Background: The effect of thyroid status on insulin sensitivity is of great interest but despite various studies there is conflicting data on this subject. Hypothyroidism has been associated with disorders of glucose and insulin metabolism involving defective insulin secretion in response to glucose, hyperinsulinemia, altered peripheral glucose disposal and insulin resistance. Thyroid dysfunction leads to alterations in glucose and lipid metabolism which is an important risk factor for cardiovascular diseases. The dyslipidemia and insulin resistance should be managed aggressively to reduce the impending risk.
Objectives: The prime objectives of the study were as follows:
1. To compare and correlate insulin resistance levels with T3, T4, and TSH in hypothyroidism patients.
2. To compare and correlate lipid profile with T3, T4, and TSH in hypothyroidism patients with healthy controls.
Materials and Methods: Forty hypothyroidism patients and Forty healthy age and sex matched controls in the age group of 18 to 45 years were taken for the study. The venous blood samples collected were used for estimation of thyroid hormones, insulin, glucose and lipid profile.
Results and Discussion: There is significant increase in insulin, Homa-IR and glucose levels in hypothyroidism cases when compared to controls. Cholesterol, LDL, VLDL and triglycerides were significantly increased, whereas HDL was significantly decreased in hypothyroidism cases when compared with controls. Insulin was moderately correlated with cholesterol but there was no correlation with other lipid profile parameters in hypothyroidism patients. Homa-IR was significantly correlated with TSH in hypothyroidism cases when compared with controls. TSH was significantly correlated with cholesterol and LDL in hypothyroidism cases (both clinical and subclinical) when compared with controls. The present study helps to evaluate changes in insulin resistance and lipid risk factors. These factors should be managed aggressively to reduce the impending risk of cardiovascular diseases.
Introduction
Hypothyroidism has insidious onset and diagnosis can be delayed by months or years. Quite often cardiovascular manifestations go unrecognized or subclinical. The heart muscle and arterial tree are the worst affected in hypothyroidism. Cardiac output at rest is decreased, reflecting the loss of inotrophic and chronotrophic effects of thyroid hormone. These alterations cause narrowing of pulse pressure, prolongation of circulation time and decrease in blood flow to the tissue [1-3].
Hypothyroidism has been associated with disorders of glucose and insulin metabolism involving defective insulin secretion in response to glucose, hyperinsulinemia, altered peripheral glucose disposal and insulin resistance [4]. Insulin resistance indicates the presence of an impaired peripheral tissue response to endogenously secreted insulin. Insulin resistance leads to an increased production of hepatic cholesterol, very low density lipoproteins (VLDL) and an increased high density lipoprotein- cholesterol (HDL-C) clearance. Insulin resistance augments the deleterious effect of hypothyroidism on the lipid profile [5].
In euthyroid non-diabetic adults, the relationship between serum TSH and cholesterol appears to be modified by insulin resistance, such that those with higher serum TSH and relative insulin resistance are at greater risk of dyslipidemia [6]. This shows that hypothyroidism is a risk factor for insulin resistance, hyperlipidemia, hypercoagulability and low grade inflammation which lead to cardiovascular diseases [5].
Hence, in the present study we aim to evaluate and correlate insulin resistance, lipid profile in clinical and subclinical hypothyroid patients which will help to better evaluate and manage the impending cardiovascular diseases.
Materials and Methods
The study was a cross-sectional study and undertaken on 40 hypothyroidism patients diagnosed by increased TSH level and decreased T3, T4 or normal T3, T4, in the age group of 18 years to 45 years attending the Medicine out-patient department and patients admitted in the medicine ward of a tertiary care hospital and 40 healthy age and sex matched controls. Exclusion criteria included patients with diabetes mellitus type 2, polycystic ovarian disease, tuberculosis and patients on medications that alter lipid levels such as statins.
