Periodontal disease can no longer be regarded as a universally prevalent condition to which all members of the world are at equal risk if they do not practice good oral hygiene. At present it is well established that periodontal disease is predominantly associated with bacterial infection and host response. Nevertheless, the rate and development of the disease, beginning and severity of the disease are often determined by systemic risk factors in the host like gender, smoking, alcohol, diabetes, stress and genetic factors [1]. Identification of these periodontal risk factors have contributed extremely large to our understanding of pathogenesis of periodontal disease, there by building up new pathways for periodontal therapy as well as for periodontal disease prevention who are at risk [2].
As the knowledge regarding understanding of periodontal disease initiation, progression and response to treatment has grown up, interest has developed in finding means by which to translate this knowledge effectively into the care of each individual. Risk factors such as smoking, diabetes and pathogenic bacteria and microbial tooth deposits have been identified to have specific role in modifying the disease progression [3]. An understanding of these factors is necessary to prevent and control periodontal disease in the population. The risk factors to which the subjects are exposed may vary in different populations and hence knowledge of the factors is essential for subjective diagnosis and prediction of risk. Recognition of risk factors of periodontal disease and their possible role in progression of the disease process has changed the preventive and therapeutic success.
Accordingly, a comprehensive assessment of patient’s risk characteristics would appear to be necessary to calculate individual risk more accurately to formulate prognosis and tomake informed treatment decisions. It also helps to determine the frequency and extent of professional support necessary to maintain the CALs obtained following active therapy. The determination of such risk levels would thus prevent under treatment and also overtreatment during supportive periodontal therapy [4].
Various risk assessment models for periodontal disease are in popular, such as the Oral Health Information Suite (OHIS) and the Periodontal Risk Calculator (PRC). But, these models have been used prospectively or retrospectively to assess and calculate the individualized total risk profile at the onset of treatment and interpretation of data from a risk assessment model [5]. PRA model by Lang and Tonetti (2003) and modified PRA model by Viswa Chandra (2007) are primarily retrospective, where information is gathered to assess the risk for a patient at the time of diagnosis or during the supportive periodontal therapy or after active therapy has been completed. These risk assessment models evaluate simultaneously a spectrum of risk factors and risk indicators and construct a functional diagram, i.e. periodontal pentagon risk diagram which are viable algorithms to assess risk in the clinical setting [6].
PRA model evaluates the severity of periodontal disease by measuring the PD and radiographic evaluation of alveolar BL with other systemic factors into consideration. To overcome the limitations like lack of predictive power for periodontal tissue breakdown and time consuming process, modified PRA model has been suggested to measure CAL instead of alveolar BL [7].
Thus the present study was done to assess the periodontal risk status among individuals using PRA and modified PRA model and also to compare their efficiency of both the models in assessment of periodontal risk.
The present study was designed to evaluate the periodontal risk among individuals, using two different PRA models, i.e. PRA and modified PRA models.
Materials and Methods
This is a descriptive cross-sectional study in which 50 adult subjects (25 female and 25 male) aged 30 to 60 y attending the Outpatient Department of SIBAR Institute of Dental Sciences, Guntur, diagnosed with chronic periodontitis were enrolled in the study. Individuals with difficulty in mouth-opening and those with less than 20 functional teeth were excluded from the study.
Informed consent was taken before the start of the study, and ethical clearance was obtained from the institutional ethical committee. Periodontal status was measured using community periodontal index (Ainamo et al.,) with score 4 were included in the study [8]. Charting of periodontal status in accordance with PRA model such as, percentage of sites with BOP, number of sites with PD ≥ 5mm, BL/age ratio, number of tooth loss, diabetic status and smoking were assessed. The alveolar bone loss was assessed using intra-oral periapical radiographs (IOPA) of the areas with PD greater than 5mm using millimeter grid [9].
In modified PRA model, BOP, number of sites with PD ≥ 5mm, CAL/age ratio, number of tooth loss, diabetic status and smoking were also assessed [Table/Fig-1].
