Recurrent Mandibular Supplemental Premolars: A Case Report with 5 Year Follow Up and Review of Literature
S.V.S.G. Nirmala1, Sandeep Chilamakuri2, Ramasubba Reddy Challa3, Sivakumar Nuvvula4, Neeraj Gokhale5
1 Professor, Department of Paedodontics & Preventive Dentistry, Narayana Dental College & Hospital, Nellore, Andhra Pradesh, India.
2 Post Graduate Student, Department of Paedodontics & Preventive Dentistry, Narayana Dental College & Hospital, Nellore , Andhra Pradesh, India.
3 Senior Lecturer, Department of Paedodontics & Preventive Dentistry, Narayana Dental College & Hospital, Nellore, Andhra Pradesh, India.
4 Professor & Head, Department of Paedodontics & Preventive Dentistry, Narayana Dental College & Hospital, Nellore, Andhra Pradesh, India.
5 Lecturer, Department of Pedodontics and Preventive Dentistry, KLE V.K Institute of Dental sciences, Nehru nagar, Belgaum, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S.V.S.G. Nirmala, Professor, Department of Paedodontics & Preventive Dentistry, Narayana Dental College & Hospital, Nellore - 524003, Andhra Pradesh, India.
E-mail: nimskrishna2007@gmail.com
A 12-year-old girl reported for a routine dental checkup. Radiographic survey disclosed the presence of two developing structures resembling premolars one on either side of the mandible in premolar region, which were of supplemental type and surgical removal of supernumerary premolars facilitated eruption of the left second premolar. On six months follow-up, there was radiographic evidence of another supernumerary premolar in the left side of mandible that is left in situ, patient is on regular follow-up. This emphasizes the importance of thorough clinical and radiographic examination, early diagnosis and follow-up of the developing dentition in children. The patient has been followed-up from the age of 12 year to 17 year. This paper describes a case of recurrent supplemental supernumerary premolars in the mandible along with review of literature.
