Facial asymmetry can be caused by various pathological conditions, condylar hyperplasia (CH) is one of such condition, characterized by unilateral or bilateral mandibular condylar overgrowth, causing facial asymmetry, mandibular deviation, malocclusion and functional impairment. Advanced imaging and scintigraphic methods, helps the clinicians in diagnosing and monitoring its macroscopic aspects. Here we report three interesting and illustrative cases of facial asymmetry with unilateral CH discussing the unusual changes in the facial bones.
Condylar overgrowth, Imaging, Mandibular deviation, Unilateral
Case Report
Case 1
A 30-year-old male patient came to the dental OPD with a chief complaint of slowly progressing facial asymmetry following a facial trauma three years back. On inspection facial asymmetry was evident due to elongation of right lower half of the face with the mandible deviated towards the left side. The prominence of chin appeared shifted towards the left side. On palpation all inspectory findings were confirmed, condylar movements appeared limited on the right side. A non tender bony prominence was appreciated in the pre auricular region during mandibular movements. On examination, the right condylar enlargement resulted in facial asymmetry, elongation of right lower half of the face shifting the chin prominence to the left side, and limited movements on the right side. Based on the history and clinical findings the provisional diagnosis of unilateral CH of right side was made. Patient’s consent for clinical pictures could not be obtained.
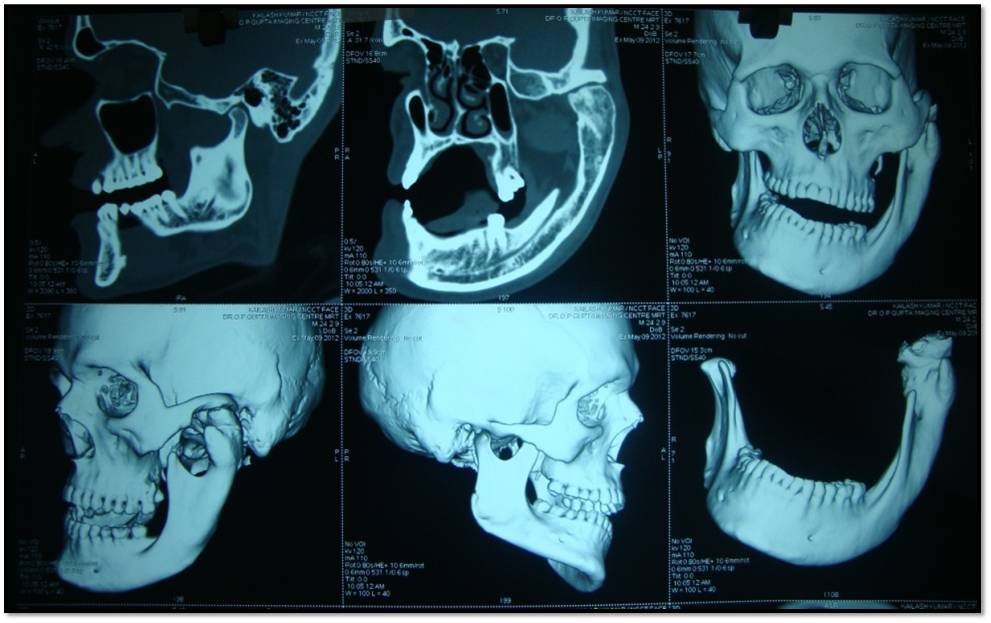
Radiographic evaluation by panoramic and conventional tomographic views revealed an enlarged bulky, right condylar head with a thick condylar neck. The ramus appeared elongated and the lower border of the right side of mandible was thickened. Computed tomography (CT) and 3 Dimensional (3D) CT scan findings supported the clinical diagnosis [Table/Fig-1]. Radionuclide bone scan was performed following intravenous injection of 20 mCi of 99m TcMDP (technetium methylene diphosphonate). Planar and SPECT images showed unilateral increased tracer uptake in the right mandibular condyle [Table/Fig-2]. After performing all routine blood investigations which were within the normal range, right condylectomy was performed and histopathology of the specimen confirmed the diagnosis of condylar hyperplasia. A second surgery of osteotomy of the mandible was planned for esthetic reasons.
Case 2
A 24-year-old male came with a chief complaint of gross facial asymmetry since childhood, which had gradually increased in size and then ceased at about 18 years of age. On extra-oral examination facial asymmetry, deviation of chin to the right side, protruded chin and restricted mouth opening were recorded [Table/Fig-3]. Intraoral examination showed deranged occlusion, open bite, midline shift, and increase anteroposterior and mediolateral dimensions of the right side upper and lower dental arches which were recorded on the diagnostic casts. Hence, a clinical diagnosis of left unilateral CH was made. Panoramic radiographic examination revealed outward bowing of the mandibular body, elongation of body and ramus, increased antero-posterior thickness of body, accentuated left gonial angle. Left condyle was found to be enlarged, elongated multilobulated, with increase in the cortical thickness [Table/Fig-4]. CT confirmed marked hypertrophy, broadening and enlargement of left mandibular condyle with sclerotic changes. Interestingly the left mandibular condyle revealed multilobulated appearance [Table/Fig-5]. The cortical outlines were well-defined but the articular margins showed sclerotic changes. The left articular fossa appeared broad, wide with sclerotic margins compated to the contralateral side. The maxilla on the left side was anteroposteriorly and mediolaterally larger than the contralateral side. The trabeculae on the affected side were thickened. Nasal septum appeared mildly deviated towards the right side. A normal serum calcium and alkaline phosphatase level suggested absence of any bony disorder further supporting the diagnosis of condylar hyperplasia.
Case 3
A 25-year-old male came concerned about facial asymmetry since last 10 years. Extra-oral examination revealed facial asymmetry attributed due to deviation of midline towards the right side with protruded chin [Table/Fig-6]. Condylar movement was affected on both right and left side. There was a marked increase in the size of mandibular ramus and body on the left side. Intraoral examination showed deranged occlusion, posterior open bite on the affected side and class II molar relationship on the contralateral side along with midline shift and anterior deep bite. Hence, a provisional diagnosis of left unilateral CH was made. Radiographic examination supported the clinical findings and revealed outward bowing of the body of mandible, elongation of the mandibular ramus and body, increased antero-posterior thickness of mandibular body with an accentuated gonial angle on the left side [Table/Fig-7]. Therefore, a diagnosis of left CH was made.
