Versatile but Temperamental: A Morphological Study of Palmaris Longus in the Cadaver
Asha Joselet Mathew1, Tintu Thottiyil Sukumaran2, Susan Joseph3
1Clinical Associate Professor, Department of Anatomy,Amrita School of Medicine, AIMS, Amrita Vishwa Vidyapeetham, Ponekara Kochi, Kerala, India.
2Lecturer, Department of Anatomy,Amrita School of Medicine, AIMS, Amrita Vishwa Vidyapeetham, Ponekara Kochi, Kerala, India.
3Lecturer, Department of Anatomy,Amrita School of Medicine, AIMS, Amrita Vishwa Vidyapeetham, Ponekara Kochi, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Asha Joselet Mathew, Clinical Associate Professor, Department of Anatomy, Amrita Institute of Medical Sciences, Ponekara, Kochi -682041, India.
E-mail: ashajmathew@aims.amrita.edu,ashajmathew@gmail.com
Introduction: Palmaris longus (PL) is one of the most variable muscles in our body and is vestigial functionally. Its long tendon and its superficial location make it an ideal source for tendon harvesting. Variations such as absence, duplication and reversal have far reaching clinical impact. The aim of this study is to estimate the presence, variants and nerve supply of the PL.
Materials and Methods: Upper extremity of 24 cadavers was dissected and PL was examined. The results were compared to other studies on the PL and literature survey was carried out.
Results: Thirty nine specimens showed normal morphology and four showed complete agenesis. Other morphological variations seen included - reversed, hybrid, fusiform, fleshy and bifurcated tendon of insertion.
Conclusion: Every surgeon must be aware of the variations of the versatile but temperamental PL. Prior knowledge of the layout of the muscle helps in planning intricate surgeries to which this tendon is put use to.
Agenesis, Accessory palmaris longus, Duplicated palmaris longus, Hybrid, Palmaris longus, Reversed palmaris longus, Tendon harvesting
Introduction
PL is a superficial, slender, fusiform muscle of the forearm acting as a weak wrist flexor in tandem with the other forearm flexor muscles. The proximal fleshy attachment is on the medial epicondyle, adjoining muscles, intermuscular septa and ante brachial fascia in common with the other superficial flexors. Distally a long tendon starts in the mid forearm and is inserted into the distal part of the flexor retinaculum and the palmar aponeurosis, frequently sending tendinous slips to the thenar muscles. It lies between the flexor carpi radialis and flexor carpi ulnaris and overlying the median nerve [1]. In evolutionary history it is seen to be prominent in mammals that use their forelimbs for ambulation and a well developed muscle is seen in the orangutan but is vestigial in humans. In predatory animals, it assists in claw retraction [2].
Numerous variations have been reported in both morphology and number [3]. It may have a proximal tendon or a distal tendon, or have a fleshy central belly with proximal and distal tendons, it maybe digastric or fleshy through out or its tendon may be split and sometimes it maybe degenerated to such an extent it that may be simply represented by a tendinous band [4]. When it is tendinous proximally and has a fleshly distal belly it is called reverse PL or PL inversus [5]. The aim of this study is to determine the presence and absence and morphological variations of PL, its impact on neighbouring nerves and more importantly its surgical significance.
Materials and Methods
Twenty years four male cadavers of South Indian origin in the age group 35-70 used for dissection for the first year medical students of Amrita School of Medicine, Amrita Institute of Medical Sciences, were studied serially during the years 2011-14. The flexor compartment of the forearm of the upper limb was dissected using standard procedure [6]. The presence, absence and morphological variations of PL, its nerve supply and its relation to flexor retinaculum and neighbouring structures were noted.
Results
Of the 48 limbs studied, 39 showed normal morphology. In four specimens there was complete agenesis. Other morphological variations seen include - reversed, hybrid, fusiform, fleshy and bifurcated tendon of insertion. All variants were unilateral. Their numbers, percentage and laterality are presented in [Table/Fig-1]. In all cases it was supplied by the median nerve.
