were IgM ELISA negative. 28 were MAT positive and 72 were MAT negative. All the samples were tested for three commercially available rapid kits Leptocheck WB, Latex agglutination test leptorapide and SD leptospira. Leptocheck WB has given 52 positives and 48 negative results; Latex agglutination test has given 72 positives and 28 negatives while SD leptospira rapid kit has given 51 positives and 49 negatives. Results of tests were compared considering ELISA and MAT as gold standard. Sensitivity, specificity, PPV, NPV and accuracy of three rapid tests were determined in comparison to IgM ELISA and MAT. Leptocheck WB, Latex agglutination test and SD leptospira had sensitivities of 84.8%, 84.8% and 72.7% & specificities of 37.3%, 70.1% and 70.1% respectively as compared to MAT. Leptocheck WB, Latex agglutination test and SD leptospira had sensitivities of 90.7%, 89.7% and 53.7% & specificities of 93.4%, 90.9% and 60% respectively as compared to IgM ELISA. Comparisons of results are shown in [Table/Fig-1,Table/Fig-2,3,4] for MAT & IgM ELISA respectively.
Comparison of different screening (Rapid) tests considering ELISA as Gold standard.
| Screening Test | %Sensitivity | %Specificity | %PPV | %NPV | %Accuracy |
|---|
| Leptocheck | 90.7 | 93.4 | 94.2 | 89.5 | 92 |
| Leptorapide | 89.7 | 90.9 | 97.2 | 71.4 | 90 |
| Sd Leptospira | 53.7 | 60 | 84.3 | 24.4 | 54 |
Comparison of different screening (Rapid) tests considering MAT as Gold standard.
| Screening Test | %Sensitivity | %Specificity | %PPV | %NPV | %Accuracy |
|---|
| Leptocheck | 84.8 | 37.3 | 40 | 83.3 | 53 |
| Leptorapide | 84.8 | 70.1 | 58.3 | 90.3 | 75 |
| Sd Leptospira | 72.7 | 70.1 | 54.5 | 83.9 | 71 |
Comparision of Rapid tests considering ELISA as Gold std
Comparision of Rapid tests considering MAT as Gold std
Discussion
As the disease Leptospirosis shows protean clinical manifestations, laboratory confirmation is a must. Isolation of leptospiras from clinical samples is time consuming; serology remains the mainstay of diagnosis [7]. MAT is not rapid test and it is used mainly in the reference laboratory only. In addition, its role in early diagnosis is rarely available. Various kits for rapid detection of Leptospirosis available commercially are simple, convenient, rapid and do not need complicated laboratory equipment. Moreover they do not require skilled hands and thus prove to be a suitable option for diagnosis in the peripheral regions. Though MAT and ELISA tests are widely used for confirmation of Leptospirosis, these commercially available rapid tests are also found to be effective. Thus their sensitivity and specificity needs to be evaluated by comparing them with ELISA and MAT results keeping them as references (gold standard) [4].
Rapid screening serological test which is sensitive early in the infection is needed. This is important because if treatment decisions are to be based on laboratory results, they must be made as early as possible, often without having available results from paired sera. When only samples from acutely ill patients were considered, the leptocheck WB and Latex agglutination test showed comparable sensitivity to the IgM-ELISA, whereas the sensitivity of the SD Leptospira IgM/IgG was closer to that of the MAT. Considering MAT as reference and compared with various rapid tests, SD leptospira shows higher sensitivity, specificity, PPV, NPV and accuracy values 72.7%, 70.1%, 54.5%, 83.9% and 71% respectively as both MAT and SD leptospira tests detects IgG antibodies appearing later during the course of disease. In S Shekatkar et al.,study showed the sensitivity and specificity of Latex agglutination test was 90.62% and 91.96% respectively compared to MAT (gold standard) which was slightly lower in our study that sensitivity and specificity of LAT was 84.8% and 70.1% respectively [13].
There are several possible explanations for the variability in screening test sensitivity observed between studies. The selection of the control population, which may cause difference [7]. The collection of healthy control sera was not done from endemic area, as cross reactivity also occurred in healthy controls, possibly as a result of preexisting condition. Lijmer et al., report that studies using a diseased population and a separate control group significantly overestimate the diagnostic performance of screening tests compared to studies using a single clinical population. The optimal design for assessing the accuracy of a diagnostic test is a prospective comparison of the “test and the reference test in a consecutive series of patients from a clinically relevant population [14]. Sensitivity of Leptospirosis screening tests may be affected by the prevalence of the various different infecting serogroups thereby effecting its performance. In all screening test for Leptospirosis diagnosis, antigen should be broadly reactive with different infecting Leptospira serovars. The characteristics of the Leptospiral antigen may differ from one place to another. So, the screening test should have ability to detect the antibodies produced against the site-specific leptospira serovars. Hence, laboratories need to validate the performance of screening tests in that particular setting in which they are to be used.
Sometimes, Leptospirosis patients might have co-infection or cross reactive antibodies of other diseases. Some of the control sera from other infectious etiology like syphilis, dengue, malaria, relapsing fever, lymes disease, legionellosis were not analyzed in this study as number of these disease agents have been reported by other investigators to cross react in leptospirosis serologic assay [3,5,15, 16]. In Stuart et al., study showed low sensitivity and specificity 47.3%, 75.5% of Leptotek IgM lateral flow test compared to gold standard MAT test [17], as MAT detects both IgM and IgG antibodies, it is difficult to differentiate between current clinical infection or past history of exposure to infection by doing only single MAT. At earlier stage of disease, genus specific IgM antibodies appear first so genus specific IgM immunoassay are expected to be positive than serovars specific MAT test. In this study, the specificity and sensitivity of latex-agglutination test (LAT) and Leptocheck WB showed comparable results to that genus specific IgM ELISA. LAT and Leptocheck WB have advantages of simple and rapid performance; and the use of stable antigens, which eliminates the necessity of maintaining live leptospiral cultures in diagnostic laboratories. The selection of a serodiagnostic assay is dependent on several factors, including the clinical likelihood of disease, the anticipated workload, and the availability of confirmatory testing in more specialized laboratories. Thus, in view of the reemerging zoonosis, the prompt diagnosis of Leptospirosis is essential for both patients care and efficient implementation of public health measures. It is therefore important to have an efficient diagnostic test that is rapid, accessible and practical to general physicians [18].
Conclusion
In this study, three rapid assays for early diagnosis of acute Leptospirosis in a hospital-based population were evaluated. Latex agglutination test kit and leptocheck WB were found to be highly sensitive and specific. Neither of these tests requires specialized equipment, and could be performed in peripheral laboratories with relatively little expertise. With either LA or leptocheck WB; human Leptospirosis will be diagnosed more readily and more accurately in the first week of fever for screening sera from acutely ill patients.