A Morphologic and Morphometric Study of Foramen Vesalius in Dry Adult Human Skulls of Gujarat Region
Binita B. Raval1, Praveen R. Singh2, Jaba Rajguru3
1Senior Resident, Department of Anatomy,Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
2Professor, Department of Anatomy,Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
3Assistant Professor, Department of Anatomy,Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Binita. B. Raval, Senior Resident, Department of Anatomy, Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
E-mail: purohitbinita@gmail.com
Introduction: The foramen Vesalius is located within bony plate between the foramen ovale and the foramen rotundum in the floor of middle cranial fossa. This foramen allows passage of emissary veins which communicate cavernous sinus and pterygoid plexus of veins.
AIM: To study the morphological and morphometric variations of foramen Vesalius in dry adult human skulls.
Materials and Methods: One hundred and fifty dry adult human skulls were studied for variations in size, shape, presence/absence and any duplication/multiplication of the foramen Vesalius. After collecting data, appropriate statistical analysis was done.
Results: The mean maximum dimension of foramen Vesalius was 0.98±0.67 mm on right side and 1.12±0.73 mm on left side. Foramen Vesalius was present in 90 (60%) skulls out of 150 observed. The incidence was 41(27.33%) on right side and 49 (32.67%) on left side. Foramen Vesalius was present unilaterally in 32 (35.56%) and bilaterally in 29 (32.23%) out of 90 skulls. Duplication of this foramen was observed in two skulls (one right side and one on left side). Foramen Vesalius was round in 72%, oval in 24% and irregular in 4% of total foramina present.
Conclusion: Foramen Vesalius was present in 60% of total skulls studied. The foramen showed variations in incidence and shapes, while there was no statistically significant difference in the maximum dimension between foramen Vesalius on right and left side. There could be some developmental reasons to explain these variations. The findings of this study could be important to anatomists and also equally essential for clinicians who approach middle cranial cavity for various procedures.
Emissary veins, Foramen vesalius, Morphology, Morphometry
Introduction
Foramina or openings in the floor of middle cranial fossa are very important as they allow passage of important structures such as nerves and blood vessels. The greater wing of sphenoid contains three consistent foramina and other small variable foramina. The consistent foramina are the foramen rotundum, foramen ovale, foramen spinosum. Accessory named foramina, foramen Vesalius and the cavernous foramen, may be present close to foramen ovale. Foramen Vesalius is one of the inconsistent foramen of the skull [1]. The incidence of occurrence of this foramen varies in different regions of the world as reported by various authors. The knowledge of three-dimensional topographic anatomy of skull structures and their morphometric values is needed but it is not sufficient for performing safe treatment. Therefore, detailed knowledge of anatomical variations is essential for clinicians who perform various invasive procedures on head and neck [2].
Foramen Vesalius (emissary sphenoidal foramen) is a small, variable but consistently symmetrical structure located antero-medial to foramen ovale and lateral to foramen rotundum [1]. It transmits sphenoidal emissary vein/veins connecting cavernous sinus with pterygoid venous plexus, thus communicating extracranial veins and intracranial venous sinus. Thus, septic thrombus from extracranial source can reach cavernous sinus producing thrombosis of cavernous sinus. The probable reason for this condition is the infection within the orbit and paranasal air sinuses. It can be due to infection involving upper half of the face. The condition is manifested by severe pain in the eye and forehead region due to involvement of ophthalmic division of trigeminal nerve. Trismus can occur if mandibular nerve is involved [2]. The valveless emissary veins help to balance between intracranial and extracranial pressure. Under normal circumstances, blood flow through emissary veins is slow. However, in cases of increased intracranial pressure, these veins become an important source of drainage of blood [2].
The neurosurgical procedure for treatment of trigeminal neuralgia is performed through foramen ovale, and while approaching this foramen the needle for microvascular decompression can be misplaced to foramen Vesalius due to proximity of these two foramina. The consequent puncture of cavernous sinus can produce serious complications [2-4].
Present study was aimed to observe variations in morphology and morphometry of foramen Vesalius. This study is of great importance to anatomists and also to clinicians who approach the area of middle cranial fossa for various invasive procedures.
Materials and Methods
The study was done in the Department of Anatomy of Pramukhswami Medical College and other medical colleges of Gujarat region for the duration of two years (January 2012 to January 2014) after obtaining permission from the Human Research Ethics Committee of our institute.
The present study included 150 intact dry adult human skulls of unknown sex. The skulls with broken floor of middle cranial cavity were excluded from this study. The incidence of occurrence of foramen Vesalius (bilateral and unilateral) was noted in the floor of the middle cranial fossa. A thin copper wire was used to confirm patency of foramina and rule out false passages. Measurement of foramen Vesalius was taken along the maximum diameter with the help of digital vernier caliper with a precision of 0.01 mm. The probes having diameter of 0.25 mm, 0.50 and 0.75 mm were used to measure minute foramina. Shapes of this foramen (round, oval, irregular) were observed bilaterally. Duplication of the foramen, if any was observed bilaterally.
Statistical Analysis
The data was recorded in tabular form. The results of the study were obtained by analysing data in SPSS software, version 14. Comparison of maximum dimension of foramen Vesalius was done on right and left sides of middle cranial fossa. Significance was considered when p-value was ≤ 0.05. The results were compared with those obtained by other workers cited in the available literature. Photographs were taken showing important variations of foramen Vesalius.