Discussion
The normal PL [Table/Fig-2] is a superficial, slender, fusiform muscle of the forearm acting as a weak wrist flexor in tandem with the other forearm flexor muscles. The proximal fleshy attachment is on the medial epicondyle, adjoining muscles, intermuscular septa and ante brachial fascia in common with the other superficial flexors. Distally a long tendon starts in the mid forearm and is inserted into the distal part of the flexor retinaculum and the palmar aponeurosis, frequently sending tendinous slips to the thenar muscles. It lies between the flexor carpi radialis and flexor carpi ulnaris and overlying the median nerve.
Agenesis of PL [Table/Fig-3] are said to follow Mendelian principles, its absence is autosomal dominant and its presence is autosomal recessive [7]. In Caucasians the prevelance of agenesis ranges between 16-25% and in Mongloids as low as 4% and in Indians 17%. The universally accepted average is 10% [8,9]. In the present study agenesis of 8.35% was noted. This emphasises the theory of ethnic variations. The prevalence of agenesis of the PL has been extensively studied following the first report of its absence in 1559 by Colombo in De Re Anatomica Libri [10]. Some authors suggested that apart from its ethnic variations, its absence is more common in women, bilateral absence being more common, and that unilateral absence occurs more frequently on the left side [3,5]. In our study we have considered side but not considered gender parameters as the cadavers were all male.
In our study the reverse PL [Table/Fig-4] took a tendinous origin from the medial epicondyle, the muscle belly was seen in the lower two third and it attached distally to flexor retinaculum and pisiform and fused with the ante- brachial fascia in this region. Reverse PL was first described by Captain John T. Morrison as an incidental post amputation finding [11]. It may cause compartment syndrome in the Carpal tunnel and Guyon’s canal. The patient will present with pain and edema in the wrist region. This is an occupational hazard in people whose work involves repetitive wrist movements as it will result in hypertrophy and cause compression of median nerve and or ulnar nerve. This makes the modern day computer professionals particularly vulnerable. Symptomatic patients presenting with a palpable volar swelling should be examined for variations in the PL. In an asymptomatic subject a hypertrophied muscle will obstruct and result in hazy interpretation of radiological assessment of this region. Difficulties in endoscopic procedure and electro myographic studies may also result from such a reversal [12].
The accessory PL [Table/Fig-5] may also cause compression of either the median nerve or ulnar nerve. The forearm muscles develops from a single precursor mass which divides into superficial component giving rise to the pronator teres, flexor carpi radialis, flexor carpi ulnaris and the PL. The deep component gives rise to the deep flexors of the forearm. The additional belly can be embryologically explained on the basis of additional cleavage of the superficial mass [13]. The term duplicated should be reserved for cases in which there is a completely separate muscle belly that does not share the common origin with the ‘normal’ appearing PL. The palmaris profundus qualifies as true duplicated and it may exist in addition to the normal PL muscle [14] or as a lone entity in place of the normal PL muscle [15]. Palmaris profundus was first described by Frohse and Fraenkel [16] and has been sometimes called musculus comitans nervi mediani because the tendon of palmaris profundus and the median nerve are often invested in a common sheath of connective tissue. Arising from the lateral edge of the radius, it lies lateral to the flexor digitorum superficialis and deep to pronator teres and its tendon of insertion passes dorsal to the flexor retinaculum to which it attaches [17]. In our study the additional muscle appears to have a hybrid disposition. Its origin follows the principle of accessory type in common with the normal PL. Its insertion on the contrary is unique, forming a triangular flattened miniature aponeurosis, which passed dorsal to the palmar aponeurosis. This aponeurosis appears to be a duplication of the palmar aponeurosis. To our knowledge such a variant has not been documented in any literature survey.
