Introduction
Tooth impaction can be defined as the infraosseous position of the tooth after the expected time of eruption, whereas the anomalous infraosseous position of the canine before the expected time of eruption can be defined as a displacement. Most of the time, palatal displacement of the maxillary canine results in impaction [1]. However, it is possible to prevent possible maxillary canine impaction by recognizing the tooth displacements early. GPS i.e. Global Positioning Satellite provides us location and the necessary information anywhere on the earth; similarly this article will guide us about different methods involved in localizing the canine that has lost its path during eruption.
After the third molar, the most frequently impacted tooth is the maxillary canine. Ericson and Kurol estimated the incidence at 1.7%. Impactions are twice as common in females (1.17%) as in males (0.51%). Of all patients with maxillary impacted canines, it is estimated that 8% have bilateral impactions. The incidence of mandibular canine impaction is 0.35%.; the prevalence of impacted maxillary canine ranges from a minimum of 0.92% to a maximum of 4.3% [2].
According to Dewel [3,4], maxillary canines have the longest period of development, as well as the longest and most tortuous course to travel from the point of formation, lateral to the piriform fossa, until they reach their final destination in full occlusion. Moss [5] states that the canine remains high in the maxilla just above the root of the lateral incisor until the crown is calcified. It then erupts along the distal surface of lateral incisor resulting in closure of the physiological diastema if present and correction of the so called ugly duckling dentition [4,6].
Aetiology
In general, the causes for retarded eruption of teeth may be either generalized or localized [4,7,8]. More recently, the absence of the maxillary lateral incisor and variation in the root size of the tooth, as well as variation in the timing of its root formation, have been implicated as important etiologic factors associated with canine impaction [4,9-11]. It seems that the presence of the lateral incisor root with the right length, formed at the right time, is an important variable needed to guide the mesially erupting canine in a more favourable distal and incisal direction. Becker et al., [11] reported an increase of 2.4 times in the incidence of palatally impacted canines adjacent to the sites of missing lateral incisors as compared with the general population. Two main theories have been proposed to explain the occurrence of palatally displaced maxillary canines: the “guidance theory” [10,12,13] and the “genetic theory” [14,15].
Interception of canine impaction
The most critical point in the prevention of possible maxillary canine impaction is the ability to recognize the tooth displacement early and to predict the subsequent failure of eruption. The average age when a maxillary canine should erupt is 13 y in boys and 12 y and 3 mnth in girls [4]. So, the ability to diagnose canine displacement in the early mixed dentition (average age of 8 y) and to prevent impaction of the canine would be extremely useful for the clinician. The best time to begin assessing potential impaction is during the early mixed dentition period, because the early diagnosis of one dental anomaly may indicate an increased risk for later appearance of others [2,15].
Localization of maxillary canine
Localisation of maxillary canine is based on both clinical and radiographic examination
Clinical evaluation: It has been suggested that the following clinical signs might be indicative of canine impaction: (1) delayed eruption of the permanent canine or prolonged retention of the deciduous canine beyond 14 to 15 y of age, (2) absence of a normal labial canine bulge, in other words, either inability to locate canine position through intraoral palpation of the alveolar process or the presence of an asymmetry in the canine bulge noted during alveolar palpation, (3) presence of a palatal bulge, and (4) delayed eruption, distal tipping, or migration of the lateral incisor [4].
According to Ericson and Kurol [16], the absence of the "canine bulge" at earlier ages should not be considered as indicative of canine impaction. In their evaluation of 505 schoolchildren between 10 and 12 y of age, they found that 29% of the children had nonpalpable canines at 10 y, but only 5% at 11 y, whereas at later ages only 3% had non-palpable canines. Therefore, for an accurate diagnosis the clinical examination should be supplemented with a radiographic evaluation.