Discussion
Mandibular CH is a rare disease first described in 1836 as an overgrowth of the mandibular condyle, unilaterally or bilaterally, leading to facial asymmetry, mandibular deviation, malocclusion and articular dysfunction as seen with the present case [1,2]. This disorder is self-limiting, but as long as it remains active, asymmetry and occlusal changes will remain progressive [1,2]. Clinically, unilateral CH presents with deviation of chin to the unaffected side, increase in the vertical dimension of mandibular ramus and body, posterior open bite on the affected side, limited and/or deviated mouth opening [2]. If deformity occurs before growth is complete, the occlusal plane usually becomes slanted for dental compensation, whereas posterior open bite is attributed to deformity occurring after completion of growth [2].
Epidemiologically, CH shows similar incidence amongst males and females, and various ethnic groups. It mainly manifests itself in patients with ages ranging 11-30 years, showing no predilection for either left or right side [1,3]. The etiology of CH is controversial and not well understood. Excessive proliferation in response to an infection, repair especially after trauma, abnormal loading have been suggested as causes leading to CH [1,3]. A plethora of other presumed causes are hormonal disturbances, partial hemihypertrophy, arthrosis, osteochondromatosis, local circulating disturbances or neurotropic disturbances [2,3]. Our first patient had given a history of trauma, the second and third cases presented with left CH due to an unknown etiology.
An accurate diagnosis is essential for a suitable treatment plan. Sequential study models, radiological and scintigraphic methods are commonly used for diagnosis and monitoring of its macroscopic aspects [4-6]. Lateral and postero anterior cephalograms, transcranial and panoramic radiographs should be evaluated for various changes in the facial bones on the affected side including the maxilla and mandible. Enlarged condylar head, increased length of condylar head, condylar neck, mandibular body and ramus on the affected side, accentuated gonial angle, characteristic depression of the inferior mandibular border at the midline where the enlarged side joins the contralateral normal mandible are appreciated [4]. A compensatory enlargement of maxilla and widening of the glenoid fossa usually at the expense of the posterior slope of the articular eminence are evident. Occlusal changes like posterior openbite or crossbite are also reported. Our findings were in concurrence with those reported in the previous literature except for the unique multilobulated appearance of condylar head, and sclerosis of the bone below the articulating surfaces in the second case which were found to be unusual. A PUB MED search revealed no such case reported till date. These modifications may be attributed to the adaptations happening during the growth and the increased masticatory load following the enlargement.
CT is useful in distinguishing the CH from neoplasia, by showing a generalized bone growth in the former and localized in the later, which is then confirmed by a biopsy [4-5].
Besides these, Bone scintigraphy with Tc pyrophosphate 99, is an auxiliary diagnostic method that has proven effective in monitoring bone growth by identifying areas of increased osteoblastic activity [2,6-7]. In the present case, Planar and SPECT images showed asymmetrical, unilateral increased tracer uptake in the right mandibular condyle suggesting active condylar hyperplasia.
Progressive facial asymmetry due to unilateral CH must be differentiated from other states of overdevelopment like hemifacial hypertrophy (unilateral enlargement of all hard and soft tissues of face), unilateral macrognathia (unilateral mandibular hypertrophy, which is a three dimensional enlargement of mandible, including condyles, ramus and ends at midline of symphysis) and laterognathia (asymmetrical prognathism where both condyles are equal in size) [7]. Chondroma and osteochondroma may produce similar symptoms and signs, but they are often localized, grow more rapidly and may cause even greater asymmetric condylar enlargement [1,2,4].
Treatment depends on age, degree of deformity and dysfunction which usually includes condylectomy during the period of active growth. If growth has stopped, orthodontics and surgical mandibular repositioning are indicated. If the height of the mandibular body is greatly increased, facial symmetry can be further improved by reducing the inferior border by osteotomies [2,8].
Axial CT section showing right condylar hyperplasia