Coding system for BOP, sites with PD≥ 5mm, tooth loss, smoking, CAL/Age ratio and siabetic status for modified PRA model
| Axis Score | Bop | No. of Sites with PD≥ 5mm | Tooth Loss | Smoking (Cigarettes/Day) | CAL/age ratio | Diabetic Status |
|---|
| 0 | 0 | 0 | 0 | Non smoker | 0 | <102 |
| 1 | ≤4 | 1-2 | 1-2 | Former smoker | ≤0.25 | 102-109 |
| 2 | 5-9 | 3-4 | 3-4 | <10 | 0.26- 0.5 | 110-117 |
| 3 | 10-16 | 5-6 | 5-6 | 10-19 | 0.51-0.75 | 118-125 |
| 4 | 17-25 | 7-8 | 7-8 | 20 | 0.76- 1.0 | 126-133 |
| 5 | >25 | >9 | >9 | >20 | >1 | ≥134 |
Systemic parameters like diabetes was further evaluated by categorizing the subjects with fasting blood glucose level <102 mg/dl indicates as score 0, score ranging between 102 and 109 mg/dl as score 1, score ranging between 110 and 117 mg/dl as score 2, 118-125 mg/dl as score 3, 126-133 mg/dl score as 4 and ≥134 mg/dl indicates as score 5, respectively. Dental status was assessed by evaluating the systemic factors with tooth related risk factors which may act as predisposing condition for periodontal disease with axis score ranging from 0 to 5 [7,10]. Socioeconomic status of the subjects was determined using Kuppuswamy classification as score 0 indicates no stressful environment, score 1 indicates upper high collar worker, score 2 indicates as white collar, score 3 as blue collar worker, score 4 indicates contract employment and score 5 as unemployed [11]. All the parameters were checked and marked on both the PRA and modified PRA models using Microsoft Excel, and the periodontal risk were assessed based on the findings and categorized as low, moderate and high.
Results