A fleshy [Table/Fig-6] was seen in only one out of 48 specimens. It was broad, fleshy and bipennate in its upper half while in the distal third the muscle appeared unipennate with fibers fanning out from its radial side all the way to its insertion. In this variation compression of both ulnar and median nerves in the forearm can result and a source of tendon is lost.
A fusiform type of PL [Table/Fig-7] was noted. The belly occupied the central one-third and it originated and inserted by means of thin tendons in the upper and lower third respectively. This type deprives the subject of a source of a lengthy tendon.
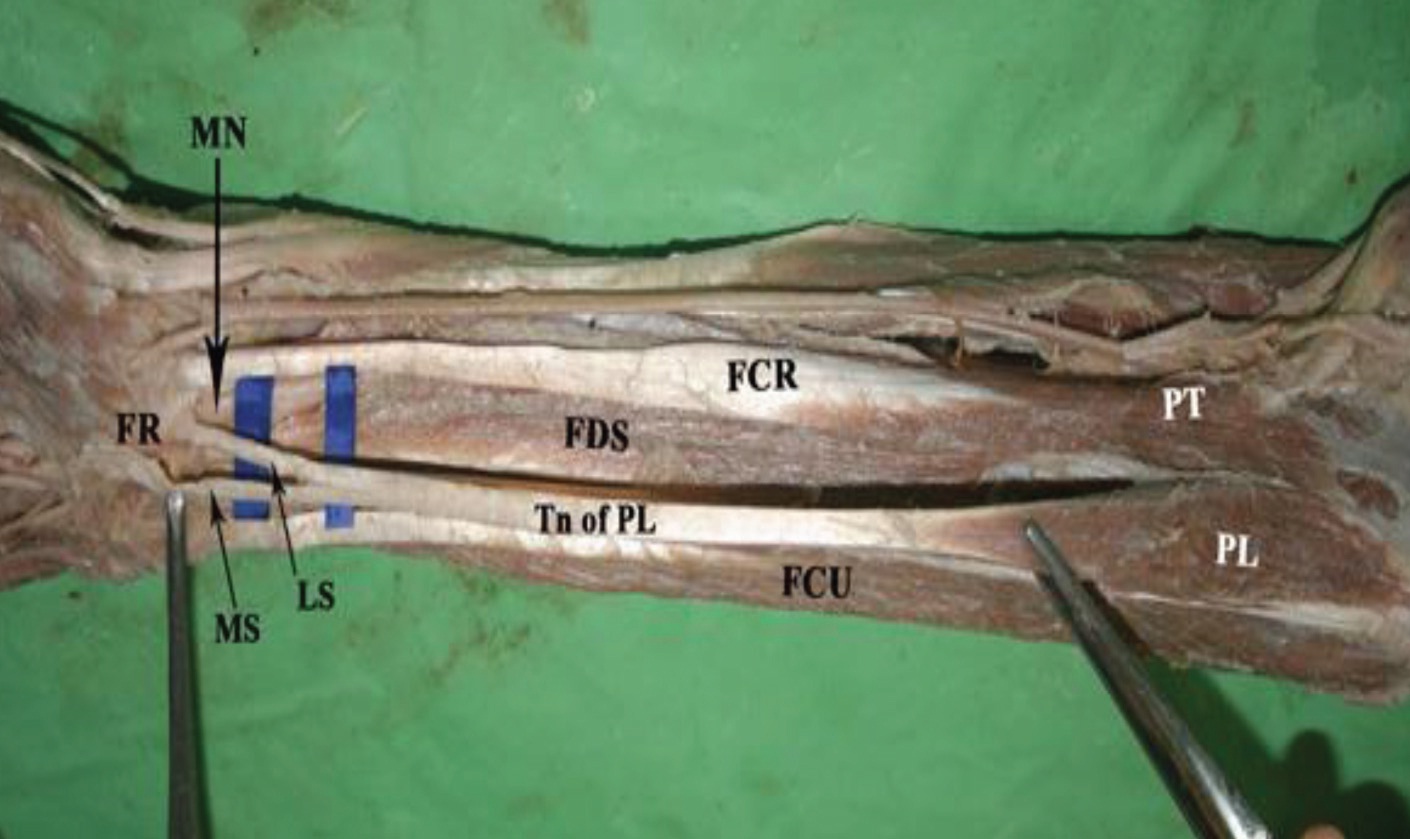
In one of our specimens the origin was the classical type. Its insertion was tendinous but split into medial and lateral divisions [Table/Fig-8]. The superficial medial slip was in continuity with the palmar aponeurosis and the deeper lateral slip passed deep to the flexor retinaculum along with median nerve. The variations at its insertion become important because of the proximity to median and ulnar nerves. The advantage of V-shaped split tendinous insertion is that it can be put to use for lip augmentation [18] as well as in oculoplasty [19].
