Unusual Foreign Body in a Routine Lateral Cephalogram
Shobha Sundareswaran1, Jean James2, Praveen S3, Latheef V.P4, Sreehari S4
1Professor and Head, Department of Orthodontics,Government Dental College, Calicut, Kerala, India.
2Junior Resident, Department of Orthodontics,Government Dental College, Calicut, Kerala, India.
3Associate Professor, Department of Orthodontics,Government Dental College, Calicut, Kerala, India.
4Associate Professor, Department of Orthodontics,Government Dental College, Calicut, Kerala, India.
5Associate Professor, Department of Orthodontics,Government Dental College, Calicut, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Shobha Sundareswaran, Professor and Head, Department of Orthodontics, Government Dental College, Calicut, Kerala - 673008, India.
E-mail: drshobhakumar@gmail.com
Routine radiographs made in the orthodontic office can often give way to detection and diagnosis of unusual syndromes, signs or foreign bodies. A case report of one such accidental detection of a very unusual foreign body within the nasal cavity of an orthodontic patient has been presented here to emphasize the importance of routine radiographic views, which over and above aiding in Orthodontic diagnosis, can also often detect potentially life threatening problems in the Oro-facial region.
Diagnostic cephalogram, Nasal foreign body
Case Report
A 12-year-old female patient reported to the Department of Orthodontics and Dentofacial Orthopedics with a presenting complaint of forwardly placed lower jaw. The patient was sent to the Department of Oral Radiology for a lateral cephalogram to facilitate orthodontic evaluation and diagnosis. The lateral cephalogram showed a radio-opacity in the maxillary sinus region [Table/Fig-1]. The patient was clinically examined thoroughly for presence of any radio-opaque objects in the craniofacial region which could account for the radiographic presentation. The radiograph was repeated to rule out any artefact.
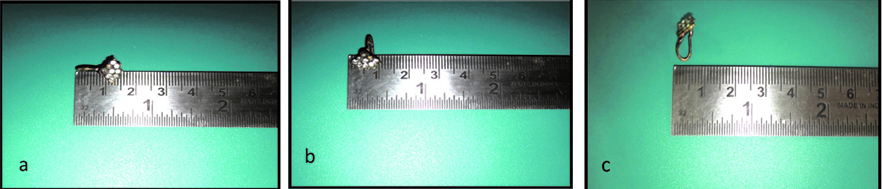
Initial history of the patient did not reveal anything of significance in this regard. On persistent probing and pointed questions regarding history of wearing jewellery of any sort in the region, the parent of the patient, reminisced about his child wearing a press-fit nose stud during a classical dance performance roughly 8 months earlier. He also agreed, upon our suggestion, to the possibility of having inhaled the piece of jewellery since the patient was suffering from a running nose at that time. Accordingly, the patient was queried regarding any signs or symptoms like pain, tenderness on palpation, nasal congestion, discharge and others to rule out maxillary sinusitis. However, the patient could not remember any untoward event at the time and had remained totally asymptomatic to date. A preliminary examination of the nasal cavity also did not reveal any apparent Cephalogramabnormalities. The patient was duly referred with a suspicion of nasal foreign body (NFB) to the ENT department for further evaluation. They confirmed our suspicions. Surgical intervention was done and a piece of nose jewellery was retrieved from the right nasal cavity. The piece of jewellery measured up to 15x10x5 mm in dimensions and was found to be partially corroded [Table/Fig-2a-c].
Discussion
Since the introduction of cephalometry by Broadbent in 1931, the applications of cephalometry have increased from merely being an aid for orthodontic diagnosis to detection of temporomandibular joint disorders, evaluation of tonsillar and lymphoid tissues, diagnosis of various craniofacial and related pathoses, and detection of foreign bodies and so on. It is of immense importance that the orthodontists understand their responsibility in thorough evaluation of all the diagnostic roentgenograms made by them. This responsibility lies not only in examining the facial patterns and the accuracy of tracings, but also in determining if other abnormalities are present. In this regard, routine radiographs made in the orthodontic office can often give way to detection and diagnosis of unusual syndromes, signs or foreign bodies [1,2].
There have been questions regarding the necessity of making routine radiographs in day to day practice due to concerns of unneccesarily exposing the patients to radiation hazards [3-8]. Here the risk of a minor radiation exposure should be weighed against the benefit of timely detection of potentially life threatening anomalies, especially those that remain asymptomatic for extended periods. There has been a continuous debate in literature on this issue. Guidelines for radiographs used in orthodontic diagnosis were put forth by the British Orthodontic Society [5], which were subsequently debated on and criticized [7]. Though studies on the radiation organ dosage from routine orthodontic care showed increased radiation burden in patients [4], lateral and PA (posterior-anterior) head films were found by Maillie HD et al., to deliver levels of radiation much lower than other standard dental radiographs and add very little to the patient’s carcinogenic burden [6]. In another such study by Freeman and Brand [3] the radiation exposure from a lateral cephalogram to the eye and the parotid and thyroid glands was found to be far less than from a panoramic and bitewing series.