Total of 50 subjects (25 males and 25 females) with a mean age of 35.5± 2.96 years and had an average number of 27.7 teeth were examined. Among the study group 13 subjects were smokers and eight subjects were former smokers; one subject was confirmed with diabetics mellitus and the other three subjects had cardiac problem. Nine patients were with extreme stress because of health concern and unemployment. Five patients had given previous history of undergoing any form of periodontal therapy [Table/Fig-2].
| Variable | Total Number | Percentage |
|---|
| Age (30-60 years) | | |
| 30-40 years | 39 | 78% |
| 41-60 years | 11 | 22% |
| Mean Age : 35±2.96 | | |
| Sex | | |
| Male | 25 | 50% |
| Female | 25 | 50% |
| Percentage of sites with bleeding on probing | | |
| 0 | | |
| <4 | - | - |
| 5-9 | 16 | 32% |
| 10-16 | 15 | 30% |
| 17-25 | 03 | 06% |
| >25 | 13 | 26% |
| 03 | 06% |
| No. of sites with probing depth>5mm | | |
| 0 | 01 | 02% |
| 1-2 | 15 | 30% |
| 3-4 | 12 | 24% |
| 5-6 | 10 | 20% |
| 7-8 | 12 | 24% |
| >9 | - | - |
| >12 | - | - |
| Tooth loss (>12) | | |
| 0 | 15 | 30% |
| 1-2 | 18 | 36% |
| 3-4 | 11 | 22% |
| 5-6 | 06 | 12% |
| 7-8 | - | - |
| > 9 | - | - |
| ≥ 12 | - | - |
| Smoking (no. of cigarettes/day) | | |
| Non-smokers | 29 | 58% |
| Former smokers | 08 | 16% |
| Current smoker | 04 | 08% |
| <10 | 04 | 08% |
| 10-19 | O5 | 10% |
| ≥ 20 | - | - |
| Socio-economic status | | |
| Score - 0 | 03 | 06% |
| score - 1 | 07 | 14% |
| score - 2 | 16 | 32% |
| score - 3 | 10 | 20% |
| score - 4 | 05 | 10% |
| score – 5 | 09 | 18% |
| Diabetic status | | |
| Score –0 | 47 | 92% |
| score - 1 | - | - |
| score - 2 | - | - |
| score - 3 | - | - |
| score - 4 | - | - |
| score – 5 | 03 | 7% |
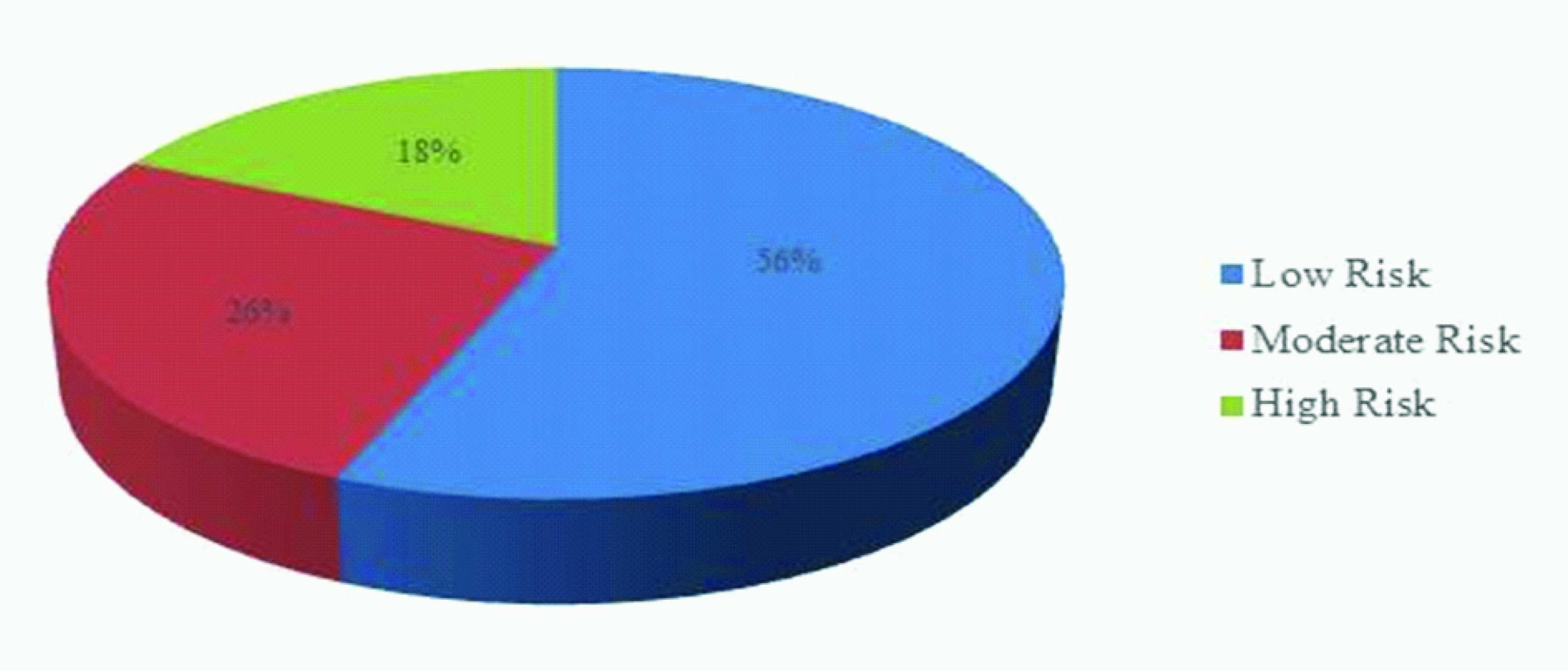
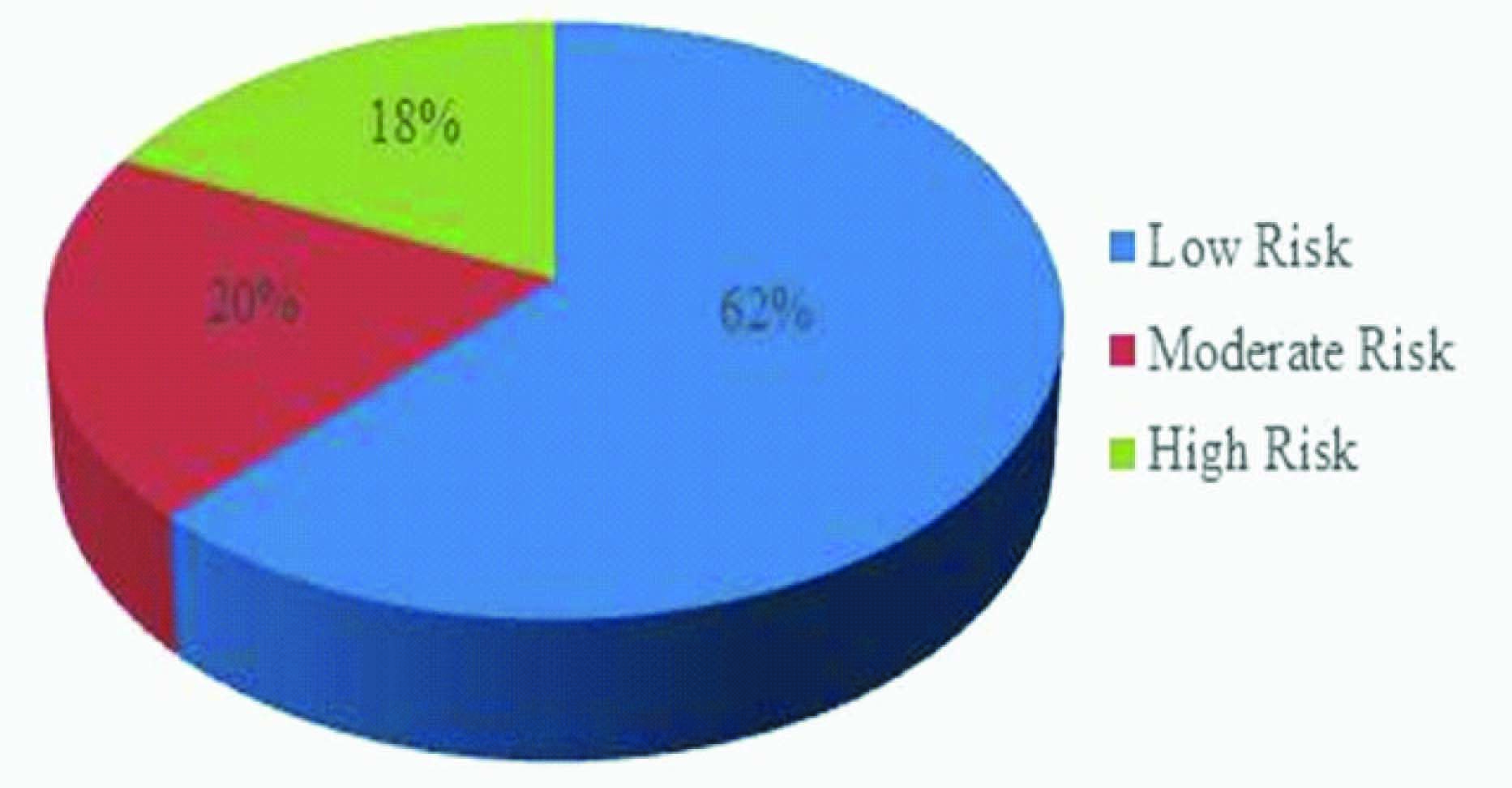
According to the PRA model (Lang and Tonetti) 28 subjects were atlow risk, 13 subjects were at moderate risk and 9 subjects were at high risk, whereas 31 subjects were at low risk, 9 subjects were at moderate risk and 10 subjects were at high risk were identified by modified PRA model given by Viswa