The aim was to evaluate treatment outcomes after apicoectomy and apexification in adjacent non-vital maxillary central incisors with large periapical radiolucencies, in a 10-year-old boy. The patient had complained of tenderness in the upper central incisors on mastication and gave a history of trauma to those teeth three years ago. On examination, there were found to be non-vital. Apexification (using Metapex) and apicoectomy (obturation with gutta percha) were performed on 11 and 21, respectively. Radiographical observations were made six months, one year and two years, post-operatively. Apical repair was found to be more favorable after apicoectomy than apexification, for a non-vital maxillary central incisor with an open apex and large periapical radiolucency.
Apicoectomy, Apexification, Metapex, Calcium hydroxide, MTA
Case Report
A 10-year-old boy reported to the Department of Pedodontics and Preventive Dentistry with a chief complaint of tenderness in the upper central incisors (11, 21) on mastication. He gave a history of trauma to those teeth three years ago. On clinical examination, they were found to be tender on percussion and were non-responsive to the cold test as well as the electric pulp test (Vitapulp, Pelton and Crane Co., North Carolina, USA). There was no discoloration or misalignment of the incisors.
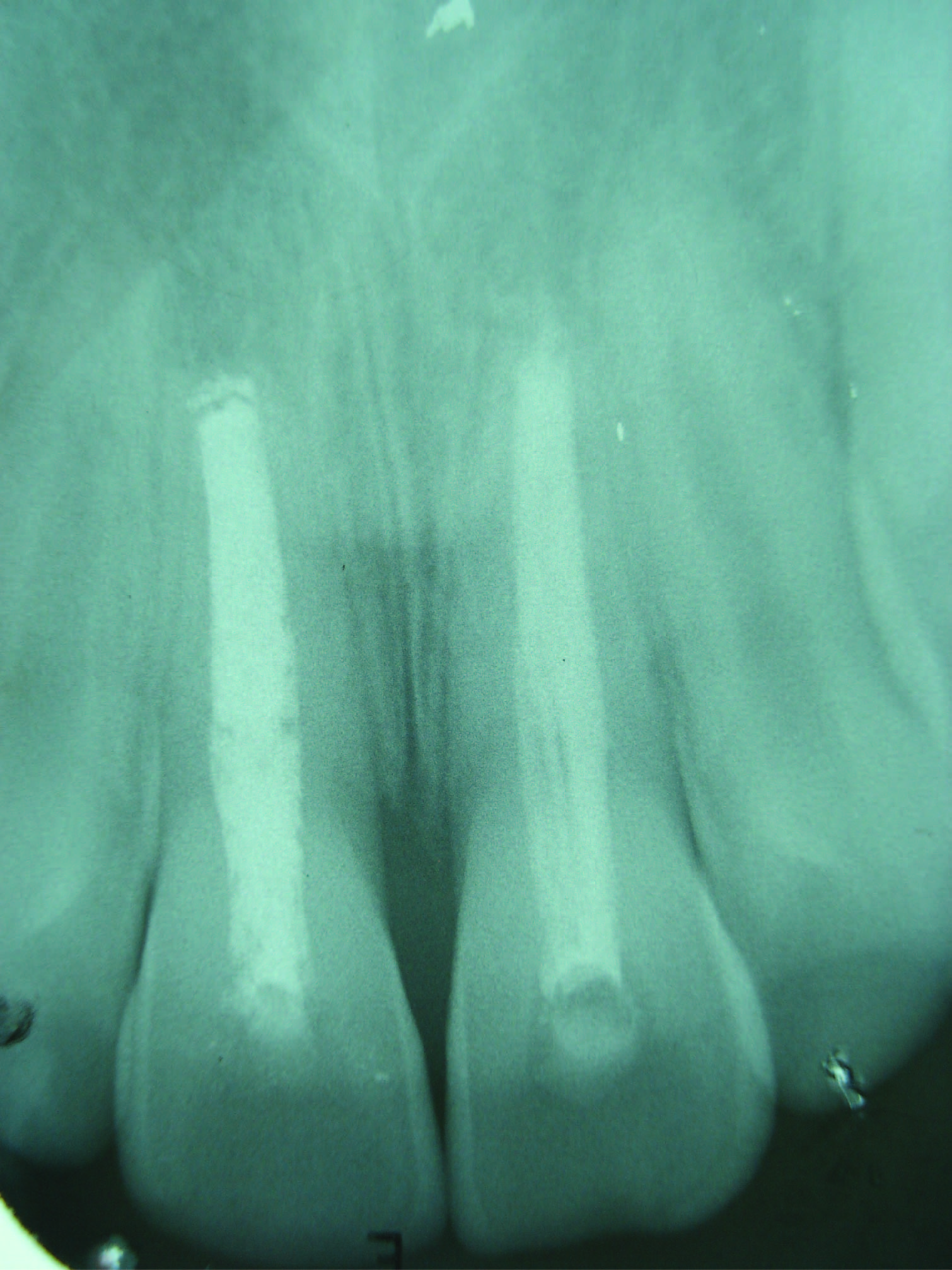
A sinus tract was present in relation to 21 [Table/Fig-1]. A radiograph revealed peri-apical radiolucencies of nearly equal dimensions(10 x 6 millimeters) and incomplete apices in relation to 11 and 21 [Table/Fig-2]. A diagnosis of pulpal necrosis was made and it was decided to perform apicoectomy and apexification for 21 and 11, respectively. A written consent was obtained from the boy’s parents before undertaking the procedures.