The study protocol was approved by the institutional ethical committee before the commencement of the study. Aseptically 5ml of venous blood was collected and a written consent was taken from the respective patients and controls. Fasting blood samples were collected from the patients and were carried to the laboratory in an ice-container. It was used to estimate fasting plasma glucose, T3, T4, TSH, insulin and lipid profile (triglyceride, total cholesterol, HDL-cholesterol, LDL-cholesterol and VLDL- cholesterol). Homeostatic model assessment (HOMA) is a method for assessing cell function and insulin resistance (IR) from basal (fasting) glucose and insulin or C-peptide concentrations [5].
Insulin resistance was calculated using the formula [5]:

(Conversion from mmol/l to mg/dl = mmol/l X 18)
The blood was allowed to clot and serum was separated by centrifugation at 5000 rpm for 5min. The serum was then used to estimate fasting plasma glucose (GOD-PAP method), triglcerides (GPO-PAP method), and total cholesterol and HDL- cholesterol (enzymatic end point method) using Randox Daytona auto analyser. Insulin, T3, T4 and TSH (Direct Chemiluminometric Assay - two site sandwich immunoassay method) were analysed using Bayers automated Chemiluminescence System (ACS: 180) (Automated Hormone Analyzer). Friedwald Equation was used for quantitative determination of LDL-Cholestrol [7].
Statistical Analysis
Student’s t-test was applied at 5% level, to test the significance of difference in the parameters under study, in the case and control group. Pearson’s correlation was applied among various parameters under study. The analysis of data was performed using SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0 and R environment ver.2.11.1 and a p-value of < 0.05 was considered significant.
Results
The study was conducted on 40 patients with hypothyroidism and 40 healthy controls. The cases and controls were age and sex matched. The mean age in hypothyroid patients was 32.08±7.56 y and in controls was 30.95 ± 8.33 years and the difference was not statistically significant. Among the hypothyroid patients there were 4 males and 36 females which suggest that hypothyroidism is more prevalent in women when compared to men. Many previous studies state that women are five to eight times more likely to develop hypothyroidism when compared to men [5].
The mean insulin, Homa-IR and glucose levels were significantly increased (p < 0.01) in hypothyroid patients when compared to controls. The mean levels of lipid profile parameters (total cholesterol, HDL-cholesterol, LDL-cholesterol, VLDL- cholesterol and triglyceride) were significantly increased (p <0.01) in hypothyroid patients when compared to controls. The mean levels of T3 and T4 were significantly decreased (p < 0.01), where as TSH levels were significantly increased (p < 0.01) in hypothyroid patients when compared to controls [Table/Fig-1].
Hypothyroid patients were divided into clinical and subclinical hypothyroid groups based on T3, T4 and TSH levels. The mean age of clinical hypothyroid patients was 32.00 ± 7.72 years and in subclinical hypothyroid patients was 32.15 ± 7.60 years as shown in [Table/Fig-2]. Both the groups were age matched and consisted of 2 males and 18 females respectively. The mean insulin, Homa-IR levels were almost same in clinical hypothyroid patients when compared to subclinical hypothyroid patients but the fasting glucose levels were lower in clinical hypothyroid patients when compared to subclinical. The mean levels of lipid profile parameters were almost same in clinical and subclinical groups. The mean levels of T3 and T4 were significantly decreased, where as TSH levels were significantly increased (p< 0.01) in clinical hypothyroid patients when compared to subclinical cases [Table/Fig-2].
