Introduction: Cardiovascular autonomic neuropathy (CAN) is one of the major complications of Diabetes Mellitus (DM) seen in a significant number of patients, which is often ignored and is also least frequently diagnosed. It can be diagnosed by performing five standard non-invasive bedside autonomic function tests based on Cardiovascular reflexes, which are quite cumbersome. Studies have revealed an increase in mortality in the diabetic patients with CAN due to silent cardiac ischemia, sudden cardiac death, arrhythmias. The precursor of diabetic cardiomyopathy is Left ventricular diastolic dysfunction (LVDD). In the present study we are studying the association between LVDD and CAN, in order to identify high mortality risk patients by performing 2D Echo and looking at LVDD instead of performing the cumbersome bedside cardiovascular autonomic function tests.
Aims and Objectives: To study the association between LVDD and CAN in patients with Type 2 DM.
Materials and Methods: This study is a cross-sectional observational study with a sample size of 100. Both outpatients and inpatients between 35 y and 65 y of age with Type 2 DM coming to Department of General Medicine, KIMS hospital, Bangalore were studied from November 2011 to October 2013.Patients with macrovascular complications, Hypertension, congenital & acquired heart diseases etc. were excluded from the study. The standard five autonomic function tests based on cardiovascular reflexes and 2D Echo were performed. Individual scores for each of the five tests were added to produce Ewing’s score. Ewing’s score of >2.5 is positive for CAN.
Statistical Analysis: Chi-square/ Fisher Exact test has been.
Results: There was a significant association between individual non-invasive bedside tests of Ewing’s score and LVDD. Significant association was also seen between LVDD and positive Ewing’s score.
Conclusion: Positive Ewing’s score is strongly associated with LVDD in patients with Type 2 DM in this study .This suggests that patients with LVDD have CAN and hence, are at increased risk of sudden cardiac death. As bedside tests are cumbersome, patients with LVDD on 2D Echo can be concluded to have CAN.
Introduction
DM affects an estimated 250 million worldwide [1]. According to the Indian Council of Medical Research-Indian Diabetes study (ICMR-INDIAB), a national DM study, India currently has 62.4 million people with DM [2]. The majority of people with DM (>90%) have Type 2 DM (T2DM). Diabetic neuropathies, including CAN, are a common chronic complication of type 1 and type 2 DM and confer high morbidity and mortality to diabetic patients [3]. CAN prevalence was as low as 2.5% of the primary prevention cohort in the Diabetes Control and Complications Trial (DCCT) [4]. It can also be as high as 90% in long standing type 1 DM patients requiring pancreas transplantation [5]. Hence, the prevalence can vary from 2.5% to 90%.
CAN is an important complication of diabetes mellitus (DM) even then it is least frequently diagnosed. Patients with type 2 DM may develop cardiomyopathy independently of coronary artery disease and associated hypertension. LVDD is considered a precursor of diabetic cardiomyopathy [6].
CAN occur when sympathetic and parasympathetic cardiovascular fibres are affected which in turn leads to neurohormonal compromise. Sympathetic over activity stimulates the renin–angiotensin– 2aldosterone system and increases heart rate, stroke volume, and peripheral vascular resistance, thus contributing to LV dysfunction [7].
As we now know, CAN is associated with LV diastolic dysfunction (LVDD), both in patients with long-term type 2 or type 1 diabetes. LVDD may progress to heart failure, mainly with preserved LV systolic function (diastolic heart failure), which is also related to high morbidity and mortality rates. Sudden, unexpected deaths occur among subjects with CAN. One potential cause may be severe but asymptomatic ischemia, which can induce lethal arrhythmias [6,8,9].
CAN is often ignored due to mild symptoms and is also least frequently diagnosed. It can be diagnosed by performing five noninvasive bedside autonomic function tests which are quite cumbersome such as Valsalva maneuver, deep breathing test, change in SBP and heart rate on standing, change in diastolic blood pressure with hand grip. In the present study we are studying the association between LVDD and CAN, in order to identify high mortality risk patients by performing 2D Echo and looking at LVDD instead of performing the cumbersome bedside cardiovascular autonomic function tests in Type 2 Diabetes Mellitus patients.