Sinus tract opening in relation to 21

Incomplete apices and large radiolucencies in relation to 11 and 21

The root canals were enlarged up till file Kerr # 80, followed by step-back preparation. Irrigation was carried out with 1% sodium hypochlorite. Apexification was carried out for 11 using Metapex (Meta Dental Corporation, USA) filled up till its apex, and the access opening was sealed with glass ionomer cement (GC 9, GC Corporation, Japan).
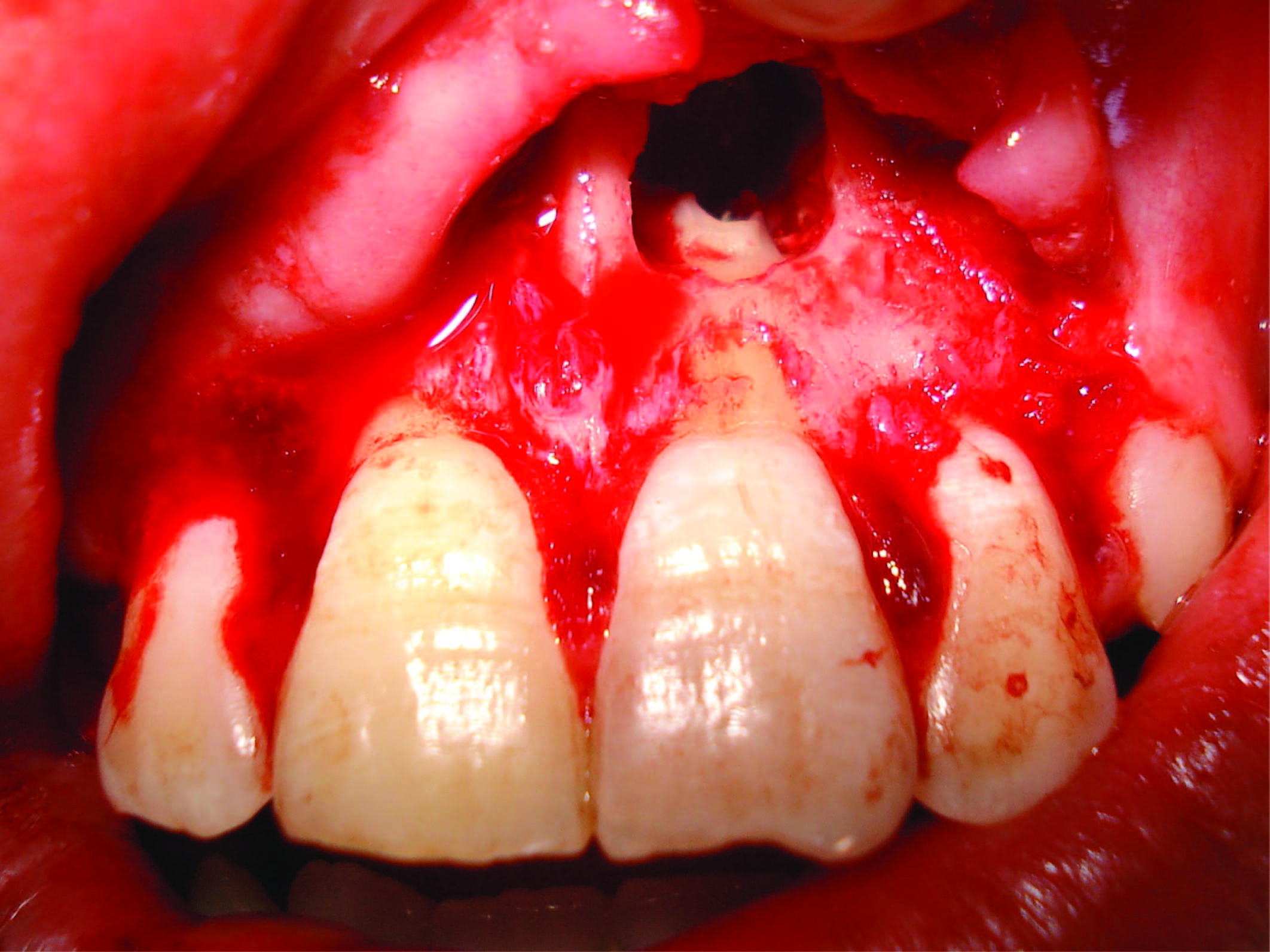
Obturation for 21 was done using gutta percha cones plasticized with heat, rolled and moulded into the root canal with a resin based sealer (AH 26, Dentsply/ Detray, Germany), using thermo-mechanical compaction. A full thickness envelope flap was raised extending from the distal papilla of the lateral incisor of one side to that of the opposite side. Thin cortical bone was removed to create a window in relation to 21 with a slow speed fissure cutting bur using water coolant. Periapical curettage was done with straight or angled instruments and dentin excavators. Apical resection was made to the amount just required for preparing the retrograde cavity (less than 2 millimeters; [Table/Fig-3]). MTA (Mineral trioxide aggregate) was used as the retrograde filling material, and the exposed root surface was treated with 1.23 % acidulated phosphate fluoride gel for 10 minutes before wound closure. Suturing was done with triple-zero silk to reposition the flap [Table/Fig-4]. Antibiotics, NSAID and an oral rinse solution were prescribed, and the sutures were removed on the seventh postoperative day.
Apical resection in relation to 21

After six months of treatment, the radiolucencies associated with 11 and 21 appeared to have resolved (5 x 3 millimeters) as compared to previous measurements [Table/Fig-5]. After one year of treatment [Table/Fig-6], 21 showed absence of any radiolucency. However, 11 showed an ill defined radiolucency measuring 3 x 2 millimeters, although an apical barrier had formed. Metapex was retrieved and gutta percha was used for obturating 21.
Radiograph in relation to 11 and 21, six months post-operatively

Radiograph in relation to 11 and 21, one year post-operatively
After two years of treatment [Table/Fig-7], both 11 and 21 were asymptomatic, without any signs of swelling, tenderness or pathological mobility. There was no periapical radiolucency in relation to 21, although 11 showed an ill-defined radiolucency measuring 3 x 2 millimeters. However, trabecular bone growth was evident within the radiolucency in relation to 11.
