Diagnostic Dilemma in Cornual Pregnancy- 3D Ultrasonography may Aid!!
Nilanchali Singh1, Reva Tripathi2, YM Mala3, Atul Batra4
1Senior Resident, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
2Director Professor and Head of Department, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
3Professor, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
4Intern, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nilanchali Singh, Senior Resident, Department of Obstetrics & Gynaecology, Maulana Azad Medical College and Lok Nayak Hospital, Bahadur Shah Zafar Marg, New Delhi-110002, India.
E-mail: nilanchalisingh@gmail.com
Interstitial or cornual pregnancy is a rare and dangerous type of ectopic gestation. It poses a diagnostic difficulty and differentiating from eccentrically located intrauterine pregnancy may be challenging. We are reporting a case of nulliparous woman diagnosed as having interstitial pregnancy on three-dimensional ultrasonography. We managed the patient successfully with weekly intramuscular doses of methotrexate. The β HCG levels were high throughout the therapy (89,000 to 1,48,000 IU/ml). The patient was admitted throughout the course of treatment. After three doses of methotrexate, the β-HCG levels began to fall. Weekly monitoring was done thereafter till normal values of β-HCG were reported. Early and prompt diagnosis and treatment of interstitial pregnancy is important to prevent catastrophic hemorrhagic complications. Three-dimensional sonography is an important diagnostic tool as it may impart better anatomical orientation and precise location of the gestational sac as compared to other imaging modalities. Methotrexate therapy may be considered in selected cases.
Cornual pregnancy, Interstitial pregnancy, Medical management, Three-dimensional sonography
Case Report
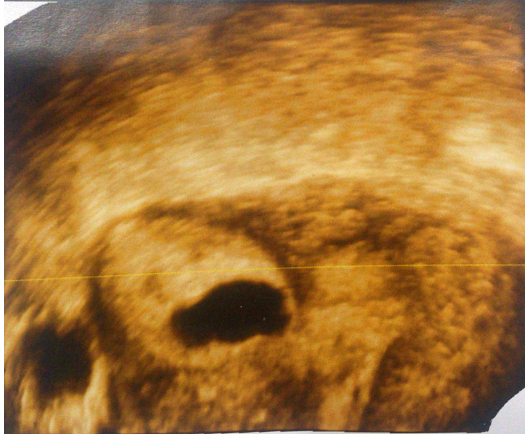
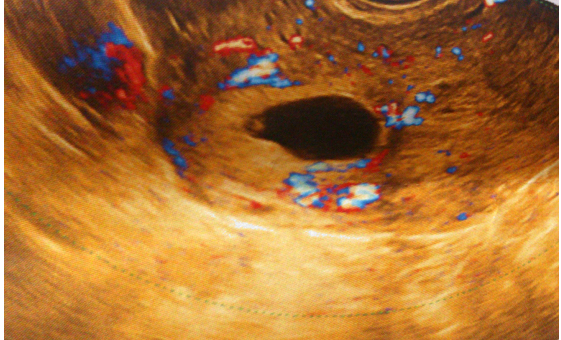
A 30-year-old, nullipara, presented with two months amenorrhea, mild abdominal pain and spotting since three days. She had spontaneous conception. General physical examination was normal. Mild tenderness in suprapubic area was present. Pelvic examination revealed bulky uterus without any adnexal pathology. The presence of cervical motion tenderness was doubtful.Urine pregnancy test was positive. Clinical features were suggestive of either ectopic pregnancy or threatened abortion. Transvaginal sonography was performed but it could not differentiate whether it is eccentrically located intrauterine gestational sac or cornual pregnancy. Hence, a three dimensional ultrasonography was performed which revealed a well-defined gestational sac in right uterine cornua, embedded in the uterine musculature [Table/Fig-1]. Doppler sonography revealed increased vascularity surrounding the gestational sac [Table/Fig-2]. Uterine cavity was empty and there was no free fluid in the peritoneal cavity. A diagnosis of cornual ectopic pregnancy was made. β-HCG levels were 89,000 IU/ml.
Treatment and follow-up
We wanted to give a trial of methotrexate therapy to the patient despite the fact that methotrexate therapy is usually not indicated in very high βHCG values, as the patient was nullipara and surgeries for cornual pregnancy are complicated. After counseling the patient and her husband regarding pros and cons of methotrexate therapy and surgery, they too opted for methotrexate therapy. Likelihood of requirement of surgery in case of failed medical management was explained. The patient was admitted for proper monitoring. Baseline renal and liver function tests were normal. Methotrexate 60 mg was administered intramuscularly as her weight was 60 kgs. β HCG levels were repeated on day-4 and day-7 and levels were 96,000 IU/ml and 1,20,000 IU/ml. Second dose of methotrexate (60 mg IM) was repeated on day 7. β HCG levels were repeated one week later and the levels were 1,48,000 IU/ml. Third dose methotrexate (same dose) was repeated. One week after receiving the third dose, the β HCG reported the fall in value i.e. 1,08,000 IU/ml. The patient remained admitted for three weeks and was discharged once the β HCG levels started decreasing.The patient had weekly serum β HCG levels monitoring, which showed a falling trend. After 12 weeks of methotrexate therapy, the β HCG level was 2.2 IU/ml. The patient remained asymptomatic during the follow-up. A repeat scan after 12 weeks showed a normal uterine cavity. The patient menstruated after two weeks of methotrexate therapy and had two normal cycles thereafter during her follow-up. She was using barrier method for contraception. The patient continues to be under regular follow-up.
