A Rare Case of Autoimmune Hypophysitis Presenting as Temperature Dysregulation
Ankur Jain1, Dinesh K. Dhanwal2
1Post Graduate Student, Department of Medicine,Maulana Azad Medical College, Bahadur Shah Zafar Marg, Delhi, India.
2Director Professor, Department of Medicine,Maulana Azad Medical College, Bahadur Shah Zafar Marg, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ankur Jain, BL-Taneja Block, Department of Medicine, Maulana Azad Medical College, Bahadur Shah Zafar Marg, Delhi-110002, India.
E-mail: drankur589@yahoo.in
Autoimmune hypophysitis is a rare cause of pan-hypopituitarism. Hypothalamic involvement in autoimmune hypophysitis is rare and usually manifests as central diabetes insipidus due to antibodies against arginine vasopressin. Temperature dysregulation is occasionally seen with suprasellar tumours but has never been reported with hypophysitis. We report a case of a middle aged man who presented to us with the complaints of documented body temperature fluctuations since two months followed gradually by hoarseness of voice, sexual dysfunction and syncope. Examination was remarkable for postural hypotension, dry coarse skin and delayed ankle reflexes. Patient’s hormone profile revealed pan-hypopituitarism and elevated titre of anti-TPO antibodies. Patient’s work up for secondary causes of hypopituitarism was negative. MRI brain revealed typical findings of hypophysitis. Patient was suspected as a case of autoimmune hypophysitis and was immediately treated with prednisolone along with hormone replacement. Rapid response within 30 days was observed in the form of subsidence of temperature fluctuations, improvement in general well being, sexual function and repeat MRI done after one month which revealed a partial empty sella. Autoimmune hypophysitis as a potentially treatable cause of temperature dysregulation has been highlighted in this case.
Hypophysitis, Hypothalamic dysfunction, Pan-hypopituitarism
Case Report
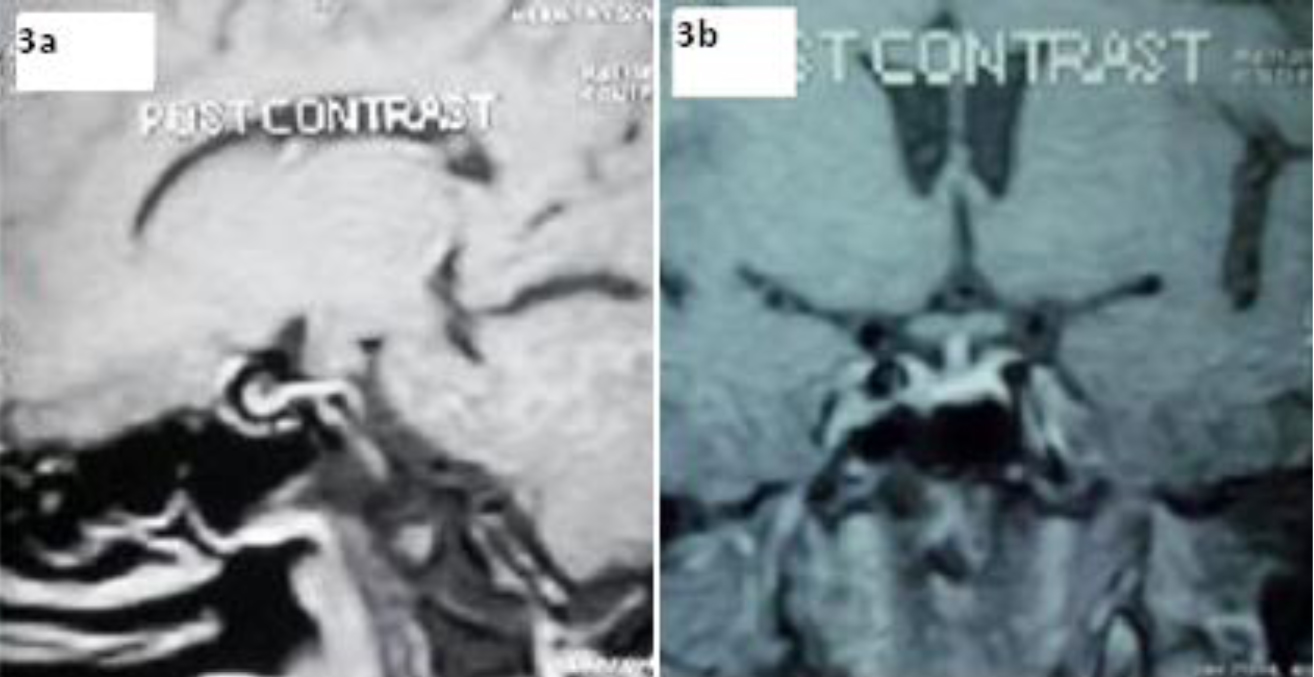
We report a case of a 56-year-old man (70kg) who presented to our out-patient department in February 2014 with the complaints of alternating periods of excessive heat and cold intolerance and body sweating which was associated with excessive shivering and documented fluctuations in body temperature throughout the day since past two months. This was followed by hoarseness of voice, constipation, loss of libido, erectile dysfunction and orthostatic dizziness after one month. There was no history of visual loss, vomiting, polyuria, polydipsia, diabetes, hypertension, weight loss, fever, cough, expectoration, headache, oral ulcers, leg ulcers, skin rash or head trauma. On examination, patient was conscious and oriented to time, place and person with BP of 110/60 mm Hg associated with postural fall, pulse rate-78/min, regular. There was mild pallor, but no icterus, clubbing, lymphadenopathy or skin pigmentation. CNS examination revealed delayed relaxation of ankle reflexes without any meningeal, cerebellar signs. Examination of fundus, cardiovascular, respiratory and abdomen were unremarkable. Patient was clinically suspected as a case of panhypopituitarism. Patient’s routine investigations and pituitary hormone profile are summarized in the given table [Table/Fig-1]. Patient’s 24 h urinary output was 2.1L. Patient’s hormone profile was consistent with panhypopituitarism. Patient was worked up for secondary causes of pan-hypopituitarism. Patient’s chest-X-ray, Electrocardiogram, liver and kidney function tests were normal. Tuberculin skin test was negative. Serum Angiotensin converting enzyme (ACE) levels, Anti-nuclear antibodies (ANA), anti-double stranded DNA, Anti-neutrophil cytoplasmic antibodies (ANCA), HIV-1 and HIV-2, viral markers, VDRL test for syphillis were negative. Patient’s CSF analysis was acellular and biochemistry was normal, Polymerase chain reaction (PCR) for Mycobacterium tuberculosis, gram’s stain, fungal stain, VDRL test for syphillis were negative. Patient’s hemoglobin electrophoresis was normal and malignancy work up including Carcinoembryonic antigen (CEA) levels, alpha fetoprotein (AFP) levels and CA-199 levels were unremarkable. Non contrast CT scan of head was normal. Patient’s MRI brain with pituitary fossa revealed bulky pituitary gland with symmetrical and conical shape associated with stalk thickening and dense homogenous post-contrast enhancement of the lesion [Table/Fig-2a,b]. After ruling out secondary causes of hypopituitarism like