Radiograph in relation to 11 and 21, two years post-operatively

Discussion
Apicoectomy has been recommended as a retreatment procedure after endodontic failure [1]. However, apicoectomy, as the first choice of treatment for non-vital incisors with large periapical defects has seldom been documented. In our patient, mineral trioxide aggregate (MTA) was used to obtain the apical seal. It has been known for its outstanding tissue compatibility, and has been found to promote periradicular healing and the production of cementum and bone [2–4]. Fluoride treatment was done for the exposed root surface following apicoectomy, to prevent root resorption owing to loss of predentine or precementum due to surgical heat liberation, irregular cutting or the presence of micro-organisms [5].
Torabinejad et al., found a success rate of 77.8% for periradicular surgery at 2-4 y and a rate of 71.8% at 4-6 y [6]. Zuolo et al., recorded success in 91.1% of cases and failure in 8.8%, over a follow-up period between 1-4 y [7]. In our patient, the incisor in which apicoectomy was performed, presented with complete disappearance of the periapical lesion after one year along with absence of tenderness to percussion, inflammation or tenderness. The tooth was asymptomatic even at the end of a two year follow up. Our finding, although in a single tooth, largely differ from those of Vallecillo Capilla et al., who found clinical and radiological success rates of only 58.6% and 55.2%, respectively, after a one year of follow-up [8].
Apexification is a form of treatment that involves cleaning of the root canal and filling it with a temporary medication that stimulates the formation of a calcified barrier at the apex, after which, permanent obturation with gutta-percha is done. Favourable results have been obtained after apexification in narrow open apex cases [9,10]. However, in our patient, the upper central incisor with a wide open apex also showed successful apical barrier formation at the end of one year.
Little success has been reported when apexification was performed after the development of a periapical pathology [11]. Ghosh et al., found a success rate of only 21.6% in such cases [9]. In our patient, the upper central incisor had established periapical radiolucency before apexification was performed. However, an apical barrier was evident after 12 months. Thus, our finding is similar to those of Dominguez et al., who observed that the presence or absence of apical pathology before treatment hardly influences the duration for successful apical closure [12].