Radiographic Assessment: The proper localization of the unerupted maxillary canine plays a crucial role. It can help to recognize the tooth displacement in mixed dentition to prevent subsequent impaction. It also aids in determining the feasibility as well as the proper access for the surgical approach and the proper direction for the application of orthodontic force. Various radiographic exposures, including panoramic views, periapical view, occlusal films, posteroanterior views and lateral cephalogram can help in evaluating the position of the canines. However, all these techniques help to visualise the tooth in 2-dimensions. So, 3-dimensional radiographic techniques including Computed Tomography (CT), Spiral CT, Cone Beam Computed Tomography (CBCT) were introduced [17].
Following are the aids to localise the erupting canines:-
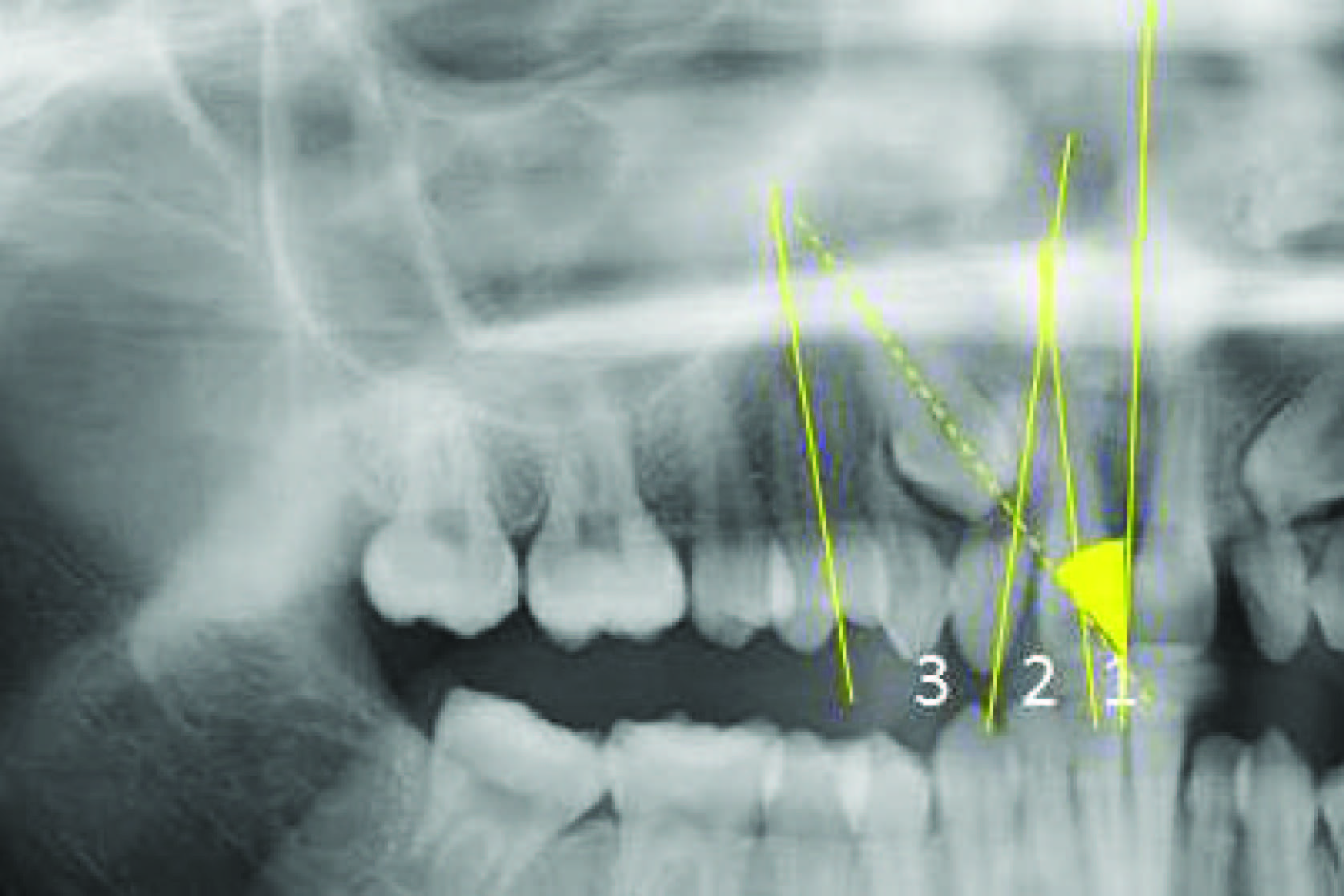
1. Panoramic Radiographs: Ericson and Kurol [18] in 1988 defined number of sectors to denote different types of impaction [Table/Fig-1].