Delayed formation, Failure of eruption, Mandibular supernumeraries, Recurrent supplemental premolars
Case Report
A 12-year-old girl reported for a routine dental checkup to the Department of Paediatric Dentistry in September 2007. Her family and medical history were not relevant. General and extra oral examination did not show any abnormalities. Intraoral examination revealed mixed dentition with Angle’s class I molar relationship.
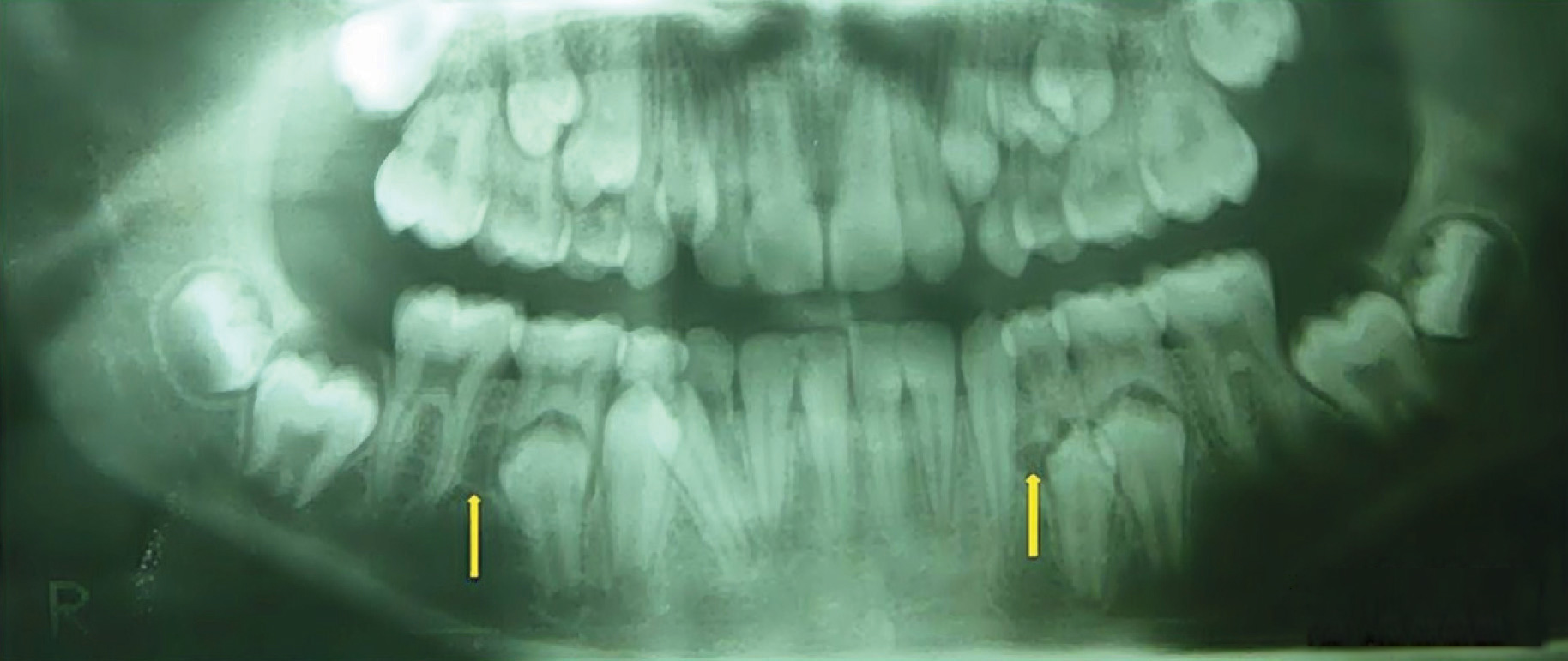
The patient had good oral hygiene and retained primary molars in all four quadrants. Orthopantomograph (OPG) disclosed the presence of two developing tooth like structures one on either side of the mandible; on the left side it was located between permanent canine and the mesial root of mandibular primary first molar whereas on the right side a crypt was found between the distal root of primary second molar and mesial root of first permanent molar [Table/Fig-1]. The patient and her mother were informed about them and counseled accordingly.
Orthopantomograph (OPG) at age 12 with calcified structure between 33 & 74 and presence of crypt between 46 & 85
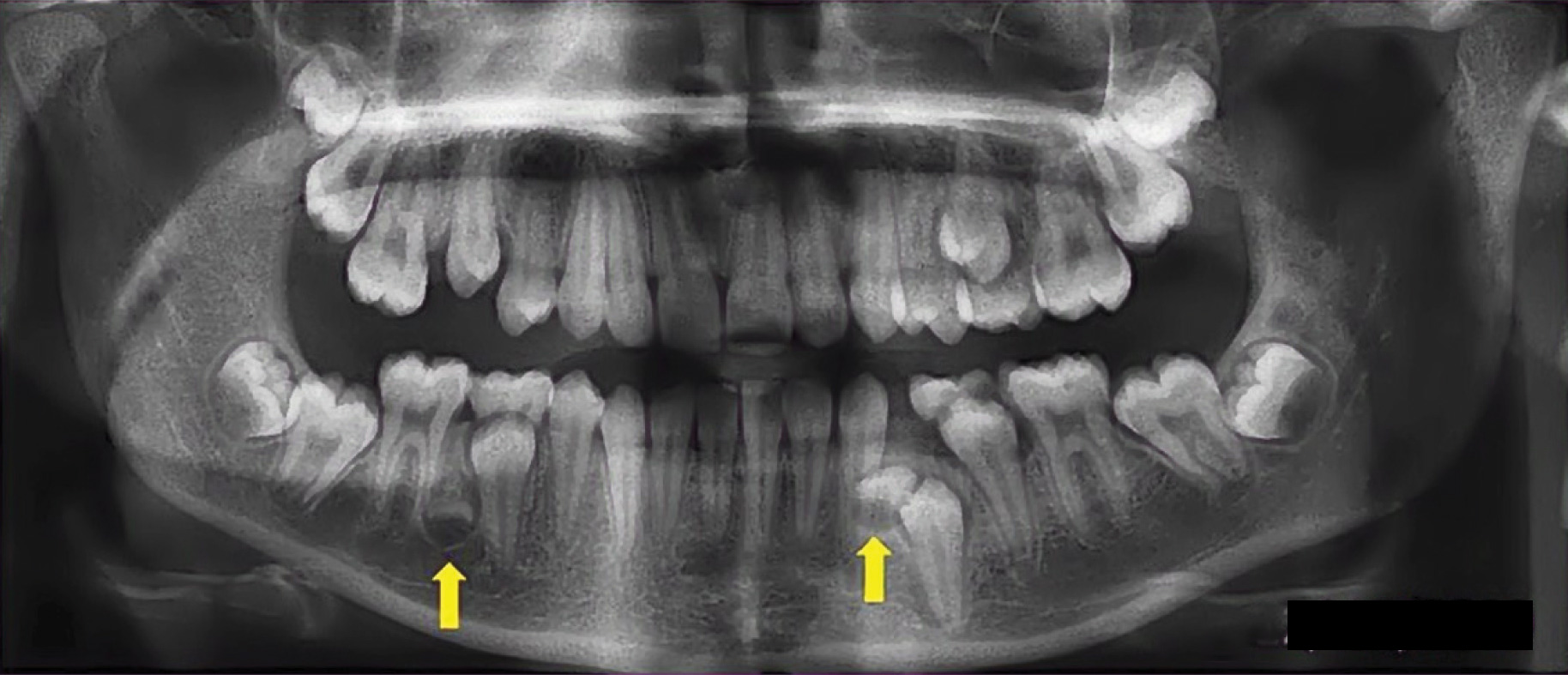
One and half year later in February 2009, the patient returned with a complaint of unerupted posterior teeth in the left lower side of the jaw. The patient was in mixed dentition stage, with retained left mandibular first primary molar [Table/Fig-2]. At this stage, OPG revealed two distinct calcified structures resembling crowns of mandibular premolars. On the left side of the mandible the developing supplemental premolar was present between the first premolar and canine region which was not only hampering the eruption of the first premolar but also was in close proximity to the root of permanent canine. On the right side, it was located in between the second premolar and the first permanent molar [Table/Fig-2]. A decision was made