Discussion
Interstitial or cornual pregnancy accounts for 1 to 3% of all ectopic pregnancies [1,2]. Mortality rate has been reported to be upto 2% [3]. It is the most hazardous type of ectopic gestation as it may not be diagnosed till late gestation due to corneal distensibility and its rupture at late gestation may lead to massive hemorrhage.Hemorrhage is also severe due to increased vascular supply in cornua.
Cornual pregnancies pose a diagnostic and therapeutic challenge. Diagnosis of interstitial pregnancy is done by ultrasound and sometimes, by laparoscopy. Ultrasonography may reveal gestational sac located in uterine cornua and surrounded by thin myometrial rim with increased vascularity [4]. Eccentrically located, intrauterine gestational sac can be misinterpreted as interstitial pregnancy on ultrasound evaluation. To distinguish between these two, a sonographic criterion can be utilized. According to this criteria, empty uterine cavity; separately seen gestational sac; sac <1 cm from the most lateral edge of the uterine cavity and; a thin myometrial layer surrounding the sac [5]. In our patient, two dimensional ultrasonography could not clearly elucidate the location of gestational sac, hence a three dimensional sonography was performed which confirmed the diagnosis.
The treatment traditionally described for interstitial pregnancy is laparotomy, hysterectomy and cornual resection, which is associated with high complication rates and increased morbidity. Laparoscopic resection of cornua is an alternative treatment [1]. Single dose or multiple dose methotrexate therapy has also been reported with successful outcome [2,6]; though high failure rates have been reported [7]. There is no consensus on dose or number of methotrexate injections for interstitial pregnancies. Intravenous and intra-amniotic methotrexate therapies have also been reported with successful outcome [6,8]. Usually, high β HCG levels are considered to be relative contraindication of medical management but in our patient, we chose this line of management as patient was a nullipara and was hemodynamically stable. She was willing for follow-up throughout the course of treatment
Various studies on interstitial pregnancy report the benefit of methotrexate therapy in cornual pregnancy but also emphasize on the need for monitoring, admission and follow-up [4,6]. Monitoring in these patients is very important, considering the catastrophic outcome that may follow rupture, despite commencement of medical therapy.
Three-dimensional ultrasonography of the uterus showing gestational sac embedded in the right cornua. Uterine cavity and musculature are also seen clearly
Doppler sonography showing increased vascularity surrounding the gestational sac in the cornua
Conclusion
Three-dimensional sonography is an important imaging modality in diagnosis of cornual pregnancy as it may depict precise location of the gestational sac differentiating it from eccentrically located gestational sac. Prompt diagnosis and management may be life saving. Methotrexate therapy may be considered in selected cases.
Learning Points
Diagnosis of cornual pregnancy may be difficult on ultrasonography as it may be confused with eccentrically located intrauterine pregnancy. Three-dimentional ultrasonography may aid in diagnosis. Methotraxate therapy may be useful but proper selection of patient is mandatory. Monitoring and follow-up is very important as rupture may occur even after commencement of medical therapy
[1]. M Vicino, G Loverro, L Resta, S Bettocchi, A Vimercati, L Selvaggi, Laparoscopic cornual excision in a viable large interstitial pregnancy without blood flow detected by color Doppler ultrasonographyFertil Steril 2000 74(2):407-09. [Google Scholar]
[2]. S Dilbaz, B Katas, B Demir, B Dilbaz, Treating cornual ectopic pregnancy with a single methotrexate injectionJ Reprod Med 2005 50(2):141-43. [Google Scholar]
[3]. MT Lau, HP Tulandi, Conservative medical and surgical management of interstitial ectopic pregnancyFertil Steril 1999 72:207-15. [Google Scholar]
[4]. A P Advincula, S Senapati, Interstitial pregnancyFertil Steril 2004 82(6):1660-62. [Google Scholar]
[5]. IE Timor-Tritsch, A Monteagudo, C Matera, CR Veit, Sonographic evolution of cornual pregnancies treated without surgeryObstet Gynecol 1992 79:1044-49. [Google Scholar]
[6]. J D Fisch, B Ortiz, S Tazuke, U Chitkara, L Giudice, Medical management of interstitial ectopic pregnancy: a case report and literature reviewHum Reprod 1998 13(7):1981-86. [Google Scholar]
[7]. K Barnhart, S Spandorfer, C Coutifaris, Medical treatment of interstitial pregnancy. A report of three unsuccessful casesJ Reprod Med 1997 42:521-24. [Google Scholar]
[8]. A Al-Khan, R Jones, D Fricchione, J Appuzio, Intravenous methotrexate for the treatment of interstitial pregnancyJ Reprod Med 2004 49:121-22. [Google Scholar]