i. Sector 1: if the cusp tip of the canine is between the interincisor median line and the long axis of the central incisor;
ii. Sector 2: if the peak of the cuspid of the canine is between the major axes of the lateral and central;
iii. Sector 3: if the peak of the cuspid of the canine is between the major axis of the lateral and the first premolar.
They used angle α to represent the angle formed between the interincisor midline and long axis of canine and “d” as the perpendicular distance of the peak of the cuspid of the impacted canine with respect to the occlusal plane. Localisation via sector methods has a more prognostic than diagnostic value. The risk of resorption of the root of the lateral incisor increases by 50% if the cusp of the canine belongs to sector 1 or 2 and if α angle is greater than 25°. The duration of treatment is longer if the canine is found in sector 1, shorter if it belongs to sector 3, with respect to sector 2. The necessity of treatment and the degree of treatment difficulty increases as this angle increases.
Linduaer et al., [19] in the year 1992, gave another sector classification and found out that 78% of canine that were destined to get impacted had their cusp tips located in sector II, III, IV. Fernandez et al., [20] in the year 1998 studied the eruption pattern of the canine and found that during eruption; the upper canine increases its inclination mesially, until a maximum angle is reached at approximately 9 y of age. From this inflexion point onwards, the tooth progressively straightens until it emerges above the gingival margin. When the lateral incisor is not yet fully developed, panoramic radiographs more commonly show overlapping of the canine and lateral incisor. In contrast, when lateral incisor development is complete, such overlapping is rare; moreover, the few cases in which it is observed involve a greater mesial inclination of the canine. The overlapping of the canine and lateral incisor in panoramic radiographs when the incisor has completed its development may be a sign of eruptive disorders of the canine, suggesting the adoption of preventive measures to avoid impaction; for example, extraction of the primary canine.
In the year 2003, Warford et al., [21] did a study for predicting the maxillary canine impaction using sectors and angular measurement. He localised the canine according to 4 sectors and measured the angle between the bicondylar line and long axis of canine. He concluded that the probability of canine impaction increases as the angle reduces and the sector increases.
Sudhakar S and Patil K [22] concluded that a single panoramic radiograph can serve as a reliable indicator for determining the bucco-palatal position of the impacted canines when they lie in the middle and coronal zones. When they lie in the apical zone it is recommended to explore their presence with other conventional or advanced imaging modalities.
Katsnelson A [23] et al., in 2010 concluded that panoramic radiographs has a high sensitivity and specificity for determining impacted maxillary canine position, with angulations greater than 65o associated with buccal impactions.
In 2012, Sajani and King [24] gave a reliable method for diagnosis of early diagnosis of unilateral canine impactions. There was a clinically discernible difference of 4 mm at the age of 8 y and beyond between the mean distance of the tip of the impacted canine group and that of the antimere group from the occlusal plane. Furthermore, there was a statistically significant difference at the age of 9 y and beyond between the 2 groups according to the position in different sectors and according to the mean angle made with the midline. Diagnosis of maxillary canine impaction is possible at 8 y of age by using geometric measurements on panoramic radiographs.
