Postpartum Acute Pulmonary Oedema with Sub clinical Rheumatic Heart Disease
Padmaja R1, Sri Krishna Padma Challa Rao. Gande2
1Assistant Professor, Department of Aanaesthesia,Konaseema institute of Medical Sciences, Amalapuram, Andhra Pradesh, India.
2Consultant Physician, Deartment of General Medicine,Konaseema institute of Medical Sciences, Amalapuram, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Padmaja R, D. No 65-8-5/1, G P T Road, Mehernagar, Kakinada, EGDT, Andhra Pradesh, India. E-mail : padmajaanes@gmail.com
Acute dyspnea with pulmonary oedema in postpartum is uncommon but life-threatening event. Contributing factors for pulmonary oedema include, administration of tocolytics, underlying cardiac disease, iatrogenic fluid overload and preeclampsia acounting 0.08% of pregnancies. Pulmonary embolism, amniotic fluid embolism, pneumonia, aspiration and pulmonary oedema are some of the potentially devastating conditions that should be considered by the attending physician.
Here, we report a case of postpartum acute pulmonary oedema referred to causality after an emergency caesarean section in a private hospital. No matter what the underlying pathology, prompt administration and appropriate resuscitation is always the first priority. Only after the patient has been stabilized attention must be turned to diagnosis and specific treatment. A diagnosis of severe Mitral Stenosis, probably of rheumatic origin was made after stabilizing the patient.
Mitral stenosis, Pulmonary oedema, Sub clinical carditis
Case Report
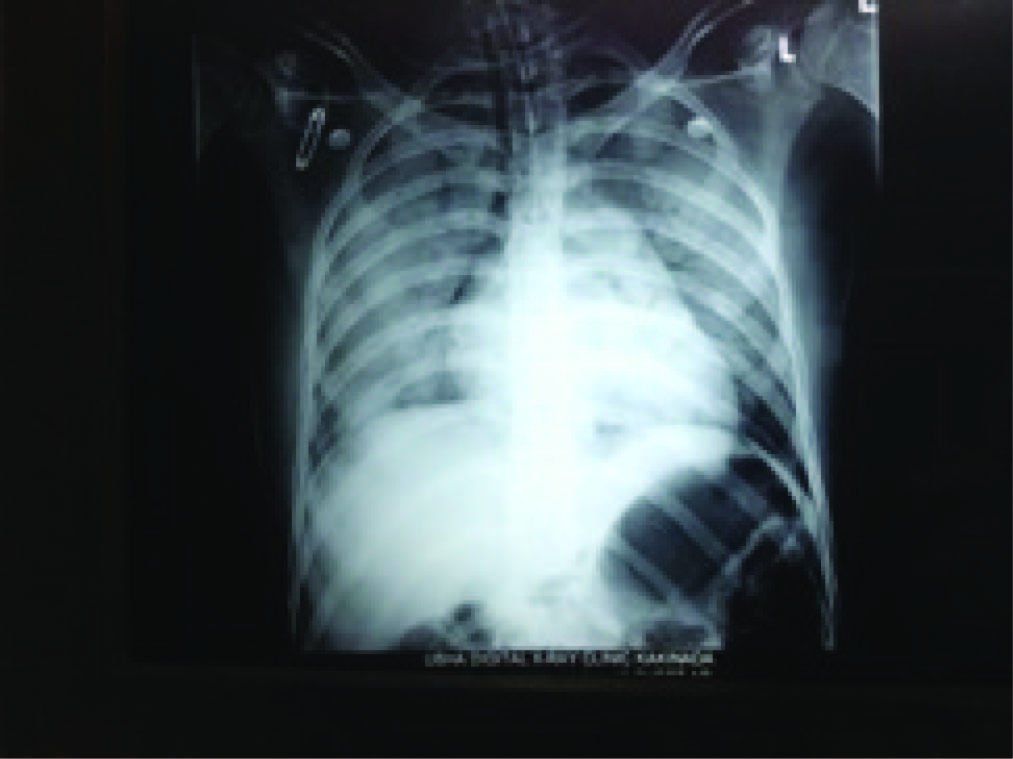
A 22-year-old patient was referred to Konaseema institute of medical sciences at casuality, with severe respiratory distress. She had undergone an emergency caesarean section under spinal anaesthesia for premature rupture of membranes, 12 h before admission in a local hospital. She had marked respiratory distress so referred to tertiary care hospital, at the time of admission with oxygen saturation of 49% on room air. Her pulse was 170/min on monitor, low volume on palpation, systolic blood pressure was recorded as 70 mmHg. Clinical examination of lungs showed bilateral coarse crepitations. Hence she was kept on Synchronized Intermittent Mandatory Ventilation(SIMV Mode) mode of mechanical ventilation and dobutamine and nor adernaline to support circulation. Electrocardiography showed sinus tachycardia and chest X-ray showed bilateral infiltrates [Table/Fig-1] by which tentative diagnosis of pulmonary oedema was made.
To evaluate the cause of pulmonary oedema a review of all the medications she had received and total fluids administered was done. History showed that she had regular antenatal check up and the antenatal history was insignificant.
She was subjected to echocardiogram which revealed severe Mitral stenosis with mild mitral regurgitation and severe Pulmonary artery hypertension (PASP i.e. pulmonary artery systolic pressure is 67mmHg). History was again reviewed but she had no history of rheumatic fever or any cardiac symptoms.
She was extubated on day four and discharged on day nine. She was advised to visit a cardiologist in view of her valvular heart disease at time of discharge.
