Cruciate Incision For Treatment of Primary/Recurrent Cases of Seroma/Hematoma of Pinna : A Novel Approach
Mahesh Bhat T1, Vinay V Rao2, David Rosario3
1Associate Professor, Department of Ear, Nose and Throat,Father Muller Medical College, Mangalore, India.
2Associate Professor, Department of Ear, Nose and Throat,Father Muller Medical College, Mangalore, India.
3Resident, Department of Ear, Nose and Throat,Father Muller Medical College, Mangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. David Rosario, Resident, Department of Ear, Nose and Throat, Father Muller Medical College, Kankanady, Mangalore-2, India.
E-mail: davidrosario84@gmail.com
Introduction: Seroma of pinna have a high predisposition for recurrence. Its surgical management requires excision of cartilage and perichondrium which can cause scarring, deformity of pinna, perichondritis and abscess formation, postoperatively.The aim of the current study is to the access the outcome of a novel approach using cruciate incision for surgical treatment of seroma/ hematoma of pinna.
Materials and Methods: Study was conducted at Father Muller Medical College in the Department of Otorhinolaryngology for a period of three months between January 2014 to March 2014 during which period 30 patients with seroma of the pinna were taken up for the study. Procedure was done under local anaesthesia with all aseptic precautions. A cruciate incision was given over the most dependent part of the swelling and flaps were raised. The collection was drained and the under surface of the flap was scraped using Rosen’s knife followed by pressure dressing for three days. Patients were followed up for three months.
Results: A total of 30 patients with seroma were studied. Out of the 30 cases 24 were primary cases and 6 were recurrent cases. Majority of the patients were in the age group 41-50 y. Out of 30 patients 18 were males and 12 were females. Out of 30 patients studied, none of them had recurrence. Four patients however developed perichondrial reaction with pain and inflammation which required analgesics and antibiotics. In 6 cases a thickening of the auricle at the site of incision was noticed which resolved over a period of 4 to 5 months. Overall cosmetic deformity was negligible with most of the patients showing a negligible scar after 6 months of follow up.
Conclusion: Cruciate incision is a good technique for treatment of seroma and hematoma of pinna as the outcome is good with no recurrence.
Hematoma auris, Perichondrium, Seroma
Introduction
Pseudocyst of auricle also called as auricular seroma ,is a cystic swelling filled with serous fluid. Aeitiology of seroma is not clearly known [1]. It can occur denovo or following surgery for ear or pinna or trauma of any sort to pinna [1,2]. Several methods have been advocated such as repeated aspiration, incision and drainage with pressure dressing, insertion of drainage tubes, excision and B.I.P.P. packing etc [3-5]. Excision and drainage which is considered the most accepted treatment modality, mainly consists of the window method where drainage of collection is done along with removal of a piece of cartilage and perichondrium [6].
The various treatment modalities available reflect on the fact that there is no single treatment which is totally satisfactory [6]. Successful treatment of seroma remains a challenge because this disease has a high propensity for recurrence. Also to be noted is that, excising the cartilage and perichondrium does have its effects in the form of scarring, deformity of pinna, chances of perichondritis and sometimes even an abscess formation [6].
The aim of this study was to the access the role of cruciate incision over the pinna through the cyst without excising the cartilage in cases of primary/recurrent seroma and studies the outcome in terms of recurrence, cosmetic outcome and chances of perichondritis/ abscess formation.
Materials and Methods
Study was conducted at Father Muller Medical College in the Department of Otorhinolaryngology for 3 months between January 2014 and March 2014 during which period 30 patients [Table/Fig-1] with seroma of the pinna were taken up for the study. These included clinically diagnosed cases of primary seroma as well as recurrent cases [Table/Fig-2] that were previously treated with other modalities like wide bore needle aspiration and window treatment.
Informed consent was taken and ethical clearance was obtained from concerned authorities.
Procedure was done under local anaesthesia with all aseptic precautions. The pinna was anaesthetised using 2% lignocaine 1:200,000 adrenaline. Infiltration was given along the post auricular groove in the region corresponding to the lobule of the ear and along the preauricular region. A total of 5cc of local anaesthetic was used to block the greater auricular nerve and auriculotemporal nerve. A cruciate incision [Table/Fig-3,Table/Fig-4]was given over the most dependent part of the swelling and flaps were raised. The collection was drained and the under surface of the flap was scraped using Rosen’s knife followed by pressure dressing for three days. Patients were followed up for three months. The outcome of this novel technique was studied in terms of recollection, recurrence, development of perichondritis/ abscess and cosmetic outcome.
Results
A total of 30 patients with seroma were studied. Out of the 30 cases 24 were primary cases and 6 were recurrent cases [Table/Fig-1] .Majority of the patients were in the age group 41-50. with 18 males and 12 females [Table/Fig-5] . None of them had recurrence.
Four patients however developed perichondrial reaction with pain and inflammation which required analgesics and antibiotics. In 6 cases a thickening of the auricle at the site of incision was noticed which resolved over a period of three months [Table/Fig-6] . Overall cosmetic deformity was negligible [Table/Fig-7] with most of the patients showing a negligible scar after three months of follow up.