Aims And Objectives
To study the association between LVDD and CAN in patients with Type 2 Diabetes Mellitus.
Materials and Methods
This study was a Cross-sectional observational study with a sample size of 100 patients from both Outpatients and Inpatients with Type II Diabetes Mellitus coming to the Department of General Medicine , KIMS hospital, Bangalore from November 2011 to October 2013.
Patients with Type2 Diabetes Mellitus, between 35 years & 65 years yrs. who were on treatment or newly diagnosed diabetics according to ADA criteria were included in the study. Patients with macrovascular complications of type II DM, with Hypertension, with congenital & acquired heart diseases & cardiac arrhythmias were excluded from the study. Patients with Vitamin B12 deficiency, with exposure to Alcohol and on drugs affecting the autonomic function were also excluded. Patients with Renal Failure, with liver diseases, with Parkinson & Parkinson plus syndromes were also excluded.
All patients who have fulfilled the inclusion criteria were subjected to detailed history taking which includes- Gastrointestinal symptoms, bowel and bladder symptoms and other relevant history. Patients were subjected to detailed clinical examination which includes bedside tests for CAN and later 2 D Echo to demonstrate LVDD. Diagnosis of CAN was based on bedside autonomic function tests with Ewing’s score > 2.5 being positive for CAN [10].
CAN was evaluated using Ewing Score based on cardiovascular autonomic function tests.
Tests for cardiovascular Autonomic Function [10] done in this study: Five non-invasive cardiovascular autonomic function tests were conducted.
1. Deep Breathing Test
The patient was made to sit comfortably and asked breathe quietly and deeply at the rate of 6 breaths per minute. A continuous ECG was taken simultaneously with markings at the beginning of each inspiration and expiration. Out of the recordings for each minute, the one with maximum R-R interval and the one with minimum R-R interval is selected and converted to beats per minute. The mean of the difference between maximum and minimum heart rate for six measured cycles is calculated as beats per minute and taken as the result value.
Deep breathing difference (DBD) or delta heart rate (DHR) =mean of heart rate differences in six breath cycles.
A difference of 15 beats/min or more was considered normal, 11-14 beats/min was considered borderline and less than 10 beats/min was taken as abnormal.
2. Heart-Rate Variation to Valsalva Manoeuver
The patient was asked to be seated comfortably and blow into the mercury sphygmomanometer up to 40 mmHg and hold it at that level for 15 sec, while a continuous ECG was being recorded. The patient is asked to release the pressure at the end of 15 sec but however the ECG is continued to record for another 30 sec from the time of release of pressure. The heart rate changes caused by the valsalva manoeuver were expressed as the ratio of the maximal tachycardia during the manoeuver to the maximal bradycardia after the manoeuver. This ratio was defined as the Valsalva ratio and was calculated as the ratio of maximum R-R interval after the manoeuver to minimum R-R interval during the manoeuver.
VR = maximal tachycardia/maximum bradycardia= maximum R-R interval/minimum R-R interval.
An abnormal response was defined for a value of 1.10 or less, 1.11-1.20 as borderline, and 1.21 or more as a normal response.
3. Heart Rate Response to Standing – Postural Tachycardia Index (PTI) (30:15 Ratio)
The patient was asked to lie down comfortably on the examination couch and a continuous ECG was recorded. The patient was later made to stand and a continuous ECG was recorded for a period of one minute. The shortest R-R interval at or around 15th beat and longest R-R interval at or around 30th beat was measured. The result was as ratio of 30/15.
PTI = Longest R-R interval at 30th beat / shortest R-R at 15th beat.
A ratio of 1.00 or less was an abnormal response, 1.01-1.03 was borderline and 1.04 was normal response.
4. Blood Pressure Response to Standing (Orthostatic test)
The patient was made to lie supine comfortably on the examination couch and rest for five minutes. The supine blood pressure was recorded. After five minutes, the patient was made to stand without any support for a period of three minutes. The blood pressure at 30 sec and at the 3rd min after standing was recorded. The difference between supine and standing BP levels was evaluated. The fall in systolic blood pressure (SBP) at 30 sec on standing noted.