Results
After compiling the observations and using SPSS software, the following results were obtained, which are arranged in tabular form. [Table/Fig-1] shows comparison of mean of maximum dimensions of right and left sided foramen Vesalius of middle cranial fossa. The mean of maximum dimensions of this foramen was 0.98±0.67 mm on right side and 1.12±0.73 mm on left side, with no statistically significant bilateral difference. The shape of the foramen Vesalius was found to be round in 64 (72%), oval in 22 (24%) and irregular in 4 (4%) of total 90 foramina studied [Table/Fig-2]. Round, oval and irregular shaped foramina were also observed [Table/Fig-3,Table/Fig-4,Table/Fig-5].
[Table/Fig-6] shows unilateral, bilateral and total distribution of foramen Vesalius. The foramen was present in 90 (60%) of total skulls studied. Unilateral foramen Vesalius is shown in [Table/Fig-7]. Bilateral asymmetrical foramen Vesalius is shown in [Table/Fig-8]. Duplication of this foramen was observed in 1% of skulls (2 out of 150) which is shown in [Table/Fig-9,Table/Fig-10]. [Table/Fig-9] shows partial duplication of this foramen. Here the foramen shows presence of spine on its walls causing partial duplication. [Table/Fig-10] shows complete duplication of the foramen. Duplicated foramen is located posterior and medial to the main foramen Vesalius.
Discussion
The skull base including middle cranial fossa originates predominately from cartilaginous precursors with a small contribution from membranous bone. Therefore, it is known as chondrocranium. The components of the skull base are derived from neural crest cells and mesoderm during the fourth week of fetal life to form the cartilaginous and bony components of the cranial base [5]. Before any mesenchyme condenses to initiate the formation of cranial cartilage, the vessels and major cranial nerves occupy their position. Therefore, foramina of skull are specified before the bones are formed. The process of endochondral ossification in the skull is the same as that of the long bones except that each ossification centre is equivalent to primary centre. The ossification process follows the same programme of growth and remodelling. Growth takes place in the unossified cartilage between adjacent ossification centres. The first ossification centres appear in lesser and greater wings of sphenoid, at eight and nine week respectively [1].
Foramen Vesalius (emissary sphenoidal foramen) is a small, variable but consistently symmetrical structure as cited by Lanzieri et al., [6]. Total distribution of this foramen was lower in the studies done by various authors [7-18] as compared to present study as shown in [Table/Fig-11].
Andreas Vesalius (1543) in his famous book “De Humani Corporis Fabrica’’ says that there is no significant difference in the frequency of occurrence of foramen Vesalius between unilateral right and left sides. This is contradictory to what we found in our study (27.33% on right side and 32.67% on left side). The findings regarding total distribution, unilateral and bilateral presence of foramen Vesalius are compared with previous studies done by various authors in [Table/Fig-11].
In our study, the values of mean maximum dimension of foramen Vesalius were variable when compared with earlier studies [11-16]. These comparative morphometrical findings have been depicted in [Table/Fig-12]. Most of the studies did not show any significant difference between maximum dimensions on right and left sides, which is similar to current study. Lanzieri et al., [6] in their study, observed four patients (out of 50); in which asymmetry of foramen Vesalius was believed due to some pathology of structures surrounding that region. In two of these cases, asymmetry might be due to invasion of emissary vein and foramen Vesalius by tumours such as nasopharyngeal melanoma and juvenile angiofibroma. The asymmetry was also seen in association with carotid-cavernous fistula. They found one patient with neurofibromatosis who had exhibited asymmetric foramina [6]. Thus, asymmetry is more likely the result of a pathological process than a normal variant.
Duplication of foramen Vesalius was found in 1% of total skulls studied which was similar to findings in the study done by Kale et al., [10](1%), but lower than Singh et al., [13](2%).
The foramen Vesalius is one the important foramina at the skull base which allows passage of emissary veins connecting cavernous sinus and pterygoid plexus of veins. These veins act as potential channels for transmitting sepsis from extracranial veins to intracranial venous sinuses. In treatment of trigeminal neuralgia, needle targeting foramen ovale can be misplaced towards foramen vesalius causing serious intracranial bleeding [2,7].