tuberculosis, sarcoidosis, syphillis, connective tissue disorders, vasculitis, metastasis, sickle cell disease and based on the characteristic imaging findings, a provisional diagnosis of auto-immune hypophysitis was made and patient was empirically started on hormone therapy in the form of prednisolone (60mg/day), levothyroxine (75 mcg/day) and testosterone. Patient improved symptomatically within 30 d of treatment and his temperature fluctuations subsided and there was an improvement in general well being and sexual function. Repeat MRI brain done after one month revealed partial empty sella [Table/Fig-3a,b], hence retrospectively confirming the diagnosis of autoimmune hypophysitis. Patient is still in our follow up.
Discussion
Autoimmune hypophysitis is a rare condition, first described in 1962. It classically affects females (F: M=8:1) and presents in late pregnancy or early post-partum period [1]. Associations with other autoimmune disorders have been described in the literature including Hashimoto’s thyroiditis, atrophic gastritis, pernicious anaemia, ovarian failure and adrenalitis [2]. Inflammatory process usually involves the anterior pituitary, however extension into posterior pituitary and pituitary stalk (Infundibulohypophysitis) have been described in the literature and anti-pituitary antibodies have been reported in association with this disease. Patients with autoimmune hypophysitis commonly present with hypopituitarism (63%), mass effects (56%), hyperprolactinemia (38%) and central diabetes insipidus (19%) [1]. Hypothalamic involvement in autoimmune hypophysitis has rarely been described and usually manifests as central Diabetes Insipidus. Earlier thought to be due to possible expansion of an inflammatory process from anterior to posterior lobe, with consequent inhibition of the axonal transport of antidiuretic hormone, hypothalamic involvement has now been shown to be due to the anti-hypothalamic antibodies targeting AVP secreting neurons, strongly suggesting the presence of hypothalamic autoimmunity in autoimmune hypophysitis [3]. Hypothalamus acts as the master of temperature regulation of the body and centre for temperature regulation has long been appreciated as preoptic nucleus and anterior hypothalamus [4]. Temperature dysregulation in hypothalamic disorders has been extremely rare even with compression from suprasellar tumours due to bilateral localization of hypothalamic nuclei and an extensive compensatory mechanism [5]. Temperature dysregulation has been reported in the literature mainly in relation to suprasellar tumours. Dziurzynski et al., reported a case of choroid glioma of the third ventricle presenting with diabetes insipidus, panhypopituitarism, mental status changes and temperature dysregulation [6]. A case of temperature dysregulation manifesting as hypothermia has been reported by de Vetten et al., after the resection of craniopharyngioma [7]. Temperature dysregulation in association with autoimmune hypophysitis has never been described in the literature till date. Our patient presented initially with temperature dysregulation and later progressed to panhypopituitarism. Patient’s workup for possible secondary etiologies of hypopituitarism was negative. Although, the diagnosis of autoimmune hypophysitis classically requires a histological confirmation by biopsy, we suspected this entity on the basis of characteristic imaging findings, anti-TPO antibody positivity and absence of other causes, which was confirmed retrospectively by rapid clinical and radiological response of the patient to prednisolone. Hypothyroidism, although can present as cold intolerance, does not cause features like shivering, sweating or wide body temperature fluctuations. Absence of central diabetes insipidus in our patient makes direct involvement of pituitary stalk and hence hypothalamus, an unlikely pathology underlying the patient’s symptoms. Since hypophysitis radiographically presents as a pituitary mass lesion and mimics a suprasellar pituitary adenoma, we hypothesize that temperature dysregulation in our case might be due to a mass effect of the enlarged pituitary gland on temperature regulating centre of the hypothalamus or may represent an autoimmune process involving the temperature regulating centre of the hypothalamus. Hence, autoimmune hypophysitis represents a potentially treatable cause of temperature dysregulation and a trial of glucocorticoids is justified in case of strong clinical and radiological suspicion.