A fall of 20 mm Hg or more was defined as abnormal, fall between 11-20 mm Hg as borderline and fall of 10 mm Hg or less was considered normal.
5. Blood Pressure Response to Sustained Handgrip
In this test, sustained muscle contraction was measured by a handgrip dynamometer, causes a rise in systolic and diastolic blood pressure and heart rate. The dynamometer was first squeezed to isometric maximum, and then held at 30% maximum for 5 min. if possible, although even three minutes was adequate. Blood pressure was recorded in the non-exercising arm thrice at one minute interval during the procedure. The maximum reading of the diastolic blood pressure was taken as the final value. Then the rise in diastolic blood pressure was calculated by subtracting resting diastolic blood pressure from this value. A rise in DBP of less than 10 mm Hg was defined as abnormal, 11-15 mm Hg as borderline and 16 mm Hg or more as normal .
Heart rate response to deep breathing, Valsalva manoeuver and standing are known as tests to evaluate parasympathetic nervous system pathway; whereas BP response to standing and to sustained handgrip allow the assessment of sympathetic nervous system activity.
After performing the five non-invasive bedside autonomic function tests, the individual scores of each test were added to get Ewing’s score [Table/Fig-1]. Ewing’s score of >2.5 was positive for CAN.
2D ECHO was done in all patients to look for LVDD by looking at the reversal of E/A ratio, left atrial enlargement and elevated left atrial filling pressure and / or reduced left ventricular ejection fraction. Other routine investigations like FBS, PPBS, HbA1c, serum creatinine, urine routine, ECG, lipid profile were performed in all patients.
Statistical Analysis
In this study Descriptive and inferential statistical analysis has been done. Continuous measurements results are presented on Mean ± SD (Min-Max) and categorical measurements results are presented in Number (%). Five percent level of significance is taken to assess the significance. The following assumptions on data are made, Assumptions: 1. Dependent variables should be normally distributed, 2. Samples drawn from the population should be random, Cases of the samples should be independent [11-14].
Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups [11-14].
Statistical software: The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1, Systat 12.0 and R environment ver. 2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
Results
There was no association between LVDD and gender with a non-significant p-value of 0.245. [Table/Fig-2].The finding of the present study is in conformity with the earlier studies. A study done by Caroline et al., in Malta concluded that there was no association between gender and LVDD [15].
There was a positive association between older group and presence of LVDD on 2D Echo [Table/Fig-2].. There was a positive association between higher age group and Ewing’s score with a p-value of 0.097+.The finding of the present study is in conformity with the earlier studies. A study done by Caroline et al., in Malta concluded that there was a significant association between higher age and LVDD [15].
In this study among the 100 Type 2 Diabetic patients, as shown in [Table/Fig-2], 30 patients had positive Autonomic (Ewing’s) scores and 70 (70%) had negative autonomic scores. Hence, the incidence of CAN in our study was 30% .The incidence of autonomic neuropathy in diabetics, ranged from 17 to 68% in other studies. However, Aaron et al., [16] in their study state that cardiovascular incidence in diabetics varies from 7.7% (Type 1) to even 90% (in pancreatic transplants). Pappachan et al., [17], in their study, showed a prevalence of CAN in 60% of the 100 cases of diabetics studied. Goel et al., [18] have reported 29 out of 75 diabetic patients (39%) to have dysautonomia. Similar results were seen with Oluranti B familoni, Olatunde odusan, Subbalakshmi et al., [19], have showed a prevalence of 37% of dysautonomia among the diabetics under study. Lakhotia et al., [20] in their study, showed that eight out of 12 Type 1 and 24 out of 38 Type 2 diabetics had dysautonomia. Noronha et al., [21] in their study, found that 78.8% of the diabetics had autonomic neuropathy, of which more than 76%, of the total study, had more than one abnormal test present. Purewal and Watkins et al., [22] in a study of 105 diabetics, both Type 1 and Type 2, found an incidence of 50%.