2. Periapical Radiographs: They are the simplest radiographs having minimum exposure. They provide us with information regarding state of development of tooth, the presence of follicle, resorption of deciduous tooth.
3. Postero-Anterior Views: Postero-anterior radiography is fundamental for evaluating the medio-lateral position of the canines with respect to a line connecting the inferior borders of the orbits. However, this technique is more useful for carrying out a prognostic evaluation rather than providing a diagnosis of position. This is possible through the evaluation of the angle formed by the long axis of the canine and the transorbital line. The prognosis and the degree of treatment difficulty increase as the angle between the long axis of the canine and the transorbital line decreases [25].
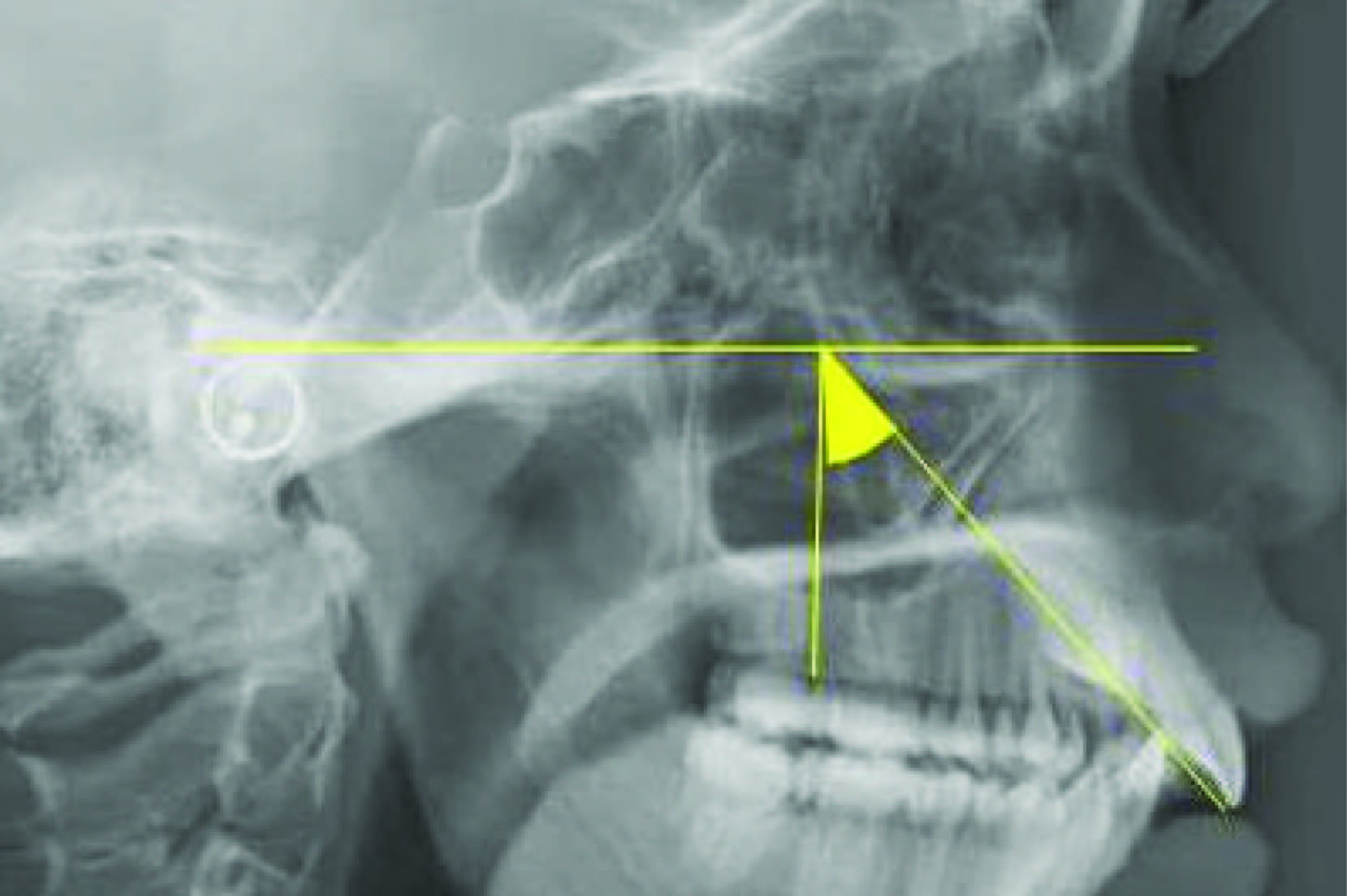
4. Lateral Cephalogram:- If the dental age of the patient is between 8 and 9 y, the upper canines can easily be located by means of laterolateral teleradiography. This technique is useful in establishing the height of the impacted tooth and the anteroposterior position of the cuspid of the impacted canine with respect to the apices of the incisors. This may be indicative to establishing whether the impaction is in palatal or labial position. However, these data may be misleading in the case of bilateral canine impactions due to overlapping images of the two teeth. Evaluation of the impacted canine is carried out by tracing its axis and intersecting it with the perpendicular to Frankfurt’s plane [26]. Various angles can be derived, whose significance from a prognostic point of view is as follows [Table/Fig-2]:
Readings under 10° are considered to be within the norm;
1. between 15 and 25°, the possibility of the necessity of treatment are increased;
2. between 25 and 45°, spontaneous growth is an exception and the difficulties involved in treatment increase;
3. Over 45°, reservations as to the possibilities of treatment success arise.
To assess whether the canine is impacted labial or palatal following radiograph could be of a great aid:
1. Occlusal Radiographs: This may be carried out according to various projections: the most frequently used is that of Simpson (perpendicular beam to the film through the glabella). If, in the image produced by this technique, the cusp of the canine is positioned in front of the ideal line connecting the apices of the lateral incisors, the position will be labial [Table/Fig-3] [27].