Mean maximum dimension of foramen/distance (mm) n= number of foramina SD= standard deviation
| Foramen | Right side n=150 Mean ± SD | Left side n=150 Mean ± SD | p value |
|---|
| Foramen Vesalius | 0.98 ± 0.67 | 1.12 ± 0.73 | 0.343 |
Shapes of foramen Vesalius
n=number of foramina
| Shape | Distribution of shapes of foramen Vesalius |
|---|
| Right side n=41 | Left side n=49 | Total n=90 |
|---|
| Round | 34(83%) | 30(61%) | 64(72%) |
| Oval | 7(17%) | 15(31%) | 22(24%) |
| Irregular | 0 | 4(8%) | 4(4%) |
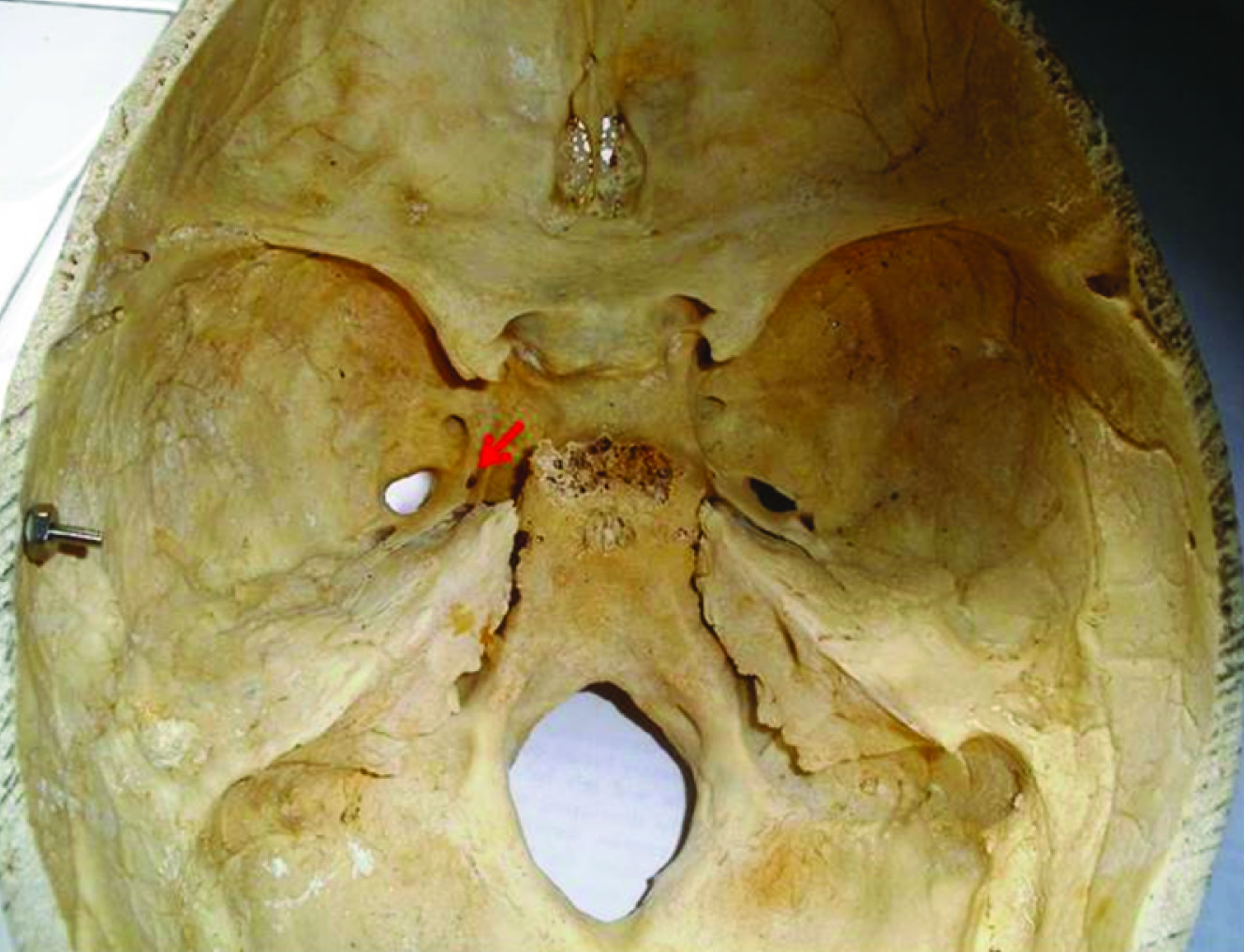
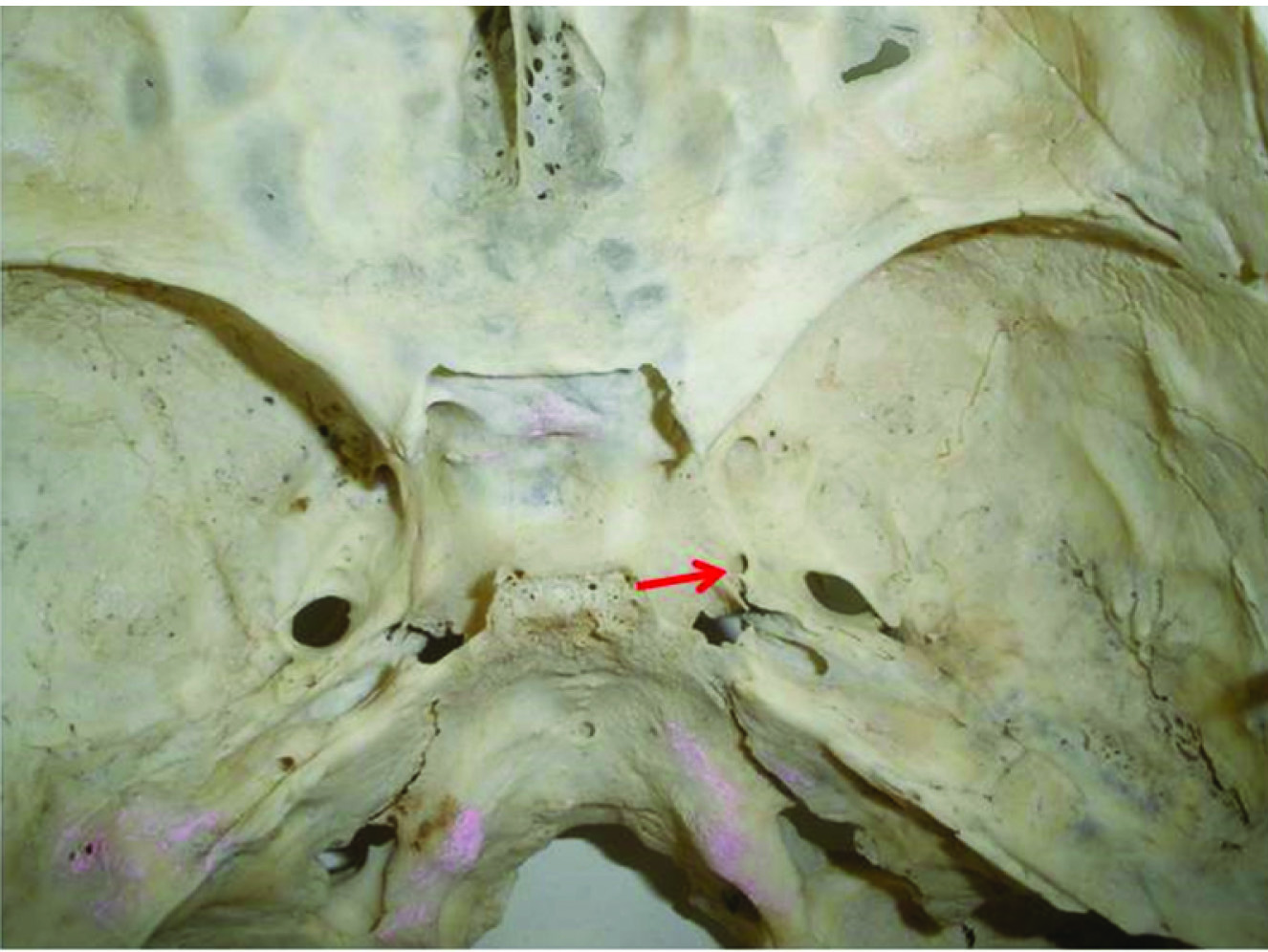
Middle cranial fossa showing round foramen Vesalius on left side (Red arrow)
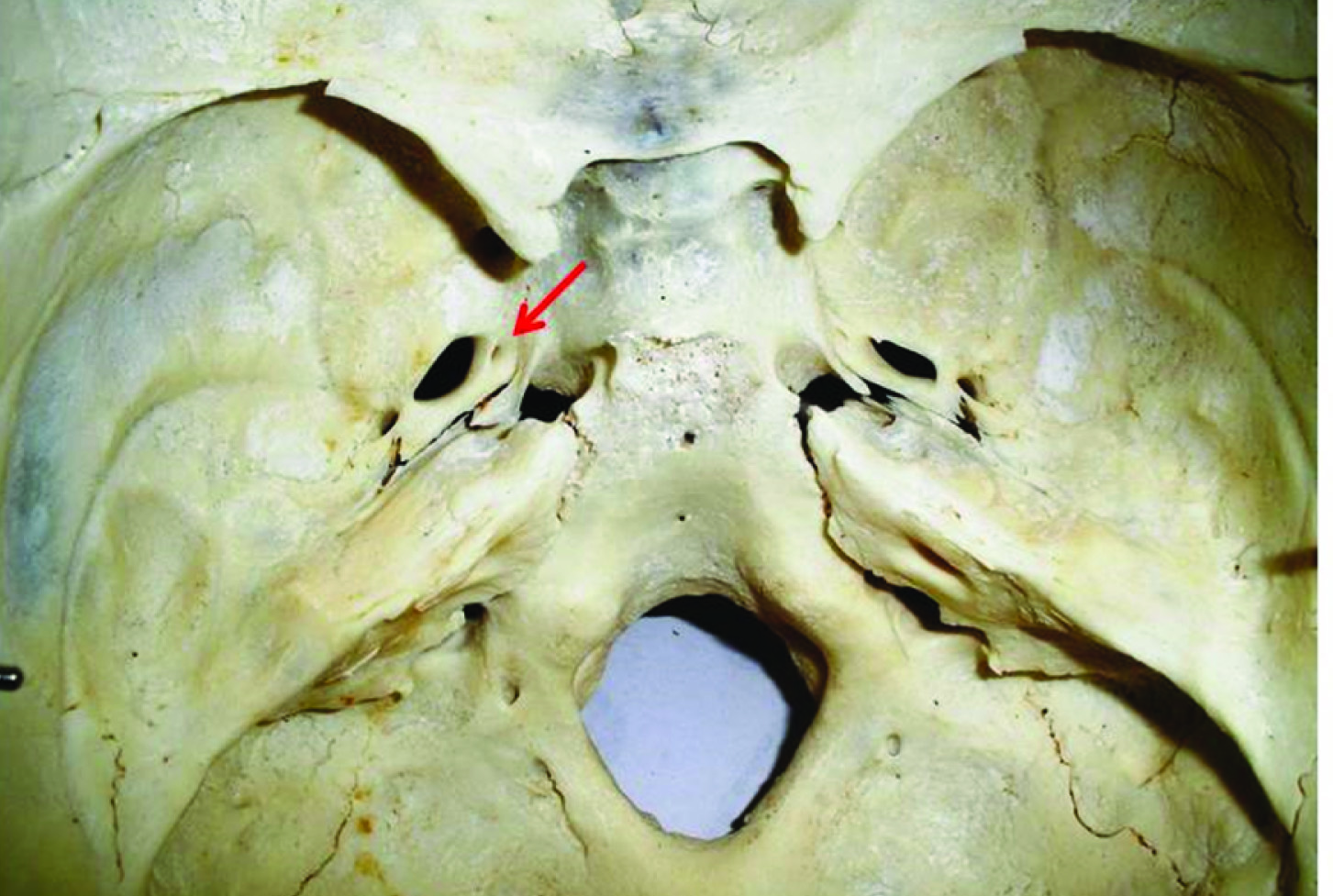