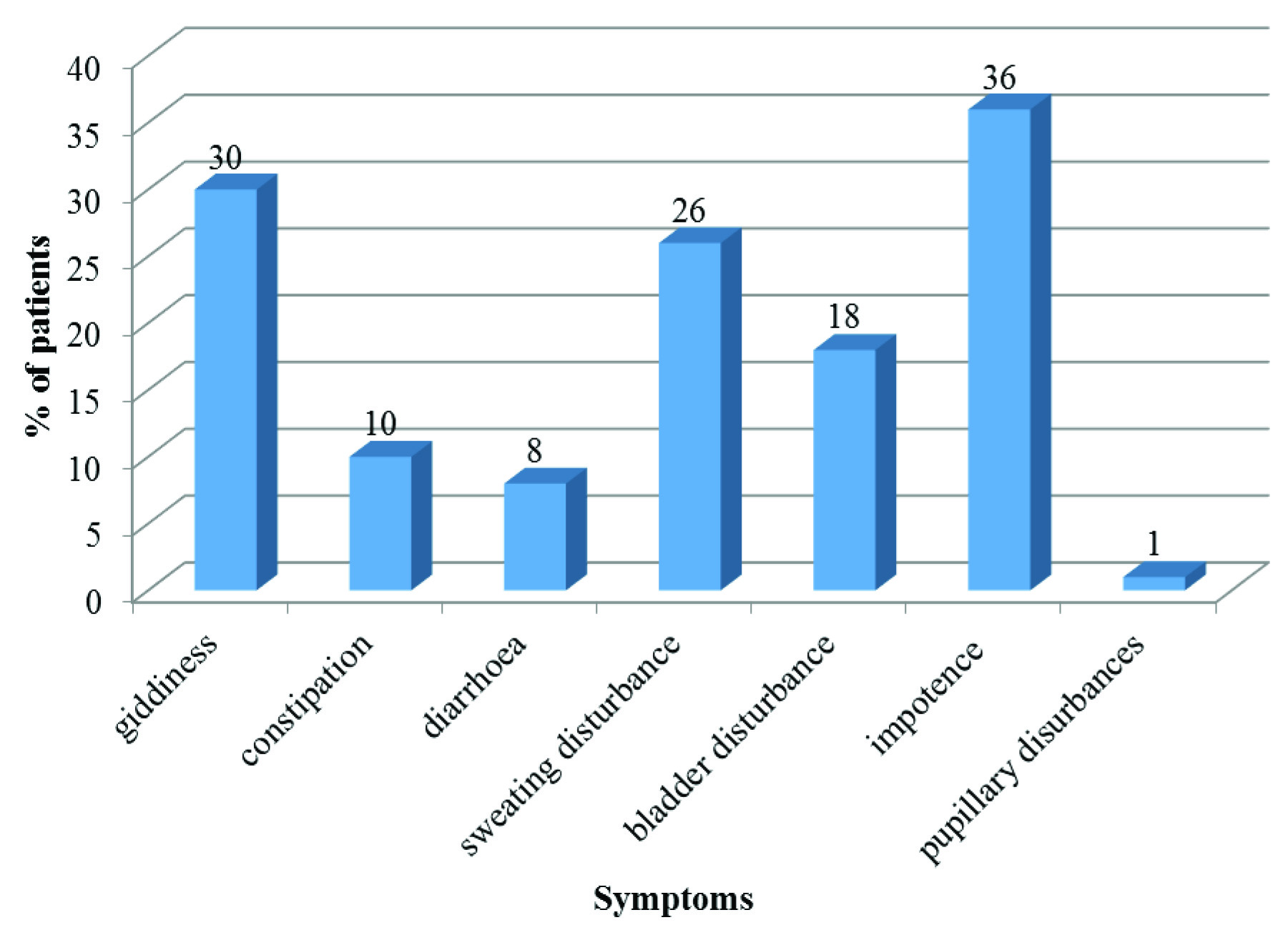
Impotence was the most common symptom in this study [Table/Fig-3]. Rundles [23] found impotence in 19 patients out of 125 diabetic patients. Noronha et al., [21] found impotence in 52% of their study diabetic subjects, being the commonest symptom.