Chandra. Thus by evaluating both the models, the number of cases at high risk level, moderate risk level and low risk level were similar with percentages of low risk levels were similar with percentages of cases at high risk were 18% and 20%, moderate risk were 26% and 18% and at low risk were 56% and 62% respectively, which was not significant [Table/Fig-3,45].
Distribution of high, moderate and low risk cases according to the PRA and modified PRA model
| Models | High risk | Moderate risk | Low Risk | Total |
|---|
| PRA Model | 9(18%) | 13(26%) | 28(56%) | 50(100%) |
| Modified PRA Model | 10(20%) | 9(18%) | 31(62%) | 50(100%) |
Distribution of high, moderate and low risk cases according to the PRA model
Distribution of high, moderate and low risk cases according to the modified PRA model
Discussion
Long-term studies strongly suggest that clinicians can achieve success in establishing and maintaining periodontal health using conventional therapeutic modalities alone with estimating risk factors for further disease progression [12]. The present study was done to evaluate the risk assessment using PRA model and modified PRA model; also to compare the risk estimation ability between these two models. Various risk assessment models have been developed, which range from a simple questionnaire to a more complicated model like PRC developed by (Page et al.,). PRC evaluates 11 key risk parameters like patient’s age, smoking, diagnosis of diabetes, history of periodontitis surgery, Probing depth, BOP, furcation involvement, sub gingival restorations, root calculus, radiographic bone height and the presence of vertical bone lesions [10]. Based on these parameters, “numeric risk and disease severity scores are calculated that establish both an assessment of risk as well as a quantification of disease severity and predict risk with a high level of accuracy [5].