Types of palmaris longus its laterality and incidence
| Morphology | Side | Number | Percentage |
|---|
| Right | Left |
|---|
| Normal | 20 | 19 | 39 | 81.25 |
| Agenesis | 2 | 2 | 4 | 8.35 |
| Reversed | - | 1 | 1 | 2.08 |
| Hybrid | - | 1 | 1 | 2.08 |
| Fusiform | 1 | - | 1 | 2.08 |
| Fleshy | - | 1 | 1 | 2.08 |
| Bifurcated tendon | 1 | - | 1 | 2.08 |
Normal palmaris longus (NPL) (Left side); with relation to median nerve (MN); also seen are pronator teres (PT); flexor carpi ulnaris (FCU); flexor carpi radialis (FCR); flexor digitorum superficialis (FDS), and flexor retinaculum (FR) seen

Agenesis of palmaris longus (Right side); pronator teres (PT); flexor carpi ulnaris (FCU); flexor carpi radialis (FCR) and flexor digitorum superficialis (FDS) seen along with median nerve (MN) flexor retinaculum (FR) and ulnar nerve and vessels (UNV)

Reversed palmaris longus (R-PL) (Left side); proximal tendon of reversed palmaris longus (Tn.R-PL); pronator teres (PT); flexor carpi ulnaris (FCU); flexor carpi radialis (FCR); flexor digitorum superficialis (FDS); flexor retinaculum(FR) median nerve (MN) and ulnar nerve (UN) seen.

Normal palmaris longus (NPL) (Left side); Hybrid palmaris longus (H-PL); Palmar Aponeurosis (PA); Duplicated Palmar Aponeurosis (DPA); pronator teres (PT); flexor carpi radialis (FCR); flexor digitorum superficialis (FDS); flexor carpi ulnaris (FCU); median nerve (MN) seen.

Fleshy palmaris longus (F-PL) (Left side); Lower unipennate portion on the radial side of the tendon ( shown by black arrow ) ; pronator teres (PT); flexor carpi radialis (FCR); flexor digitorum superficialis (FDS); flexor carpi ulnaris (FCU) and flexor retinaculum (FR) seen.

Fusiform palmaris longus (Fm-PL) (Right side); distal tendon of palmaris longus (D.Tn); proximal tendon of palmaris longus (P.Tn); pronator teres (PT); flexor digitorum superficialis (FDS); flexor carpi radialis (FCR); flexor carpi ulnaris (FCU); median nerve (MN) and palmar aponeurosis (PA) seen

Palmaris longus (PL) (Right side); tendon of palmaris longus (Tn. of PL) medial slip (MS) and lateral slip (LS); pronator teres (PT); flexor carpi ulnaris (FCU); flexor carpi radialis (FCR); flexor digitorum superficialis (FDS); flexor retinaculum (FR) and median nerve (MN) seen
Conclusion
PL though morphological and functionally insignificant is harvested for various reconstructive surgeries such as tendon graft, tendon transfer, nerve palsies and ptosis repair and cosmetic procedures such as lip augmentation. It is ideal as its removal produces no functional impairment. It is easily accessible because of its superficial location, and its length and breadth are perfectly suited for repairs.