Middle cranial fossa showing oval shaped foramen vesalius on left side (Red arrow)
Middle cranial fossa showing irregular foramen vesalius on right side (Red arrow)

Distribution of foramen Vesalius
| Distribution | Right side | Left side | Distribution in 90 skulls(showing presence of foramen) |
|---|
| Unilateral | 12 | 20 | 32(35.56%) |
| Bilateral | 29 | 29(32.23%) |
| Total | 41 | 49 | 90(60%) |
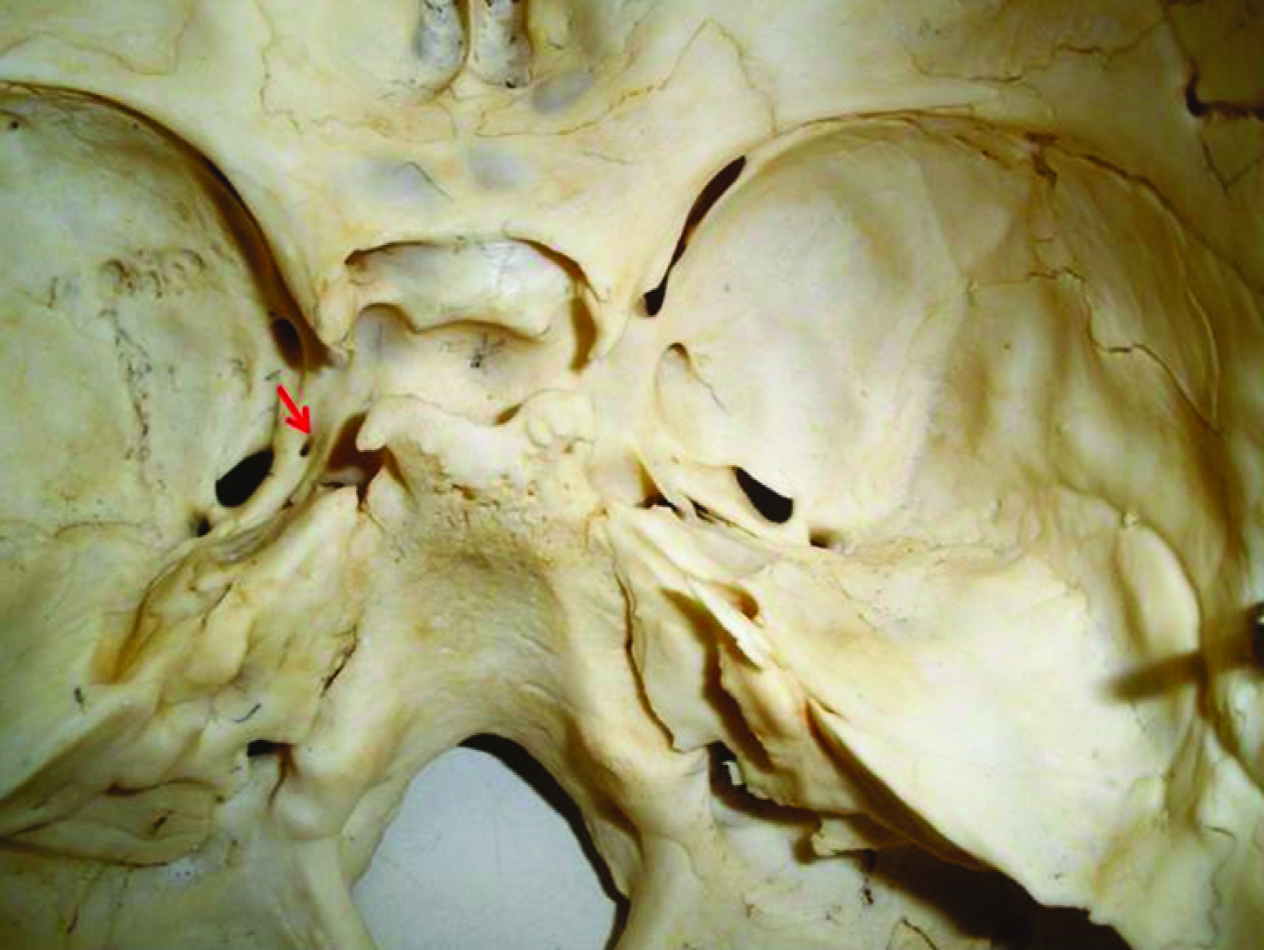
Middle cranial fossa showing unilateral foramen Vesalius on left side (Red arrow)
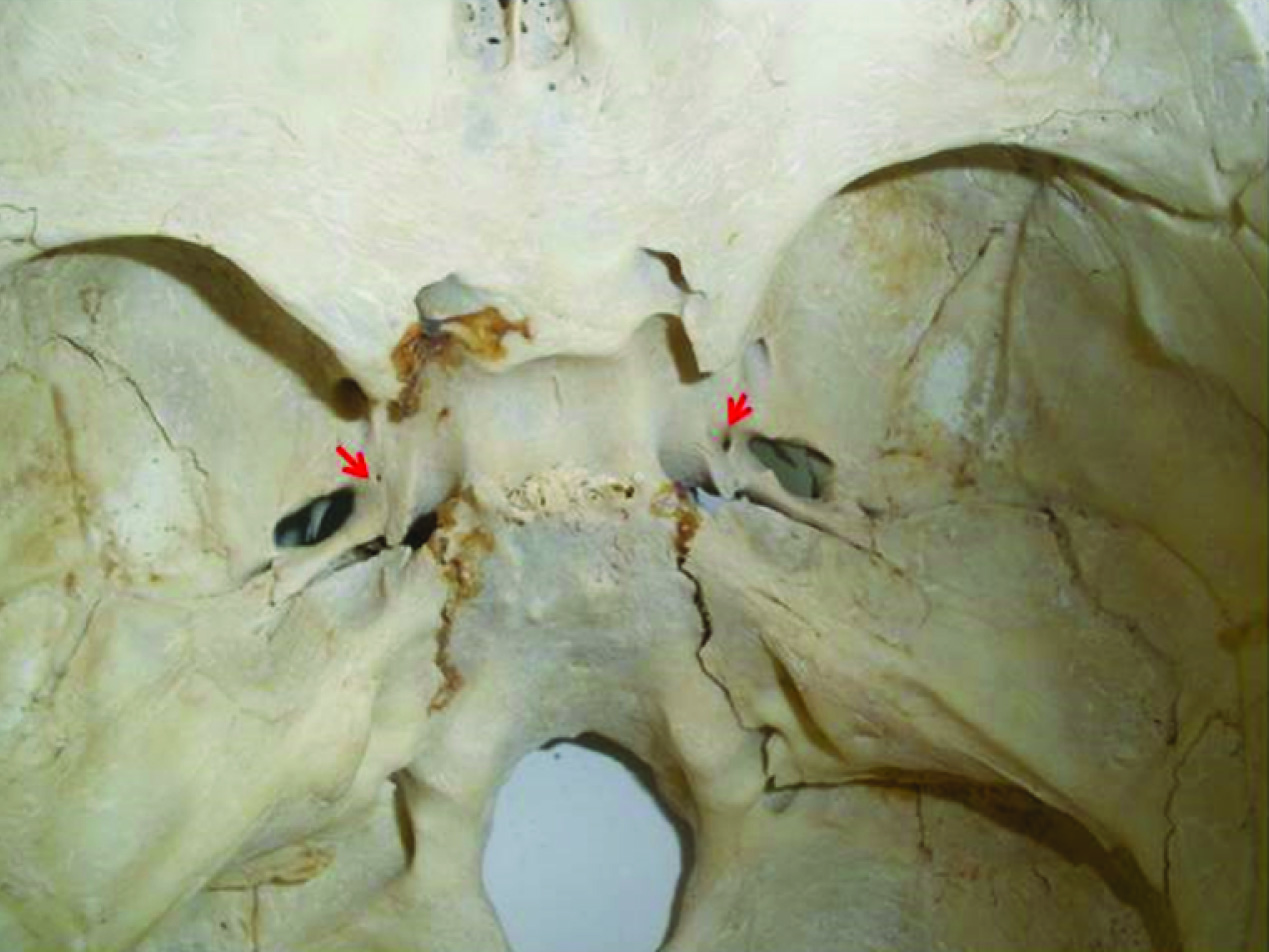
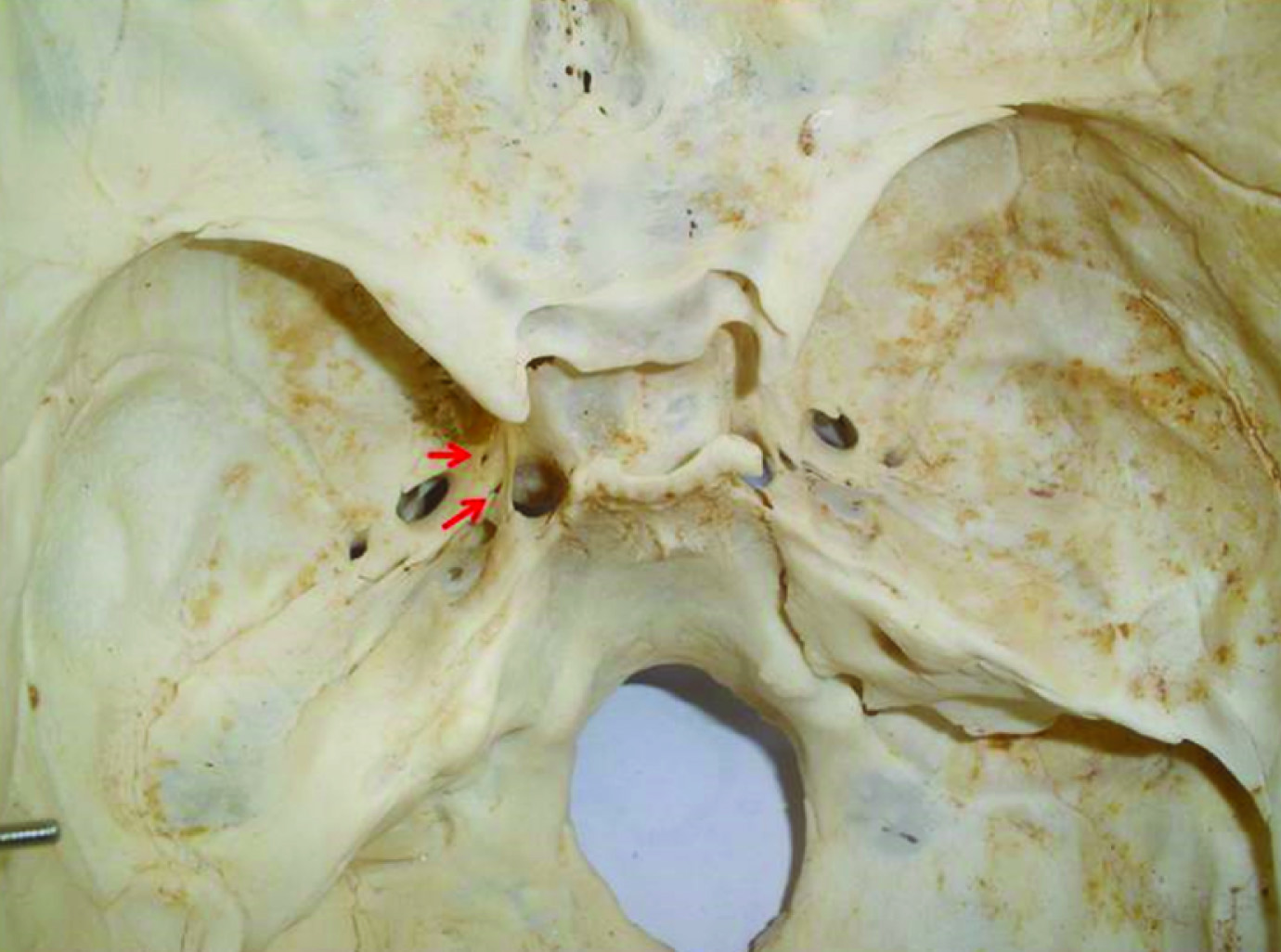
Middle cranial fossa showing bilateral asymmetrical foramen
Vesalius(Red arrows)