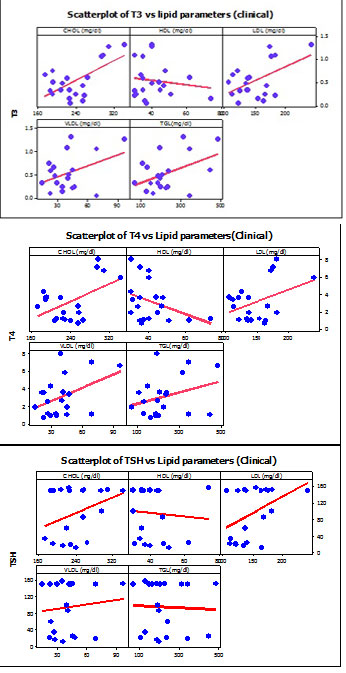
Homa-IR was positively correlated with TSH, whereas insulin did not correlate with thyroid hormones in hypothyroid patients [Table/Fig-3]. TSH was positively correlated with cholesterol and LDL, where as T3 and T4 did not correlate with lipid profile in hypothyroid patients [Table/Fig-4].
T3, T4 levels were positively correlated with cholesterol in clinical group, where as TSH did not correlate [Table/Fig-5]. However, in subclinical group TSH levels correlated with cholesterol but other lipid profile parameters showed no significant correlation with thyroid hormones in the two groups. Homa-IR and insulin positively correlated with thyroid hormones in clinical group, where as Homa-IR did not correlate with TSH in subclinical group [Table/Fig-6,Table/Fig-7]. Homa-IR significantly correlated with cholesterol, LDL, VLDL and triglycerides but correlation between Homa-IR and HDL was not significant in both clinical and subclinical hypothyroidism patients [Table/Fig-8,Table/Fig-9].
Discussion
In the present study it was observed that the mean values of T3, T4 were significantly decreased and TSH were increased in cases (both clinical and subclinical) when compared to controls and this correlates to the findings of American Association of Clinical Endocrinologists, which states that there will be decrease in T3, T4 levels in clinical hypothyroidism or normal levels of T3, T4 in subclinical hypothyroidism along with increased levels of TSH (both clinical and subclinical) [8].
There was significant increase in insulin, Homa-IR and glucose levels in cases (both clinical and subclinical) when compared to controls. This is explained by previous studies which stated that, hypothyroidism is associated with disorders of glucose and insulin metabolism, involving defective insulin secretion in response to glucose, hyperinsulinemia, altered peripheral glucose disposal and insulin resistance [4,9]. In the present study it was observed that the mean values of lipid profile parameters including cholesterol, LDL, VLDL and triglycerides were significantly increased in cases, where as HDL was significantly decreased in cases when compared with controls. The changes in lipid profile components in the present study are common abnormalities of lipoprotein metabolism associated with hypothyroidism. The elevation in cholesterol, triglyceride and LDL is accounted by the effect of thyroid hormone on lipoprotein lipase activity and the expression of LDL receptor, and these changes probably play an important role in atherogenesis in untreated hypothyroidism [10].
Hypothyroidism cases were divided into clinical and subclinical hypothyroidism based on T3, T4 and TSH levels [8]. Studies have shown the correlation of clinical hypothyroidism with insulin resistance and dyslipidemia [5,7,11], but the studies correlating with sub clinical hypothyroidism with these metabolic conditions are lacking’.
In the present study it was observed that insulin was positively correlated with cholesterol but there was no correlation with other lipid profile parameters in hypothyroidism patients. We observed that Homa-IR was positively correlated with TSH in hypothyroidism patients both clinical and subclinical cases when compared with controls. This corresponds well with the studies showing that patients with mild thyroid failure and even subjects with high normal serum TSH values have evidence of comparable atherogenic factors, such as endothelial dysfunction manifested by flow mediated endothelial–dependent vasodilatation and high serum cholesterol levels. Moreover, the fact that insulin resistance was similar in patients with clinical and subclinical hypothyroidism indicates that thyroid hormones levels per se may not be entirely responsible for the manifestation of this phenomenon and may be due to impairment of insulin signaling cascade and phosphorylation pattern of signaling molecules (such as insulin receptor substrate 1) with decreased glucose uptake [12,13].