It was concluded from [Table/Fig-4] that the heart rate response to deep breathing, a measure of cardiac parasympathetic function is reduced in Type 2 diabetic patients with LVDD with a significant p-value of 0.028*. The finding of the present study is in conformity with earlier studies. A study involving 207 type 2 Diabetes mellitus done by Subbalakshmi et al., in KMC [19] Mangalore showed that heart rate response to deep breathing, valsalva maneuver and active standing was lower in type 2 Diabetics. Ewing et al., [10] studied 543 diabetic patients and concluded that response to deep breathing was abnormal in diabetics with CAN.
From [Table/Fig-5] it was concluded that the association between abnormal VR and LVDD is statistically significant with a p-value of <0.001**. One study evaluated heart rate response to Valsalva manoeuver in 132 type II diabetic patients [18]. Heart rate response was significantly smaller (p<0.001**) in the study group.
From [Table/Fig-6]it was inferred that there is a significant association between LVDD and abnormal heart rate response to standing with a statistically significant p-value being 0.014*. This was in conformity with earlier studies. A study conducted by Caroline et al., in Malta showed a significant association between PTI and LVDD [15].
From [Table/Fig-7] it was inferred that fall in Systolic BP was significantly associated with LVDD with a p-value of 0.011 The finding of the present study was in conformity with earlier studies. A study was conducted on the orthostatic test in patients with impaired glucose tolerance (IGT) and Type II diabetes [18]. The mean cardiovascular autonomic function score was higher in test group (p<0.001**). In another study [22] conducted showed higher incidence of postural hypotension in diabetic patients with autonomic neuropathy.
From [Table/Fig-8] it was concluded that, there was a significant association between LVDD and raise in diastolic blood pressure with a p-value of <0.001**. The mean raise in diastolic BP in patients with LVDD is 10.97 + 5.7 mmHg and in patients without LVDD is 16.29 + 3.51 mmHg. The finding of the present study is in conformity with earlier studies. In another study [24], found a decrease in cardiovascular response to sustained handgrip test in diabetic patients.
There was a strongly significant association between LVDD and Ewing’s score with a p-value of <0.001**[Table/Fig-9].
Hence, diabetic patients with LVDD can be concluded to have CAN.
| Test Parameter | Criteria Category | | Score |
|---|
| Deep breathing test (DBT) | Delta heart rate (bpm) | > 1 5 Normal | 0 |
| 11–14 Borderline | 0.5 |
| < 1 0 Abnormal | 1 |
| Valsalva maneuvre (VM) | Valsalva ratio (VR) | > 1.21 Normal | 0 |
| 1.11–1.20 Borderline | 0.5 |
| < 1.1 0 Abnormal | 1 |
| Handgrip test (HGT) | Change in DBP | > 16 Normal | 0 |
| 11–15 Borderline | 0.5 |
| < 1 0 Abnormal | 1 |
| Lying to standing test | Fall in SBP | < 10 Normal | 0 |
| 11–20 Borderline | 0.5 |
| > 20 Abnormal | 1 |
| 30:15 ratio/ PTI index | Change in HR | > 1 . 0 4 Normal | 0 |
| 1.01–1.03 Borderline | 0.5 |
| <1.0 1 Abnormal | 1 |
Age and Gender Distribution among patients and its association with LVDD and Ewings score
| Age in years | Total | Male | Female | LVDD | Positive Ewing’s score |
|---|
| 35-45 years | 14(14%) | 8(11.1%) | 6(21.4%) | 3(9.37%) | 2(6.67%) |
| 46-55 years | 45(45%) | 29(40.3%) | 16(57.1%) | 12(37.5%) | 11(36.67%) |