Every surgeon must be aware of the variations of the versatile but temperamental palmaris longus. Prior knowledge of the layout of the muscle helps in planning intricate surgeries to which this tendon is put use to.
[1]. Standring Susan, Anatomy Grays, The Anatomical Basis of Clinical Practice 2005 39th EditionLondonElsevier Churchill Livingstone:876-77. [Google Scholar]
[2]. DK Sharma, CK Shukla, V Sharma, Clinical assessment of absence of palmaris longus and its association with gender, body sides, handedness and other anomalies in population of Central IndiaJ Anat Soc India 2012 66(1):13-20. [Google Scholar]
[3]. SR Nayak, A Krishnamurthy, AR Lakshmi, L Prabhu, GC Kumar, KT Dinit, Multiple muscular anomalies of upper extremity: A cadaveric studyRom J Morphol Embryol 2008 49(3):411-15. [Google Scholar]
[4]. N Mobin, G Saraswati, Anatomical variations of palmaris longusAnatomica Karnataka 2010 4(2):74-77. [Google Scholar]
[5]. JM Cope, EM Looney, CA Craig, R Gawron, R Lampros, R Mahoney, Median nerve compression and reverse palmaris longusInt J Anat Var 2009 2:102-04. [Google Scholar]
[6]. GJ Romanes, Cunninghams Manual of Practical Anatomy 2011 4115th EditionIndiaOxford Medical Publications:74-75. [Google Scholar]
[7]. FH Michel, EF Shaw, Anatomical variations of the palmaris longus causing carpal tunnel syndromeJ Plastic and Reconstructive Surgery 1978 62:798-800. [Google Scholar]
[8]. F Troha, GK Baibak, JC Keeleher, Frequency of palmaris longus in North American CaucasiansAnn Plast Surg 1990 26(6):477-78. [Google Scholar]
[9]. NW Thomson, BJ Mockford, GW Cran, Absence of the palmaris longus: A population studyUlster Med J 2001 70(1):22-24. [Google Scholar]
[10]. Realdi Columni Cremonensis.De Re Anatomica Libri.Venice: ex typographia N. Beuilacquae 1559 [Google Scholar]
[11]. JT Morrison, A palmaris longus muscle with a reversed belly, forming an accessory flexor muscle of the little fingerJ Anat Physiol 1916 50:324-26. [Google Scholar]
[12]. VPS Fazan, Reversed palmaris longus and median nerve relationship. Case report and literature reviewBraz J Morphol Sci. 2007 24(2):88-91. [Google Scholar]
[13]. WH Holinshed, Anatomy for surgeonsTetracyclineTeratology 1964 32nd EditionNew YorkHarper and Row:412 [Google Scholar]
[14]. DP Jones, Bilateral palmaris profundus in association with bifid median nerve as a cause of failed carpal tunnel releaseJ Hand Surg Am 2006 31(5):741-43. [Google Scholar]
[15]. MF Fatah, Palmaris profundus of Frohse and Frankel in association with carpal tunnel syndromeJ Hand Surg Br 1984 9(2):142-44. [Google Scholar]
[16]. F Frohse, M Frankel, Die Muskeln des menschlichen Armes 1908 [Google Scholar]
[17]. RA Bergman, SA Thompson, AK Afifi, FA Saadeh, Compendium of human anatomical variation: text, atlas and world literatureBaltimore, Urban and Schwarzenberg 1988 41:282-88. [Google Scholar]
[18]. BA Davidson, Lip augmentation using the palmaris longus tendonPlast Reconstr Surg 1995 95:1108-10. [Google Scholar]
[19]. K Kurihara, T Kojima, E Marumo, Frontalis suspension for blepharoptosis using palmaris longus tendonAnn Plast Surg 1984 13:274-78. [Google Scholar]