Middle cranial fossa showing partial duplication of foramen vesalius on right side (Red arrow)
Middle cranial fossa showing complete duplication of foramen vesalius on left side (Red arrow)
Incidence of foramen Vesalius shown by various authors
| Name of author | Year | Total distribution | Bilateral distribution | Unilateral distribution |
|---|
| Gupta et al.,[7] | 2014 | 34% | 14% | 20% |
| Kodama et al.,[8] | 1997 | 21.75% | - | - |
| Gupta et al.,[9] | 2005 | 32.85% | 22.85% | 20% |
| Kale et al.,[10] | 2009 | 45% | 25.1% | 19.9% |
| Shinohara et al.,[11] | 2010 | 33.75% | 15.5% | 18.25% |
| Rossi et al.,[12] | 2010 | 40% | 13.75% | 26.25% |
| Singh et al.,[13] | 2011 | 51% | - | 20% |
| Chaisuksunt et al.,[14] | 2012 | 10.9% | 12.7% | 4.5% |
| Shaik et al.,[15] | 2012 | 36% | 24% | 16% |
| Ozer et al.,[16] | 2013 | 34.8% | 9.3% | 25.5% |
| Nirmala et al.,[17] | 2014 | 50% | 23.3% | 26.67% |
| Srimani et al.,[18] | 2014 | 5% | - | - |
| Present study | 2014 | 60% | 32.23% | 35.56% |
Mean maximum dimension of foramen Vesalius reported by various authors
| Name of Author | Year | Mean maximum dimension(Right side) | Mean maximum dimension(Left side |
|---|
| Shinohara et al.,[11] | 2010 | 0.67 ± 0.28 mm | 0.76 ± 0.39 mm |
| Rossi et al.,[12] | 2010 | 1.457 ± 1.043 mm | 1.592 ± 0.938 mm |
| Singh et al.,[13] | 2011 | 0.79 mm | 0.96 mm |
| Chaisuksunt et al.,[14] | 2012 | 1.71 ± 0.58 mm | 2.22 ± 1.05 mm |
| Ozer et al.,[16] | 2013 | 0.86 ± 0.21 mm | 1.07 ± 0.37 mm |
| Present study | 2014 | 0.98 ± 0.67 mm | 1.12 ± 0.73 mm |
Conclusion
Foramen Vesalius is an inconsistent foramen of sphenoid bone. In our study, incidence of this foramen was 60% which is considerably higher than the previous studies. The exact cause of variations observed in current study is difficult to determine but these might be due to genetic, nutritional, environmental or other unknown factors. The detailed knowledge of anatomy and morphology including variations of foramen Vesalius, as observed in current study is of great importance to the clinicians in diagnosis and management of various conditions where micro-neurosurgical and microvascular approach is a requisite.