The interaction between insulin resistance and high TSH has profound clinical implications. At low insulin sensitivity, relatively minor differences in TSH are associated with marked changes in lipid risk factors and thus cardiovascular risks [5,13]. Another study showed that females with insulin resistance have significant association with subclinical and clinical hypothyroidism [5].
In the present study, we observed that insulin was positively correlated with thyroid hormones in clinical hypothyroidism but not in subclinical hypothyroidism. Our findings correlate to a study which concluded that insulin concentrations correlate with FT4 but not with FT3 or TSH in profound hypothyroidism [5].
In the present study, we observe that TSH was positively correlated with cholesterol and LDL in hypothyroidism patients which means, as TSH increases, consequently cholesterol and LDL also rises. Thyroid hormones increase adipose tissue lipolysis as measured by high free fatty acids or glycerol release. From the above facts, the high atherogenic lipids in hypothyroidism can be explained indirectly as a subsequence of the reduction of thyroid hormones [10].
Mean ± SD values of different parameters in the two study groups
p>0.05: Not Significant, *p: <0.05: Significant, ** p: <0.01: Highly significant, *** p: <0.001: Very highly significant
| Parameters | Cases (40) M=04; F=36 (Mean ± SD) | Controls (40) M=04; F=36 (Mean ± SD) | p value |
|---|
| Age (years and months) | 32.08±7.56 | 30.95±8.33 | > 0.05 |
| FBS (mg/dl) | 92.67±4.46 | 77.75±4.79 | <0.001** |
| Insulin (mu/l) | 31.15±48.53 | 5.82±2.45 | 0.001** |
| HOMA-IR | 7.12±10.88 | 1.11±0.46 | 0.001** |
| CHOL (mg/dl) | 236.85±57.02 | 146.00±9.76 | <0.001** |
| HDL (mg/dl) | 41.12±10.90 | 47.47±5.01 | 0.001** |
| LDL (mg/dl) | 153.67±44.04 | 82.12±10.12 | <0.001** |
| VLDL (mg/dl) | 37.27±17.09 | 18.90±5.02 | <0.001** |
| TGL(mg/dl) | 207.47±93.74 | 88.72±15.58 | <0.001** |
| T3 (ng/ml) | 0.70±0.37 | 1.00±0.24 | <0.001** |
| T4 (μg/dl) | 4.82±2.91 | 8.38±1.61 | <0.001** |
| TSH(μIu/ml) | 66.05±61.59 | 2.45±1.25 | <0.001** |
Mean ± SD values of different parameters in the two groups of cases
p>0.05: Not Significant, *p: <0.05: Significant, ** p: <0.01: Highly significant, *** p: <0.001: Very highly significant
| Parameters | Clinical (20) M=02; F=18 (Mean ±SD) | Subclinical (20) M=02; F=18 (Mean ±SD) | p-value |
|---|
| Age (years and months) | 32.00±7.72 | 32.15±7.60 | >0.05 |
| FBS (mg/dl) | 90.65±4.59 | 94.70±3.35 | 0.003* |
| Insulin (mu/l) | 22.23±19.44 | 40.08±65.49 | 0.250 |
| HOMA-IR | 4.99±4.41 | 9.25±14.63 | 0.221 |
| CHOL (mg/dl) | 238.45±46.59 | 234.85±67.05 | 0.845 |
| HDL (mg/dl) | 43.40±13.36 | 38.85±7.39 | 0.191 |
| LDL (mg/dl) | 149.45±32.59 | 157.90±53.69 | 0.551 |
| VLDL (mg/dl) | 39.75±19.67 | 34.80±14.14 | 0.367 |
| TGL(mg/dl) | 227.75±109.29 | 187.20±72.30 | 0.175 |
| T3 (ng/ml) | 238.45±46.59 | 234.85±67.05 | <0.001** |
| T4 (μg/dl) | 43.40±13.36 | 38.85±7.39 | <0.001** |
| TSH(μIu/ml) | 149.45±32.59 | 157.90±53.69 | <0.001** |
Correlation between Homa-IR and insulin with T3, T4 and TSH

Correlation between T3, T4, TSH and lipid profile

Correlation of T3, T4 and TSH with lipid profile parameters
Correlation between HOMA-IR and Insulin with T3, T4 and TSH

Correlation between HOMA-IR and Insulin with T3, T4 and TSH

Correlation between Homa-IR and lipid profile

Scatter plots showing the correlation between Homa-IR and lipid profile

Conclusion
Hence, in the present study we observed that there is an association between insulin resistance and cholesterol levels with hypothyroidism (both clinical and subclinical) which justify that there is an increased risk for insulin resistance disorders, such as cardiovascular disease and metabolic syndrome. Therefore, screening and treatment for both clinical and subclinical hypothyroidism may be warranted due to its adverse effects on lipid metabolism and insulin resistance state.