SPECT showing asymmetrical, unilateral increased tracer uptake in the right condyle,

Profile picture showing facial asymmetry due to left condylar hyperplasia

Pictorial presentation of changes in facial bones associated with condylar hyperplasia; A-Enlarged condylar head, multilobulated; B-Widening of the glenoid fossa; C-Outer bowing of the inferior mandibular border and increased cortical thickness; D-Shifting of the midline to the opposite side and Notching of the inferior border at the midline; E-Increased height of the mandible; F-Increased height of the maxilla as a result of compensatory enlargement of maxilla; G-Increase in ramal height; H-Increased length and width of condylar neck; I-Increased gonial angle ; J-Inferior positioning of the mandibular canal; K-Posterior open bite on the affected side; L-Deviated nasal septum

CT section along with 3D Reconstruction showing multilobulated appearance of left condylar head,
Extraoral picture showing facial asymmetry attributed to deviation of midline towards the right side with protruded chin,

OPG revealing outward bowing of the body of mandible, elongation of the mandibular ramus and body, increased antero-posterior thickness of mandibular body with an accentuated gonial angle on the left side

Conclusion
CH is a rare disease causing dental and facial deformity. A thorough history, clinical examination, along with conventional and interventional radiology plays a vital role in differentiating it from other similar conditions. A correct diagnosis initiates an effective treatment plan for both aesthetic and functional rehabilitation.
[1]. W Neville Brad, D Damm Douglas, M Allen Carl, E Bouquot Jerry, Textbook of Oral and Maxillofacial Pathology 2001 2nd EditionPhiladelphia W.B. Saunders:16 [Google Scholar]
[2]. D Mehrotra, S Dhasmana, M Kamboj, G Gambhir, Condylar hyperplasia and facial asymmetry: Report of five casesJ Maxillofac Oral Surg 2011 10:50-6. [Google Scholar]
[3]. D Nitzan, A Katsnelson, I Bermanis, The clinical characteristics of condylar hyperplasia: Experience with 61 patientsJ Oral Maxillofac Surg 2008 66:312-18. [Google Scholar]
[4]. C White Stuart, MJ Pharoah, Textbook Oral RadiologyTetracyclineTeratology 2007 5th EditionMarylandMosby:550 [Google Scholar]
[5]. Y Mutoh, Y Ohashi, N Uchiyama, K Teradak, K Hanada, F Sasaki, Three dimensional analysis of condylar hyperplasia with computed tomographyJ Craniomaxillofac Surg 1991 19:49-55. [Google Scholar]
[6]. SC Hodder, JI Rees, TB Oliver, PE Facey, AW Sugar, SPECT bone scintigraphy in the diagnosis and management of mandibular condylar hyperplasiaBr J Oral Maxillofac Surg 2000 38:87-93. [Google Scholar]
[7]. CP Saridin, P Raijmakers, AG Becking, Quantitative analysis of planar bone scintigraphy in patients with unilateral condylar hyperplasiaOral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 104:259-63. [Google Scholar]
[8]. A Silvestri, V Incisivo, G Mariani, Treatment of mandibular condylar hyperplasia in developmental age: Clinical caseMinerva Stomatol 2000 49:501-10. [Google Scholar]