Another risk assessment tool is the OHIS (Page et al.,), which could provide a comprehensive and systematic approach to clinical decision- making to periodontitis and a quantitative information to the clinician and patient as an aid to diagnosis and to facilitate individual, needs-based treatment planning, reduction in oral healthcare costs, and improved clinician productivity and income [13]. Trombelli et al., proposed a simplified risk assessment model called Union of European railway industries simplified method (UniFe) using five key parameters: smoking status, diabetic status, number of sites with PD ≥ 5 mm, BOP score, and BL/age. A numeric value for each parameter was calculated, based on its extent or severity, and patients were assigned to 1 of 5 risk categories derived from the sum of those values [14].
PRA model is based on a multifactorial graphic i.e., the Periodontal Pentagon Risk Diagram. This functional diagram is composed of six vectors representing a combination of six clinical, systemic, and environmental factors to predict the risk of recurrence of periodontitis, and patients are classified as low, moderate, or high-risk profile. The parameter which were included in these model are known risk factors such as BOP along with increased probing depth may serve as an indicator for future loss of periodontal attachment [15]. BL can be equated with CAL although it succeeds it by 6–8 months (Goodson et al.,) [14–17]. Since tooth loss also represents a true end point outcome variable reflecting the patient's history of oral diseases and trauma, it is logical to incorporate this risk indicator. The aggregate sum of these factors provides an individualized total risk profile for the patient. The PRA provides an assessment of risk for patients during the supportive, post treatment phase, after active therapy has been completed. However, the PRA model has the following limitations. a) it mainly assesses the cumulative status of a periodontitis patient, b) there is no proper identification of risk factors and risk determinants, c) in the functional diagram, the presence of a systemic disease is assessed as a high-risk factor with no emphasis on the current status of a disease, d) smoking is assessed in the risk assessment model but another potential risk factor, diabetes, is not assessed separately and is included in the systemic diseases category, e) it does not take into account the various dental factors, which may modify or initiate the progression of periodontal disease [6].
Numerous other health problems may modify the progression of periodontal disease and the host response play an important role by varying from an inadequate response to an exaggerated response (Klokkevold and Mealy) [18]. Socio-economic status and stress are the other important background characteristics to assess the risk for periodontal disease. Socio-economic status relates to decreased awareness and decreased dental visits whereas psychosocial factors or stress has the direct association with periodontitis (Axtellius et al., [19] and (Novak and Novak) [15].
Based on the limitations of PRA model, Viswa Chandra has proposed a Modified PRA model with considering four entities from the PRA risk assessment model were retained in the new model: BOP, probing depth (PD), tooth loss and smoking. The entities that were added in the new model included various aspects of risk assessment, especially risk factors (diabetes, and tooth deposits or factors that may retain deposits) and other risk determinants such as socio-economic factors and stress (Page and Beck, 1997) [17]. The large body of evidence showed that Diabetes is a known biological risk factor that leads to the initiation and progression of periodontitis. According to the American Academy of Periodontology, 2000 the diagnosis of diabetes mellitus was known well by fasting blood glucose level than other diagnostic test. The values of fasting glucose less than 110mg/dl considered as low risk, and more than 126mg/dl considered as high risk. Any value falling in between the low risk and high risk levels were categorized as moderate risk (Genco and Loe 1993) [10].
Risk is assessed as follows: A low-periodontal-risk patient has all the parameters in the low-risk areas or at the most one parameter in the medium-risk area according to the PRA model. Whereas in modified PRA model a low-periodontal-risk patient has all the parameters in the low-risk category or at the most two parameters in the moderate and high risk area [Table/Fig-6,7]. A moderate-periodontal-risk patient has two parameters must be in the moderate-risk category and not more than one parameter in the high risk category according to the PRA model. However, inmodified PRA model a moderate-periodontal risk patient has at least three parameters in the moderate risk area and not more than one parameter in the high risk area. A high-periodontal-risk patient must has only two parameters in the high-risk category according to the PRA model, which differ from modified PRA model in that at least two parameters in the high-risk category [Table/Fig-8,Table/Fig-9,10] [6,9].