Table showing the biochemical investigations of the patient
| Parameter | Patient’s Value | Normal Value | Parameter | Patient’s Value | Normal Value |
|---|
| Hemoglobin(g/l) | 127 | 133-162 | TSH (m IU/L) | 0.12 | 0.34-4.25 |
| Total cell count (x109) | 6.70 | 3.54-9.06 | Free T3 (pmol/L) | 0.022 | 3.7-6.5 |
| Platelets (x109) | 172 | 165-415 | Free T4 (pmol/L) | 2.83 | 9.0-16 |
| ESR (mm/hour) | 45 | 0-15 | Prolactin (m IU/L) | 84.9 | 53-360 |
| Fasting sugar (mmol/L) | 5.43 | 4.2-5.6 | FSH (IU/L) | 3.6 | 1-12 |
| Serum sodium (mmol/L) | 145 | 136-146 | LH (IU/L) | 0.28 | 2-12 |
| Serum potassium (mmol/L) | 4.5 | 3.5-5.0 | Testosterone (nmol/L) | 6.9 | 9.36-37.10 |
| Serum calcium (mmol/L) | 2.45 | 2.2-2.6 | Serum cortisol (nmol/L) | 121.2 | 138-690 |
| Serum phosphorous (mmol/L) | 1.13 | 0.81-1.4 | Anti-TPO antibodies (IU/L) | 400 | <35 |
MRI brain of the patient (post-contrast) showing enlarged and bulky pituitary gland (2a) and conical shape of the pituitary gland with a thickened stalk (2b)

Post-treatment MRI of the pituitary fossa of the patient (post-contrast) after one month showing a partial empty sella (3a and 3b)
Conclusion
Temperature dysregulation is a challenging clinical problem, both diagnostically as well as therapeutically and represents a rare manifestation of hypothalamic disorders. Hypothalamic involvement in autoimmune hypophysitis may occur as a result of direct expansion of the inflammatory process or possible anti-hypothalamic antibodies. Present case highlights the fact that in patients presenting with prominent temperature dysregulation, an early suspicion of autoimmune hypophysitis can lead to its prompt diagnosis and management can relieve the alarming symptoms of the patient. Autoimmune hypophysitis therefore might represent a potentially treatable cause of temperature dysregulation.
[1]. CC Cheung, S Ezzat, HS Smyth, SL Asa, The spectrum and significance of primary hypophysitisJ Clin Endocrinol Metab 2001 86:1048-53. [Google Scholar]
[2]. H Koshiyama, H Sato, S Yorita, T Koh, T Kanatsuna, K Nishimura, Lymphocytic hypophysitis presenting with diabetes insipidus: case report and literature reviewEndocr J 1994 41:93-97. [Google Scholar]
[3]. A De Bellis, E Sinisi, HP Pane, A Dello lacovo, G Bellastella, G Di Scala, Involvement of hypothalamus autoimmunity in patients with autoimmune hypopituitarism: role of antibodies to hypothalamic cellsJ Clin Endocrinol Metab 2012 97:3684-90. [Google Scholar]
[4]. JA Boulant, Role of the preoptic-anterior hypothalamus in thermoregulation and feverClin Infect Dis 2000 31(Suppl 5):S157-61. [Google Scholar]
[5]. HE Clar, Disturbances of the hypothalamic thermoregulationActa Neurochir(Wien) 1985 75:106-12. [Google Scholar]
[6]. K Dziurzynski, JB Delashaw, SH Gultekin, CG Yedinak, M Fleseriu, Diabetes insipidus, panhypopituitarism, and severe mental status deterioration in a patient with chordoid glioma: case report and literature reviewEndocr Pract 2009 15:240-45. [Google Scholar]
[7]. L de Vetten, G Bocca, Systemic effects of hypothermia due to hypothalamic dysfunction after resection of a craniopharyngioma: case report and review of literatureNeuropediatrics 2013 44:159-62. [Google Scholar]