[1]. LP Reed, FD Terry, DH Ian, Thyroid physiology and Diagnostic evaluation of patients with thyroid disorders and Hypothyroidism and Thyroiditis In Williams Text book of Endocrinology 2003 10th EditionW.B. Saunders Company:331-55. [Google Scholar]
[2]. WS Ellen, HW Gordon, The heart in endocrine disorders, A text book of Cardio vascular Medicine 2001 6th EditionW.B. Saunders Company:2158-59. [Google Scholar]
[3]. JJ Larey, Weetman Antony P, Disorders of thyroid gland, Harrison’s principles of internal medicine 2005 16th EditionThe McGraw Hill Companies:2104-13. [Google Scholar]
[4]. M Peppa, C Koliaki, SP Nikolopoulo, SA Raptis, Skeletal muscle insulin resistance in endocrine diseaseJ Biomed Biotechnol 2010 2:1-13. [Google Scholar]
[5]. BM Singh, B Goswami, V Mallika, Association between insulin resistance and hypothyroidism in females attending a tertiary care hospitalIndian J Clin Biochem 2010 25(2):141-45. [Google Scholar]
[6]. SAP Chubb, WA Davis, TME Davis, Interactions among Thyroid function, Insulin sensitivity and serum lipid concentrations; The Fremantle Diabetes studyJ Clin Endocrinol Metab 2005 90(9):5317-20. [Google Scholar]
[7]. N Rifai, RG Warnick, AK Shetty, AK Shetty, Lipids, lipoproteins, apolipoproteins and other cardiovascular risk factors in Teitz textbook of clinical chemistry Carl A Burtis, Edward R Ashwood, david E Burns. Editors 2006 4th EditionPhiladelphiaW.B Saunders:903-81. [Google Scholar]
[8]. JR Garber, CR Hamilton, Y Handelsman, R Hellman, JS Kukora, P Levy, American association of clinical endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidismEndocrine practice 2002 8(6):457-67. [Google Scholar]
[9]. K Boelaert, JA Franklyn, Thyroid hormone in health and diseaseJ Endocrinol 2005 187(1):1-15. [Google Scholar]
[10]. HK Al-Hakeim, Serum levels of lipids, calcium and magnesium in women with hypothyroidism and cardiovascular diseaseJ Lab Physicians 2009 1(2):49-52. [Google Scholar]
[11]. S Danzi, I Klein, Thyroid hormone and the cardiovascular systemMinerva Endocrinol 2004 29:139-50. [Google Scholar]
[12]. P Purohit, Estimation of serum insulin, Homeostasis model assessment – insulin resistance and C-peptide can help to identify possible cardiovascular disease risk in thyroid disorder patientsIndian J Endocrinol Metab 2012 16:S97-103. [Google Scholar]
[13]. E Maratou, DJ Hadjidakis, A Kollias, K Tsegka, M Peppa, M Alevizaki, Studies of insulin resistance in patients with clinical and subclinical hypothyroidismEur J Endocrinol 2009 160(5):785-90. [Google Scholar]