to keep the right sided supplemental premolar under observation after weighing the risk to benefit ratio as the tooth bud was not sufficiently calcified, the removal of which could cause damage to the root of the first permanent molar. After routine hematological investigations, surgical removal of supplemental premolar on the left side was carried out [Table/Fig-3]. After an 8 months interval, in November 2010 surgical extraction of supernumerary premolar was performed on the right side [Table/Fig-4]. The postoperative period remained uneventful.
OPG at age 14 with supplemental premolars between 33 & 34 and 45 & 46
Surgical exposure of the supplemental premolar on the left side of mandible; Enucleated supplemental tooth bud on left side of the mandible

Surgical exposure of the supplemental premolar on the right side of the mandible; Enucleated supplemental tooth bud on right side of the mandible

Six months later in May 2011, on examination premolar on the left side had erupted to the satisfaction of the patient [Table/Fig-5]. Subsequent OPG taken in December 2013 at 17 years of age showed all permanent teeth as well as early crown formation of another supernumerary tooth between the lower left first permanent molar and second premolar [Table/Fig-6]. It was decided to periodically observe this recurrent supplemental tooth and radiographically review the patient for further treatment.
Intra-oral picture showing erupted premolars on either side of the mandible

OPG of the patient at age 17, showing recurrent supernumerary premolar between 45 & 46

Discussion
Supernumerary teeth are described as those in excess when compared to the normal dental formula [1]. The incidence of super-numerary premolars is reported to be 1 in 10,000 individuals [2]. Grahnen reported that mandibular premolar supernumeraries occur in 0.29% of the general population. They have been reported to represent 6.6 to 14% of all supernumeraries [3].