| 56-65 years | 41(41%) | 35(48.6%) | 6(21.4%) | 15(46.87%) | 17(56.67%) |
| Total | 100(100%) | 72(100%) | 28(100%) | 32(100%) | 30(100%) |
Inference Higher age is positively associated with presence of LVDD with p=0.102+ and with positive Ewing’s score with p = 0.09+
Distribution of symptoms among patients
Study of Delta Heart Rate among patients and its association with LVDD
| LVDD |
|---|
| Yes | No | Total |
|---|
| DHR | Normal | 12 | 41 | 53 |
| Abnormal | 20 | 27 | 47 |
| Total | | 32 | 68 | 100 |
Study of Valsalva ratio (VR) and its association with LVDD
| LVDD | Total |
|---|
| Yes | No |
|---|
| VP | Normal | 14 | 64 | 78 |
| Abnormal | 18 | 4 | 22 |
| Total | 32 | 68 | 100 |
Study of postural tachycardia index (PTI) and its association with LVDD
| LVDD | Total |
|---|
| Yes | No |
|---|
| PTI | Normal | 15 | 49 | 64 |
| Abnormal | 17 | 19 | 36 |
| Total | | 32 | 68 | 100 |
Study of fall in SBP and its association with LVDD
| LVDD | Total |
|---|
| Yes | No |
|---|
| FALL in SBP | Normal | 26 | 65 | 91 |
| Abnormal | 6 | 3 | 9 |
| Total | | 32 | 68 | 100 |
Study of raise in DBP and its association with LVDD
| LVDD | Total |
|---|
| Yes | No |
|---|
| Raise in DBP | Normal | 18 | 67 | 85 |
| Abnormal | 14 | 1 | 15 |
| Total | | 32 | 68 | 100 |
Study of Ewing’s score and its association with LVDD
| LVDD |
|---|
| Yes | No | Total |
|---|
| Ewings Score | Normal | 7 | 63 | 70 |
| Abnormal | 25 | 5 | 30 |
| Total | | 32 | 68 | 100 |
Conclusion
Positive Ewing’s score was strongly associated with LVDD in patients with Type 2 Diabetes Mellitus in this study with a p-value of <0.001**. Positive Ewing’s score suggests that patients are having CAN. LVDD is the earliest precursor of diabetic cardiomyopathy. In this study there was a significant association between Ewing’s score and LVDD. So, from this study, we can conclude that Type 2 diabetic patients with LVDD will have CAN and hence are at increased risk of sudden cardiac death. As bedside tests for the diagnosis of CAN are cumbersome, patients with LVDD can be concluded to have CAN.
Abbreviations
+ - Suggestive significance (p-value: 0.05<p<0.10).
* - Moderately significant (p-value: 0.01<p ≤ 0.05).
** - Strongly significant (p-value: p≤0.01).
Inference Higher age is positively associated with presence of LVDD with p=0.102+ and with positive Ewing’s score with p = 0.09+
[1]. WHO: world health organization 2013(last updated May 2013, Citied May 2013) http://www.who.int/en/ [Google Scholar]
[2]. RM Anjana, R Pradeepa, M Deepa, ICMR-INDIAB Collaborative Study Group: Prevalence of diabetes and prediabetes in rural and urban India: Phase 1 results of the Indian Council of Medical Research-INdiaDIABetes (INDIAB) studyDiabetologia 2011 54:3022-27. [Google Scholar]
[3]. Pop-Basu Rodica, Cardiac Autonomic Neuropathy in Diabetes: A clinical perspectiveDiabetes care 2010 33(2):434-41. [Google Scholar]
[4]. Diabetes Control and Complications Trial Research Group. The effect of intensive diabetes therapy on measures of autonomic nervous system functions in the Diabetes Control and Complications Trial (DCCT). Diabetologia 1998 41:416-23. [Google Scholar]
[5]. WR Kennedy, X Navarro, DE Sutherland, Neuropathy profile of diabetic patients in a pancreas transplantation programNeurology 1995 45:773-80. [Google Scholar]
[6]. W Dinh, R Füth, M Lankisch, L Bansemir, Cardiovascular autonomic neuropathy contributes to left ventricular diastolic dysfunction in subjects with Type 2 diabetes and impaired glucose tolerance undergoing coronary angiographyDiabet Med 2011 28(3):311-18. [Google Scholar]