A success rate of 74% to 100% has been reported with the use of different formulations of calcium hydroxide for apexification [10,13–15]. Walia et al., and Dominguez et al., observed apical barrier formation occurring at 7 ± 2.5 months and six months, respectively [10,12]. However, in our patient, apical barrier formation was observed in 12 months. Metapex (mixture of calcium hydroxide and iodoform) was used in our patient for apexification. A success rate of 100% was found in a study that used a calcium hydroxide- iodoform mixture as the intracanal medicament, wherein, the average time for the apical barrier to form was found to be 6.09 mnth [15]. Although 11 showed an ill-defined radiolucency two years post-operatively, it may be considered as a successful outcome, because trabecular bone growth was evident in the region, and the tooth is asymptomatic with no signs of swelling, tenderness or pathological mobility.
In this case report, the comparison between outcomes of apicoectomy and apexification has been made from adjacent maxillary central incisors with periapical radiolucencies of equal size. Moreover, since the procedures were done in the same patient, the physiological response in terms of healing and repair would have been the same, unaffected by geographical location, ethnicity or socio-economic status. There is no study in literature as yet that has documented a similar comparison. However, more number of similar cases would need to be treated so as to ascertain the benefit of one procedure over another.
Conclusion
Apical repair was found to be more favorable after apicoectomy than apexification, for a non-vital maxillary central incisor with an open apex and large periapical radiolucency.
[1]. Furusawa M, Asai Y, SEM observations of resected root canal ends following apicoectomyBull Tokyo Dent Coll 2002 43:7-12. [Google Scholar]
[2]. Torabinejad M, Parirokh M, Mineral trioxide aggregate: a comprehensive literature review--part II: leakage and biocompatibility investigationsJ Endod 2010 36:190-202. [Google Scholar]
[3]. Ghoddusi J, Tavakkol Afshari J, Donyavi Z, Brook A, Disfani R, Esmaeelzadeh M, Cytotoxic effect of a new endodontic cement and mineral trioxide aggregate on L929 line cultureIran Endod J 2008 3:17-23. [Google Scholar]
[4]. Asgary S, Eghbal M, Ehsani S, Periradicular regeneration after endodontic surgery with Calcium-Enriched Mixture cement in dogsJ Endod 2010 36:837-41. [Google Scholar]
[5]. Soares JA, Silveira FF, Nunes E, Apical surgery with calcium hydroxide capping of the exposed dentine: a case reportJ Oral Sci 2007 49:79-83. [Google Scholar]
[6]. Torabinejad M, Corr R, Handysides R, Shabahang S, Outcomes of nonsurgical retreatment and endodontic surgery: a systematic reviewJ Endod 2009 35:930-37. [Google Scholar]
[7]. Zuolo M, Ferreira M, Gutmann J, Prognosis in periradicular surgery: a clinical prospective studyInt Endod J 2000 33:91-8. [Google Scholar]
[8]. Vallecillo Capilla M, Muñoz Soto E, Reyes Botella C, Prados Sáchez E, Olmedo Gaya MV, Periapical surgery of 29 teeth. A comparison of conventional technique, microsaw and ultrasoundMed Oral 2002 7:46-9.:50-3. [Google Scholar]
[9]. Ghosh S, Mazumdar D, Ray PK, Bhattacharya B, Comparative evaluation of different forms of calcium hydroxide in apexificationContemp Clin Dent 2014 5:6-12. [Google Scholar]
[10]. Walia T, Chawla HS, Gauba K, Management of wide open apices in non-vital permanent teeth with Ca (OH) 2 pasteJ Clin Pediatr Dent 2000 25:51-6. [Google Scholar]
[11]. Kusgoz A, Yildirim S, Gokalp A, Nonsurgical endodontic treatments in molar teeth with large periapical lesions in children: 2-year follow-upOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 104:60-5. [Google Scholar]
[12]. Dominguez Reyes A, Muñoz Muñoz L, Aznar Martín T, Study of calcium hydroxide apexification in 26 young permanent incisorsDent Traumatol 2005 21:141-5. [Google Scholar]
[13]. Gu HJ, Xu Q, Liu LM, Ouyang Y, Treatment of chronic apical periodontitis teeth complicated by open apices with Vitapex in the adultsShanghai Kou Qiang Yi Xue 2007 16:140-43. [Google Scholar]
[14]. Rodd HD, Davidson LE, Livesey S, Cooke ME, Survival of intentionally retained permanent incisor roots following crown root fractures in childrenDent Traumatol 2002 18:92-97. [Google Scholar]
[15]. de Jesus Soares A, Yuri Nagata J, Casarin RC, Flávio Affonso de Almeida J, Gomes BP, Augusto Zaia A, Randi Ferraz CC, José de Souza-Filho F, Apexification with a new intra-canal medicament: a multidisciplinary case reportIran Endod J 2012 7:165-70. [Google Scholar]