[1]. S Standring, Anatomy Gray’s, The Anatomical Basis of Clinical Practice. In external skull 2008 40th EditionLondonChurchill Livingstone Elsevier:424-25. [Google Scholar]
[2]. AR Freire, AC Rossi, VC Souza de Oliveria, FB Prado, PH Ferreira Caria , PR Botacin, Emissary foramens of the human skull: Anatomical characteristics and its relations with clinical neurosurgeryInt J Morphol 2013 31(1):287-92. [Google Scholar]
[3]. M Sindou, Y Keravel, B Abdennebi, J Szapiro, Neurosurgical treatment of trigeminal neuralgia. Direct approach or percutaneous method?Neurochirugie 1987 33(2):89-111. [Google Scholar]
[4]. WH Sweet, CE Poletti, Complications of percutaneous rhizotomy and microvascular decompression operations for facial pain. In Schmideck HH, SweetWH (eds) Operative neurosurgical techniques: indication, methods and resultsGrune and Straton, Ornaldo 1988 :1139-44. [Google Scholar]
[5]. WR Nemzek, HA Brodie, ST Hecht, BW Chong, CJ Babcook, JA Seibert, MR, CT, and plain film imaging of the developing skull base in fetal specimensAJNR Am J Neuroradiol 2000 21(9):1699-706. [Google Scholar]
[6]. CF Lanzieri, PM Duchesneau, SA Rosenbloom, AS Smith, AE Rosenbaum, The significance of asymmetry of the foramen of VesaliusAJNR Am J Neuroradiol 1988 9(6):1201-04. [Google Scholar]
[7]. N Gupta, A Yadav, Thomas RJ, A Shrivastava, Incidence of foramen Vesalius in adult human North Indian craniaJournal of Dental and Medical sciences 2014 13(5):34-38. [Google Scholar]
[8]. K Kodama, K Inoue, M Nagashima, G Matsumura, S Watanabe, G Kodama, Studies on the foramen Vesalius in the Japanese juvenile and adult skullsHokkaido Igaku Zasshi 1997 72(6):667-74. [Google Scholar]
[9]. N Gupta, B Ray, S Ghosh, Anatomic characteristics of foramen VesaliusKathmandu Univ Med J (KUMJ) 2005 3(2):155-58. [Google Scholar]
[10]. A Kale, F Aksu, A Ozturk, IA Gurses, O Gayretli, FG Zeybek, Foramen of VesaliusSaudi Med J 2009 30(1):56-59. [Google Scholar]
[11]. AL Shinohara, CG de Souza Melo, EM Silveira, JR Lauris, JC Andreo, A de Castro Rodrigues, Incidence, morphology and morphometry of the foramen of Vesalius: complementary study for a safer planning and execution of the trigeminal rhizotomy techniqueSurg Radiol Anat 2010 32(2):159-64. [Google Scholar]
[12]. AC Rossi, AR Freire, FB Prado, PH Caria, PR Botacin, Morphological characteristics of foramen of Vesalius and its relationship with clinical implicationsJ Morphol Sci 2010 27(1):26-29. [Google Scholar]
[13]. P Singh, C Raibagkar, Study of variation in atypical foramina of dry human skullNJIRM 2011 2(2):1-5. [Google Scholar]
[14]. V Chaisuksunt, L Kwathai, K Namonta, T Rungruang, W Apinhasmit, S Chompoopong, Occurrence of the foramen of Vesalius and its morphometry relevant to clinical considerationScientific World Journal 2012 :1-5. [Google Scholar]
[15]. H Shaik, M Shepur, S Desai, S Thomas, G Maavishettar, S Haseena, Study of Foramen Vesalius in South Indian skullsIndian Journal of Medicine and Healthcare 2012 1(1):22-24. [Google Scholar]
[16]. MA Ozer, F Govsa, Measurement accuracy of foramen of Vesalius for safe percutaneous techniques using computer-assisted three-dimensional landmarksSurg Radiol Anat 2014 36(2):147-54. [Google Scholar]
[17]. D Nirmala, N Hema, Study of emissary sphenoidal foramen and its clinical implicationsJournal of Evidence Based Medicine and Healthcare 2014 1(4):175-79. [Google Scholar]
[18]. P Srimani, P Mukherjee, M Sarkar, H Roy, SK Sengupta, AN Sarkar, Foramina in alisphenoid- Observational study on their osseomorphology and morphometryInternational journal of Anatomy, Radiology and Surgery 2014 3(1):1-6. [Google Scholar]