Single supernumerary premolar may occur in 76-86% of cases, double supernumeraries in 12-23% of cases and multiple super-numeraries in less than 1% of cases [1] and the present case showed three supernumerary teeth.
Cases of late developing supernumerary teeth have been reported scarcely in the literature [2,3]. Among 48,550 subjects, supplemental premolars were present in 10% of cases with 79% in mandible and the findings of present case were in accordance with the reported literature. They may develop approximately 7-12 year after normal development [2].
The exact etiology of hyperdontia is obscure and they may form from independent, locally conditioned hyperactivity of the dental lamina [4]. The supplemental form would come from the lingual extensions of the accessory tooth bud, whereas the rudimentary form would be derived from proliferation of the epithelial remnants of the dental lamina induced by dentition pressure which was most widely accepted [5].
Parry [6] reported only one case of a supernumerary mandibular premolar (0.05%) among 2000 patients aged 16-26 year. The present case is in accordance with the radiographic evidence of late forming mandibular supernumerary premolar [7]. The majority of supplemental teeth in the permanent dentition develop later than the norm for teeth in that particular area.
It is difficult to determine exactly when a supernumerary premolar starts to form because of its lingual position which makes detection difficult on routine radiographs. Scott stated that the calcification of premolar teeth commences between 1.5 year and 2.5 year of age, although there may be no radiographic evidence of this until 3 or 4 year. But, it has been reported that supplemental premolars develop approximately 7 to 11 year after normal tooth development. The time of initial supplemental premolar mineralization could be determined within two years [8].
In the present case the supplemental teeth were detected on sequential conventional radiographs. But, they may not provide adequate information regarding the three dimensional relation of tooth to the adjacent structures. Hence, Computed Tomography (CT) can be used to provide more useful information than conventional radiographs to evaluate the root relationships of supernumerary teeth to the permanent teeth [9].
According to Primosch [10], the supernumerary teeth in our case resembled supplemental teeth. The frequent complications associated with the presence of supernumerary premolars are delayed eruption of permanent teeth, root resorption of adjacent teeth and dentigerous cyst [11]. In the present case, supplemental premolar hindered the eruption of lower left first premolar. In addition, several studies have reported the recurrence of supernumerary premolars after surgical removal. A possible mechanism for recurrence is that the crypts of additional supernumerary premolars were present earlier, but were not detected in the original radiographs [12].
Whenever a supernumerary tooth is diagnosed, the long term possibility of the progressive and delayed appearance of further supernumeraries should be considered. However, as these cases are uncommon, no guidelines for follow up have been developed. An appropriate time to carry out an OPG may be between the age of 16 y and 18 year, coinciding with the examination of the third molar.
In subsequent follow-up visits, surgical removal of supplemental premolars in mandible may be associated with recurrent tooth formation. A review of cases exhibiting this characteristic recurrence have been detailed in [Table/Fig-7].