Risk diagram of a low periodontitis risk patient according to PRA model. Scores of the patient plotted a 16% of sites with BOP, 4 sites with PD≥5, 4 lost teeth and BL/age ratio 0.25

Risk diagram of the same low periodontitis risk patient according to modified PRA model. Scores of the patient plotted are 16% of sites with BOP, 4 sites with PD≥5, 4 lost teeth and BL/age ratio 0.25

Risk diagram of a high periodontitis risk patient according to PRA model. Scores of the patient plotted are 25% of sites with BOP, 8sites with PD≥5, ≥12lost teeth and BL/age ratio of ≥1.5, diabetic and an occasional smoker

Risk diagram of the same high periodontitis risk patient according to modified PRA model. Scores of the patient plotted are 25% of sites with BOP, 8sites with PD≥5, ≥12lost teeth and BL/age ratio of ≥1.5, with a fasting blood glucose level of 126-133 mg/dl, periodontal abscess and living a stressful environment

Categorization of risk levels
| Risk levels | PRA model | Modified PRA model |
|---|
| Low risk | All parameters in the low risk area or at the most one parameter in the moderate risk category | All parameters in the low risk area or at the most one parameter in the moderate and high risk category |
| Moderate risk | Two parameter must be in the moderate risk category and not more than one parameter in the high risk categoryor the presences of one parameter each in moderate and high risk as moderate | At least three parameters in the moderate risk area and not more than one parameter in the high risk area |
| High risk | At least two parameters in the high-risk category | At least two parameters in the high risk category |
Subjects with maximum of two parameters in the moderate risk or high risk are considered as low risk individuals in both the models [Table/Fig-6,7]. According to PRA model, subjects with two parameters in the moderate risk area and not more than one at high risk are categorized as moderate risk subjects. Whereas in modified PRA model a minimum of three parameters in the moderate risk area not more than one parameter in high risk are categorized as moderate risk subjects. In both the models a periodontal risk patient with at least two high risk parameters is categorized in the high-risk category [Table/Fig-8-10] [6,9].
In the present study, 50 subjects aged between 30-60 y and diagnosed with chronic periodontitis were examined. All the subjects had generalized BOP and at least one site with probing PD ≥ 5mm showing that both these risk factors fall into low risk category. There were thirteen current smokers, eight former smokers, five subjects with past periodontal history, three subjects were diabetic, three subject with cardiac complaint and nine subjects were under extreme stress because of health concern and unemployment [Table/Fig-2]. When all these entities were drawn, according to PRA model, 18% were at high-risk cases and 26% were at moderate risk and 56% were low-risk cases. In the modified PRA model, 20% of high-risk cases, 18% were of medium risk case and 62% of low-risk cases were identified [Table/Fig-3-5].
The number of smokers in the present study were 21 (13 subject were current smokers and eight subjects were former smokers) among them five subjects fall into high risk in both the models whereas in the remaining 16 subjects eight subjects were categorized as moderate risk and rest of the eight subjects in low risk in both the models.
Three subjects were diagnosed as diabetic with fasting blood glucose level falling in the range of between 126 and 133 mg/dl and were categorized under high risk in both the models which is similar to previous study (Viswa Chandra) [6]. Out of ten subjects in Socioeconomic status, nine subjects shows the score five were categorized under high risk and one subject with moderate risk due to health concern.
Likewise, Shruthi et al., [20] have conducted a study to evaluate the periodontal risk of individuals using the modified periodontal risk assessment model with 30 patients. They identified 43.3% were in low risk group, 33.3% in moderate risk group, and 23.4% in high risk group by modified PRA Model whereas 66.6% patients were in low risk group, 16.6% in moderate risk group and 16.6% in high risk group when identified by PRA Model [18]. The variations between these studies can be attributed to variation in sample size, type and increased risk variables in the present population.
Conclusion
Evaluation of risk factors and customizing the individual treatment plan accordingly in the broadest senses can bring renaissances in the traditional approach to oral health care. A gradual progress from past decades in the assessment of risk, using risk models has driven in the reduction of morbidity and cost of health care. By comparing with earlier studies, the present study with more number of subjects has shown no difference between the two models even though additional risk factors were included in modified PRA model.