Discussion
Seromas are rare, asymptomatic, cystic swellings of the pinna that result from an accumulation of sterile fluid within an unlined intracartilagenous space [1]. It is unilateral, asymptomatic, cystic swelling of the helix or antihelix, most often located in the scaphoid fossa. The auricular pseudocyst has a cavity that is not lined by epithelium [2]. The term pseudocyst of auricle was designated to these by Hartman in 1846 who first defined and made a study on seroma’s [7].This rare disorder results from spontaneous accumulation of sterile,oily yellowish fluid. Bacterial cultures are always negative [8]. A pseudocyst of the auricle is an intercartilaginous cystic swelling of the anterior auricle. The cause is uncertain, and most patients deny any history of inflammation or trauma [9].The condition is disturbing to both the patients because of its ugly appearance and the treating doctor in deciding the appropriate line of management which if unsatisfactory can lead to recurrences and at times deformity.
It is quite interesting that Hansen [10] and Engel in their studies on seromas found them only in males. In our study the ratio was 3:2 for male: female. Various treatments in literature include simple aspiration, intra-lesional injection of corticosteroids and aspiration in combination with bolstered dressing/sutures or plaster of paris cast [3-5].These methods are known to be associated with high rate of recurrence or thickening. Other more invasive techniques include incision and drainage of the cavity followed by obliteration by curettage, window procedure etc. The invasive techniques are known to be involved with risk of perichondritis, abscess formation, cauliflower deformity and may be followed by recurrences [6].
In studies done by Bage et al., [2], recurrence rate with aspiration and bandaging was 54.55% and for aspiration and injection technique was 17.95%, compared with this study our technique of cruciate incision showed no recurrence [Table/Fig-6] . In a study done by Bhandary et al., [6], 12% of patients showed perichondrial reaction,20% showed thickening of pinna and 4% showed deformity of the pinna who were treated with window procedure. Compared to this in our study, 8% showed perichondrial reaction, 12% showed thickening of the pinna which is much lesser when compared to the results of window procedure however none of our patients showed any recurrence or deformity [Table/Fig-6] .
| Primary cases | 24 |
| Recurrent cases | 6 |
| Total | 30 |
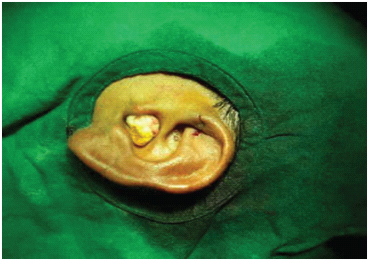
Preoperative photograph in a recurrent case showing scar from previous procedure

Incision site being marked


| Age group in years | Number of cases | Percentage |
|---|
| 11-20 | 1 | 3.33% |
| 21-30 | 3 | 10% |
| 31-40 | 7 | 23.33% |
| 41-50 | 14 | 46.66% |
| 51-60 | 5 | 16.66% |
| Sequelae/ Complication | Number |
|---|
| 1) Recurrence | ---- |
| 2) Perichondrial reaction | 4 |
| 3) Thickening of the pinna | 6 |
| 4) Cosmetic deformity | ---- |
Conclusion
There are several modalities available for the treatment of seroma’s of the pinna. However, most of these procedures are associated with sequel like recurrence, perichondrial reaction leading to perichondritis and abscess formation, thickening of pinna and cosmetic deformity. Our study with this novel technique showed no recurrence, no cosmetic deformity and negligible incidence of perichondritis and thickening making it one of the ideal methods for dealing with recurrent/primary seroma’s.
[1]. D Engel, Pseudocysts of the auricle in ChineseArchotolaryngol 1966 83(3):197-202. [Google Scholar]
[2]. Bage Pseudocyst of the auricleNational journal of clinical anatomy 2012 1(4):181-85. [Google Scholar]
[3]. Miyamoto Steroid injection therapy for pseudocyst of the auricleActa Derm Venereol 1994 74(2):140-42. [Google Scholar]
[4]. D Ophir, G Marshak, Needle aspiration and pressure sutures for auricular pseudocystPlast Reconotr Surg 1991 87:783-84. [Google Scholar]
[5]. KH Juan, Pseudocyst of the auricle: steroid therapyAuris Nasus Larynx 1994 21:8-12. [Google Scholar]
[6]. Bhandary Satheesh, Mannil Thomas Varghese, A comparative study in the management of auricular pseudocystsIndian Journal of Otolaryngology and Head and Neck Surgery 2000 52(3) [Google Scholar]
[7]. M Harder, C Zachary, Pseudocyst of the ear: surgical treatmentJ Dermatol Surg Oncol 1993 19:585-88. [Google Scholar]
[8]. S Ichiok, Pseudocyst of the auricle: case reports and its biochemical characteristicsAnn Plast Surg 1993 31:471-74. [Google Scholar]
[9]. WJ Grabski, SJ Salasche, ML McCollough, VL Angeloni, Pseudocyst of the auricle associated with traumaArch Dermatol 1989 25(4):528-30. [Google Scholar]
[10]. JE Hansen, Pseudocyst of the Auricle in CaucasiansArchives of Otolaryngology 1967 85:35-36. [Google Scholar]