In addition, there have been questions about orthodontists’ level of responsibility in discovering incidental abnormalities on radiographs [9]. As orthodontists, we cannot shy away from our responsibility in ensuring the overall health and general welfare of our patients. In today’s world of growing litigation, such responsibility has no longer remained a matter of choice but of absolute necessity. All orthodontists who take lateral cephalograms should approach each image as a skull film and observe the entire head and neck. Meticulous examination of lateral head films in a systematic and stepwise manner will prevent the clinician’s attention being diverted by certain specific areas or findings. Such a sequential examination has been prescribed by Bisk and Lee [2] which included inspection of the cranium, followed by the sella turcica and paranasal sinuses, nasal pharynx and cervical area. Paediatric radiologists are particularly interested in areas such as the mastoids, paranasal sinuses, sella turcica, nasopharynx including adenoid and tonsillar tissue, prevertebral area, soft palate, uvula, tongue, epiglottis, hyoid bone, vallecula, aryepiglottic fold, arytenoid, cervical spinal canal and spinal column and calvarium [2]. There have been numerous reports in literature on conditions found on routine lateral cephalometric orthodontic radiographs including cysts in the maxillary sinus, tuberculum sella, enlarged adenoids, maxillary sinusitis, as well as foreign bodies in the nostril and maxillary sinus areas to name a few [1,2].
Foreign bodies detected in the nasal cavity can be either inanimate or animate. They are found most commonly in the floor of the nose just below inferior turbinate or just anterior to the middle turbinate [10]. These nasal foreign bodies can lead to numerous complications such as infections of the maxillary sinuses, middle ear, epiglottis, the meninges, diphtheria, tetanus, rhinoliths and even erosion into adjacent structures [1].
Thus seemingly innocuous NFBs such as the nose jewellery detected in our case, can, if left undetected, consequently lead to an array of serious problems. If, on the contrary, they can be detected early enough, immediate interventions can be undertaken. Particularly in the case presented here, the patient had remained completely asymptomatic, which could have made the anomaly evade diagnosis for indefinite periods during which any of the above mentioned complications could have ensued. It was the timely detection from the routine lateral cephalograms that prevented such consequences.
Lateral cephalogram showing a radio-opacity in the maxillary sinus region

Lateral cephalogram showing a radio-opacity in the maxillary sinus region
Conclusion
In the case report presented, it was a matter of great intrigue that the patient remained completely oblivious of having inhaled and retained the object in her nasal cavity. She also remained surprisingly asymptomatic during the entire period. It was only because of the radiographic abnormality detected on routine pre orthodontic lateral cephalometric evaluation, a high degree of clinical suspicion and thorough clinical history that the presence of the foreign body was revealed. If retained indefinitely, this could possibly have given rise to a multitude of problems.
Thus, it can be safely stated that considering the risk benefit ratio, it is important to obtain radiographic images not only when need for those images is felt, but also as routine diagnostic procedure for each case. Hence this case emphasizes the importance of routine radiographic views, which over and above aiding in Orthodontic diagnosis, can also often detect potentially life threatening problems in the Oro-facial region.
[1]. AH Moffitt, Discovery of pathologies by orthodontists on lateral cephalogramsThe Angle orthodontist 2011 81(1):58-63. [Google Scholar]
[2]. S Bisk, FA Lee, Abnormalities found on cephalometric radiographsThe Angle orthodontist 1976 46(4):381-86. [Google Scholar]
[3]. JP Freeman, JW Brand, Radiation doses of commonly used dental radiographic surveysOral surgery, oral medicine, and oral pathology 1994 77(3):285-89. [Google Scholar]
[4]. P Hujoel, L Hollender, AM Bollen, JD Young, M McGee, A Grosso, Head-andneck organ doses from an episode of orthodontic careAmerican journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics 2008 133(2):210-17. [Google Scholar]
[5]. TA Isaacson, K Horner, E Whaites, Orthodontic Radiographic—Guidelines for the Use of Radiographs in Clinical Orthodontics 2008 3rd EditionBritish Orthodontic Society [Google Scholar]
[6]. HD Maillie, JE Gilda, Radiation-induced cancer risk in radiographic cephalometryOral Surgery, Oral Medicine and Oral Pathology 1993 75(5):631-37. [Google Scholar]
[7]. DL Turpin, British Orthodontic Society revises guidelines for clinical radiographyAmerican journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics 2008 134(5):597-98. [Google Scholar]
[8]. P Soni, V Sharma, J Sengupta, Cervical vertebrae anomalies-incidental findings on lateral cephalogramsThe Angle orthodontist 2008 78(1):176-80. [Google Scholar]
[9]. DL Turpin, Befriend your oral and maxillofacial radiologistAmerican journal of orthodontics and dentofacial orthopedics : official publication of the American Association of Orthodontists, its constituent societies, and the American Board of Orthodontics 2007 131(6):697 [Google Scholar]
[10]. A Kalan, M Tariq, Foreign bodies in the nasal cavities: a comprehensive review of the aetiology, diagnostic pointers, and therapeutic measuresPostgraduate medical journal 2000 76(898):484-87. [Google Scholar]