2. Clark’s Rule or Parallax Method or Tube Shift Method: Parallax is the apparent displacement of an image relative to the image of a reference object and is caused by an actual change in the angulation of the x-ray beam. The change in angulation of the beam is caused by a change in the x-ray tube position. The reference object is normally the root of an adjacent tooth. Two radiographs of the object are taken. First using the proper technique and angulation as prescribed and the second, radiograph is taken keeping all the parameters constant and equivalent of those of the first radiograph, only changing the direction of the central ray either with a different horizontal angulation or vertical angulation. A tube shift may be carried out in either the horizontal or the vertical plane. If the tooth shifts in the same direction as the tube then the tooth is lingually placed and if it moves in the opposite direction then it is buccally placed (SLOB- same lingual opposite buccal) [28].
Horizontal tube shift: Usually, periapical radiographs (PAS) are used in illustrations of a horizontal tube shift but occlusal radiographs (OR) are superior because they cover a larger area. Therefore, the tube can be moved much more between the two exposures resulting in the shift of the image of the impacted canine being easier to determine as is discussed later. Frequently part or the entire crown or the root of the impacted canine is not captured on one or both periapical radiographs. The radiation dose from two OR is comparable with that from two PAS[29].
Vertical tube shift: In 1986, Keur described a vertical tube shift (VTS) using a rotational panoramic radiograph (PR) and an OR. Because a PR is often taken as an initial radiograph, this combination of radiographs only requires one additional exposure, the OR. The PR tube is actually positioned behind the head at an angle of -7° to the occlusal plane, and the film is in front of the head. However, to aid interpretation of the VTS, the tube can be considered to be in front of the head at an effective angle of +7° [Table/Fig-4a]because the relationship of the image of the canine to the image of the lateral incisor is unaltered. The OR is taken at an angle of +60° to 65° to the occlusal plane [Table/Fig-4b], i.e., there is an effective difference of 53° to 58° between the taking of the two films. The image of the palatally impacted canine that is farther away from the x-ray tube moves in the same direction as the tube [29].