Discussion
Significant shortness of breath, tachypnea, rhonchi on auscultation, evidence of hypoxia by pulse oximetry and arterial blood gas, pink frothy fluid through endotracheal tube and chest X-ray finding are consistent with pulmonary oedema. The percentage of pregnancies that are complicated by acute pulmonary oedema has been estimated to be 0.08% which is in correlation with previous studies [1,2].The most common contributing factors include the administration of tocolytic agents, underlying cardiac disease, iatrogenic fluid overload and preeclampsia.
Careful review of patient medication chart excluded tocolytic therapy and iatrogenic fluid overload in our case. Echocardiography revealed a clinically unexpected finding of mitral valve stenosis. Rheumatic fever is the leading cause of mitral valve stenosis [3-5], but our patient had no history of rheumatic fever. Only 50 to 70% of patients give a history of rheumatic fever which may be because such patients may have suffered from subclinical rheumatic fever not associated with polyarthritis [6]. The absence of a history of rheumatic fever in a patient does not precludes the presence of rheumatic heart disease correlates with Yazici HU et al., [7].
Atrial fibrillation is a common complication of Mitral valve stenosis [6] and affects 40% of cases of mitral stenosis [5]. Atrial fibrillation is due to increasing left atrial size and left atrial hypertension [8]. Although our patient had left atrial dilatation (4.8 cm), she had no atrial fibrillation.
Our patient was asymptamatic in the entire antenatal period and the intraoperative period. The sudden rise in venous return due to autotransfusion leads to pulmonary oedema in a parturient with significant mitral stenosis which was also seen in our patient [9].
A significant number of patients with suspected rheumatic carditis have no clinical murmurs [10]. The reported prevalence
of subclinical carditis in rheumatic fever ranges from 0 to 53%. Echocardiography is more sensitive and more accurate in diagnosing valvular involvement in acute rheumatic fever [11,12]. A recent echocardiographic screening survey from India has also suggested a very high prevalence rate (52.4/1000 school children) [13]. One-third of these patients develop chronic valvular heart disease. Occurrence of valvular heart disease in acute rheumatic fever without evident carditis is observed as study done by Folger GM et al., [14].
We believe that Doppler echocardiography should be done to suspected pregnant patient to detect subclinical valvular heart disease and to prevent untoward complications during perioperative period. Hand-held and mobile forms of echocardiography should be made available in remote areas of the world.
The chest X-ray showing bilateral infiltrates
Conclusion
Mitral stenosis of rheumatic origin is most likely missed and underreported because of lack of diagnostic modalities such as echocardiography. Its prevalence is higher than expected and provides a challenge to anaesthesiologist, when it is clinically unrecognised and present with complications like pulmonary oedema during perioperative period.
[1]. C Sciscione Anthony, Thomas Ivester, Marissa Largoza, James Manley, Philip Shlossman, HC Colmorgen Garrett, Acute Pulmonary Oedema in pregnancyObstetrics and Gynaecology 2003 101(3):511-15. [Google Scholar]
[2]. khan Masuda Islam, Acute postpartum pulmonary oedema in a 32-yearold woman five days after caesarean deliveryJournal of Enam Medical College 2013 3(2):113-16. [Google Scholar]
[3]. P Nordet, WHO/ISFC. Global programme for the prevention and control of RF/RHDJ In Fed Cardiol 1993 3:4-5. [Google Scholar]
[4]. MJ Eisenberg, Rheumatic heart disease in the developing world: prevalence, prevention and controlEur Heart J 1993 14:122-28. [Google Scholar]
[5]. C Conradie, R Schall, JD Marx, Echocardiographic study of left atrial thrombus in mitral stenosis Clin Cardiol 1995 16:729-31. [Google Scholar]
[6]. A Selzer, KE Cohn, Natural history of mitral stenosis: a reviewCirculation 1972 45:878-90. [Google Scholar]
[7]. HU Yazici, B Akcay, U Ozturk, A Tassal, A giant left atriumTürk Kardiyol Dern Ars 2010 38:223 [Google Scholar]
[8]. AR Rick, JE Gregory, Experimental evidence that lesions with basic charecteristics of rheumatic carditis can result from anaphylactic hypersensitivityBull johns Hopkins hospital 1993 73:239 [Google Scholar]
[9]. Salmasi Abdul-Majeed, Dancy Mark, Unrecognised mitral valve stenosis in a London multi-ethnic communityBr J Cardiol 2011 18:138-41. [Google Scholar]
[10]. M Tubridy-Clark, JR Carapetis, Subclinical carditis in rheumatic fever . A systematic reviewInt J Cardiol 2007 119:54-58. [Google Scholar]
[11]. M Bhaya, RB Panwar, R Beniwal, S Panwar, Echocardiographic evidence of significant regurgitation can be the sole criterion for diagnosis of probable rheumatic heart disease. Experience from a large cross-sectional surveyJ Am Coll Cardiol 2009 53:A409 [Google Scholar]
[12]. IB Vijayalakshmi, The role of echocardiography in diagnosing carditis in the setting of acute rheumatic feverCardiol Young 2005 15:583-88. [Google Scholar]
[13]. WHO Technical Report, Series. Rheumatic fever and rheumatic heart disease: Report of a WHO expert panel 2004 [Google Scholar]
[14]. GM Folger, R Hajar, A Robida, HA Hajar, Occurrence of valvular heart disease in acute rheumatic fever without evident carditis. Colour-flow Doppler identificationBr Heart J 1992 67:434-38. [Google Scholar]