Characteristics of cases presented with recurrent supplemental premolars in chronological order
| S. No | Author(s) | Year | Country | Gender | Age | No. of cases | Total teeth | Maxilla | Mandible | No of Extracted teeth | Follow up Period (Years) | Recurrent supplemental Teeth |
|---|
| Right | Left | Right | Left | Maxilla | Mandible | | Maxilla | Mandible |
|---|
| 1 | Poyton | 1960 | Canada | F | 11 | 1 | 8 | | 2 | 2 | 4 | - | 3 | 5 | - | 3 |
| 2 | Stevenson and Mc Kechnie | 1964 | Scotland | M | 12 | 1 | 8 | 3 | 2 | 2 | 1 | 1 | 2 | - | - | 3 |
| 3 | Shapira and Haskell | 1981 | USA | F | 12 | 1 | 4 | - | - | 2 | 2 | - | 2 | 1 | - | 1 |
| 4 | Rubenstein | 1991 | Richmond | F | 13 | 1 | 4 | 3 | 3 | 2 | 1 | 1 |
| 5 | Anegundi and Tavargeri | 2008 | India | M | 14 | 1 | 9 | 2 | 2 | 2 | 1 | 4 | 3 | 4 | 2 | - |
| PRESENT CASE |
| 6 | Case | 2014 | India | F | 12 | 1 | 3 | - | - | 1 | 2 | - | 2 | 5 | - | 1 |
In general, extraction of supernumerary premolars is the recommended treatment of choice but the time of surgical removal is controversial. If supernumerary teeth are close to the inferior alveolar nerve, increasing the risk of surgery, the teeth should be left in situ and monitored clinically and radiographically. King, Lee [13] reported that supernumerary premolars should be left in situ until further development which allows for uncomplicated surgery with less damage to roots and adjacent structures. Therefore, it was decided to observe and to review the patient after the third supernumerary tooth was detected.
When dealing with unerupted supernumerary teeth, we should understand that each case must be thoroughly planned with a multidisciplinary team (Paediatric Dentist, Orthodontist and Oral Surgeon) and the decision should be made whether to go for extraction or wait and watch. Evaluative monitoring should be done from this interdisciplinary point of view.
Conclusion
From a clinical standpoint, the early detection of supernumerary premolars is essential to prevent onset of complications in children. Although, the occurrence of recurrent supplemental premolars is relatively infrequent, they should be followed up routinely. However, due to their clinically unapparent development, an OPG during mixed dentition is indispensable.
[1]. Rajab LD, Hamdan MA, Supernumerary teeth: review of the literature and a survey of 152 casesInt J Paediatr Dent 2002 12:244-54. [Google Scholar]
[2]. Kantor ML, Bailey CS, Burkes EJ, Jr, Duplication of the premolar dentitionOral Surg Oral Med Oral Pathol 1988 66:62-64. [Google Scholar]
[3]. Grahnen H, Lindahl B, Supernumerary teeth in the permanent dentition: a frequency studyOdontol Revy 1961 12:290-94. [Google Scholar]
[4]. Biase DD, Midline supernumerary teeth in Huston, Texas school childrenJ Dent for children 1969 24:98-105. [Google Scholar]
[5]. Kassai Y, Munne P, Hotta Y, Regulation of mammalian tooth cusp patterning by ectodinScience 2005 309:2067-70. [Google Scholar]
[6]. Parry RR VI, Supernumerary teeth amongst orthodontic patients in IndiaBr Dent J 1961 111:257-58. [Google Scholar]
[7]. McNamara CM, Foley TF, Wright GZ, Sandy JR, The management of premolar supernumeraries in three orthodontic casesJ Clin Pediatr Dent 1997 22:15-18. [Google Scholar]
[8]. Scott NS, Introduction to Dental Anatomy 1967 5 edLondonChurchill Livingstone [Google Scholar]
[9]. Kawashita Y, Saito T, Nonsyndromic multiple mandibular supernumerary pre-molars: a case reportJ Dent Child (Chic) 2010 77:99-101. [Google Scholar]
[10]. Primosch RE, Anterior supernumerary teeth--assessment and surgical intervention in childrenPediatr Dent 1981 3:204-15. [Google Scholar]
[11]. Leyland L, Batra P, Wong F, Llewelyn R, A retrospective evaluation of the eruption of impacted permanent incisors after extraction of supernumerary teethJ Clin Pediatr Dent 2006 30:225-31. [Google Scholar]
[12]. Poyton GH, Morgan GA, Crouch SA, Recurring supernumerary mandibular premolars. Report of a case of postmature developmentOral Surg Oral Med Oral Pathol 1960 13:964-66. [Google Scholar]
[13]. King NM, Lee AM, Wan PK, Multiple supernumerary premolars: their occurrence in three patientsAust Dent J 1993 38:11-16. [Google Scholar]