3. Right Angle Technique: The right angle technique uses two radiographs taken at right angles to each other. According to Wraith, Ballard suggested the use of the combination of a lateral cephalometric radiograph with a postero-anterior cephalometric radiograph for localization of impacted maxillary canines. However, the position of the impacted tooth is often difficult to interpret, and an additional intraoral film is required to see the fine detail of the impacted tooth and its surrounding structures. Another combination of radiographs that may be used is a rotational PR and a vertex (axial) or true OR, often supplemented with a periapical radiograph [29].
4. 3-D Techiniques: Because of superimposition of structure on the film it become difficult to distingusish the details which makes the diagnosis and treatment planning difficult with conventional radiographic methods. To be in a position to recommend best line of treatment and to plan appropriate mechanotherapy strategy the orthodontist requires following information-
1. The exact position of the crown and root apex of the impacted tooth and orientation of the long axis.
2. The proximity of the impacted tooth to the roots of the adjacent teeth.
3. The presence of pathology, such as supernumerary teeth, apical granulomas, or cysts, and their relationship with the impacted tooth.
4. The presence of adverse conditions affecting adjacent teeth, including root resorption.
5. The anatomy and position of crown and root [17].
In recent years, CAT scans have become the technique of choice as they supply more realistic information than traditional radiographic methods. CT provides excellent tissue contrast [Table/Fig-5] and eliminates blurring and overlapping of adjacent teeth. Despite its advantages, until now, the use of CT for location of impacted teeth and assessment of resorption has been restricted because of issues related to cost, risk/benefit, access, and expertise in reading the CT. Cone beam Computed Tomography was then introduced which reduces the exposure to radiation[25].
5. Rapid Prototyping: CT studies provide a good visualization of the spatial relationship between anatomical structures. However, even when a 3D reconstruction is obtained, the analysis by the orthodontist and the dental surgeon is still limited: 3D images are seen as 2-dimensional (2D) on film and the computer screen. This limitation can be overcome with the use of CT to make a model by means of rapid prototyping. This technique comprises several technologies that use data from computer-aided design files to produce physical models and devices by a process of material addition [30]. Dental modeling by means of rapid prototyping was an efficient auxiliary method in diagnosis, orthodontic treatment planning, and communication with this patient and the orofacial surgeon. Rapid prototyping technology made possible the fabrication of an attachment for forced canine eruption. Rapid prototyping dental modeling might become the diagnostic procedure of choice in the evaluation of impacted maxillary canines [30].
Sector classification by Ericson and Kurol
Canine position on Lateral Cephalogram
Occlusal radiograph showing labially impacted canine

A) Panoramic radiograph tube effectively at +7 to occlusal plane. Image of incisal tip of palatal canine is projected on film, on film, midway along lateral incisors. B) Tube for maxillary OR is at +60. Image of incisal tip of palatal canine is projected onto apex of lateral incisor i.e. the tooth farther away from tube has moved in the same direction as the tube

3-D imaging of impacted maxillary canine

Conclusion
Recognition of tooth disturbances in early mixed dentition which are genetically associated with canine impaction can aid the clinicians in the early diagnosis of this clinical situation. If the displacement of the canines is detected early, the clinicians should then focus on the means of preventing a possible impaction. Clinically common radiograph used to determine position of impacted canine is occlusal radiograph or Clark’s method using two periapical radiographs, the reason being the ease of availability and assessment. Other supplemental radiographs like OPG, lateral cephalogram etc can be used to decide the prognosis of impacted canine.