[7]. AI Vinik, RE Maser, BD Mitchell, R Freeman, Diabetic autonomic neuropathyDiabetes Care 2003 26:1553-79. [Google Scholar]
[8]. TP Didangelos, GA Arsos, DT Karamitsos, VG Athyros, ND Karatzas, Left ventricular systolic and diastolic function in normotensive type 1 diabetic patients with or without autonomic neuropathy: a radionuclide ventriculography studyDiabetes Care 2003 26:1955-60. [Google Scholar]
[9]. M Ansari, M Alexander, A Tutar, BM Massie, Incident cases of heart failure in a community cohort: importance and outcomes of patients with preserved systolic functionAm Heart J 2003 146:115-20. [Google Scholar]
[10]. DJ Ewing, CN Martyn, RJ Young, BF Clarke, The value of cardiovascular function tests: 10 years experience in diabetesDiabetes Care 1985 8:491-98. [Google Scholar]
[11]. Rosner Bernard, Fundamentals of BiostatisticsTeratology 2000 5th EditionDuxbury:80-240. [Google Scholar]
[12]. Riffenburg Robert H, Statistics in Medicine 2005 Second EditionAcademic press:85-125. [Google Scholar]
[13]. PSS Sunder Rao, J Richard, An Introduction to Biostatistics, A manual for students in health sciencesTetracyclineTeratology 2006 4th EditionNew DelhiPrentice hall of India:86-160. [Google Scholar]
[14]. KP Suresh, S Chandrasekhar, Sample Size estimation and Power analysis for Clinical research studiesJournal Human Reproduction Science 2012 5(1):7-13. [Google Scholar]
[15]. Caroline LVDD & cardiovascular autonomic neuropathy in type 2 DM. Poster presented at Department of Diabetes and Endocrine centre, Malta dei hospital, University of Malta, Malta. Accessed from http://spo.escardio.org/eslides/view.aspx?eevtid=48&fp=P5002 Accessed on January 2012. [Google Scholar]
[16]. Vinik Aaron I, Maser Raelene E, Mitchell Braxton D, Freeman Roy, Diabetic Autonomic NeuropathyDiabetes Care 2003 26(5):1553-79. [Google Scholar]
[17]. Pappachan JM, Sebastian J, Bino BC, Cardiac Autonomic Neuropathy in Diabetes Mellitus: prevalence, risk factors and utility of Corrected QT interval in the ECG for its Diagnosis, Kottayam Medical College, South India. Melaka Manipal Medical College, Malaysia. 88. Rundle RWDiabetic neuropathy. Medicine (Baltimore) 1945 24:111-60. [Google Scholar]
[18]. Goel A, Agarwal Ruchika, Singla S, Lakhani KK, Sonigra DT, Agarwal SB, A clinical study on Autonomic nervous system manifestations in Diabetes mellitusThe Journal of the Association of Physicians of India 2005 53:999 [Google Scholar]
[19]. NK Subbalakshmi, PMR Adhikari, A Rajeev, Independent predictors of cardiac parasympathetic dysfunction in type 2 diabetes mellitusSingapore Med J 2008 49(2):121 [Google Scholar]
[20]. M Lakhotia, PKD Shah, R Vyas, SS Jain, A Yadav, MK Parihar, Clinical Dysautonomia in Diabetes Mellitus- A Study with Seven Autonomic Reflex Function TestsJAPI 1997 45(4):271-74. [Google Scholar]
[21]. JL Noronha, SD Bhandarkar, PN Shenoy, VJ Retnam, Autonomic Neuropathy in Diabetes MellitusJ Postgrad Med 1981 27:1-6. [Google Scholar]
[22]. TS Purewal, PJ Watkins, Postural hypotension in diabetic autonomic neuropathy: a ReviewDiabet Med 1995 12:192-200. [Google Scholar]
[23]. RW Rundles, Diabetic neuropathy – general review with report of 125 casesMedicine 1945 24:111-60. [Google Scholar]
[24]. T Dyrberg, Prevalence of diabetic autonomic neuropathy measured by simple bedside testsDiabetologia 1981 20:190-94. [Google Scholar]