[1]. G Litsas, A Acar, A review of early displaced maxillary canines. Etiology, Diagnosis and interceptive treatmentThe Open Dentistry Journal 2011 5:39-47. [Google Scholar]
[2]. S Ericson, J Kurol, Radiographic assessment of canine eruption in children with clinical signs of eruption disturbancesEur J Orthod 1986 8:133-40. [Google Scholar]
[3]. BF Dewel, The upper cuspid: Its development and impactionAngle Orthod 1949 19:79-90. [Google Scholar]
[4]. SE Bishara, Impacted maxillary canines: a reviewAm J Orthod Dentofacial Orthop 1992 101:159-71. [Google Scholar]
[5]. JP Moss, The impacted canineDental Practioner 1972 22:241-48. [Google Scholar]
[6]. BH Broadbent, Ontogenic development of occlusionAngle Orthod 1941 11:224-41. [Google Scholar]
[7]. SE Bishara, DD Kommer, MH McNeil, Management of impacted caninesAM J Og'mot 1976 80:173-90. [Google Scholar]
[8]. RE Moyers, Handbook of orthodontics 1963 Second EditionChicagoYear Book Medicall:83-88. [Google Scholar]
[9]. H Jacoby, The etiology of maxillary canine impactionAm J Orthod 1982 84:125-89. [Google Scholar]
[10]. BH Miller, Influence of congenitally missing teeth on the eruption of upper canineTrans Br Soc Study Orthod 1963 50:17-24. [Google Scholar]
[11]. A Becker, P Smith, R Behar, The incidence of anomalous lateral incisors in relation to palatally displaced cuspidsAngle Orthod 1981 51:24-29. [Google Scholar]
[12]. I Brin, A Becker, M Shalhav, Position of the maxillary permanent canine in relation to anomalous or missing lateral incisors: a population studyEur J Orthod 1986 8:12-16. [Google Scholar]
[13]. PA Mossey, HM Campell, JK Luffingham, The palatal canine and the adjacent lateralincisor: a study of a west of Scotland populationBr J Orthod 1994 21:169-74. [Google Scholar]
[14]. S Peck, L Peck, M Kataja, Site-specificity of tooth maxillary agenesis in subjects with canine malpositionsAngle Orthod 1996 66:473-76. [Google Scholar]
[15]. S Peck, L Peck, M Kataja, Concomitant occurrence of canine malposition and tooth agenesis: evidence of orofacial genetic fieldsAm J Orthod Dentofacial Orthop 2002 122:657-60. [Google Scholar]
[16]. S Ericson, J Kurol, Longitudinal study and analysis of clinical supervision of maxillary canine eruptionCommunity Dent Oral Epidemiol 1986 14:112-16. [Google Scholar]
[17]. S Chaushu, G Chaushu, A Becker, The role of digital volume tomography in the imaging of impacted teethWJO 2004 5:120-32. [Google Scholar]
[18]. S Ericson, J Kurol, Early treatment of palatally erupting maxillary canines by extraction of the primary canines Eur J Orthod 1988 10:283-95. [Google Scholar]
[19]. SJ Lindauer, LK Rubenstein, WM Hang, WC Andersen, RJ Isaacson, Canine impaction identified early with panoramic rasdiographsJ Am Dent Assoc 1992 123:91-97. [Google Scholar]
[20]. E Fernandez, LA Bravo, M Canteras, Eruption of the permanent upper canine: a radiologic studyAm J Orthod Dentofacial Orthop 1998 113:414-20. [Google Scholar]
[21]. JH Warford, RK Grandhi, DE Tira, Prediction of maxillary canine impaction sing sectors and angular measurementAm J Orthod Dentofacial Orthop 2003 124(6):651-55. [Google Scholar]
[22]. S Sudhakar, K Patil, VG Mahima, Localization of impacted permanent maxillary canine using single panoramic radiographIndian J Dent Res 2009 20(3):340-45. [Google Scholar]
[23]. A Katsnelson, WG Flick, Use of panoramic x-ray to determine position of impacted maxillary caninesJ Oral Maxillofac Surg 2010 68(5):996-1000. [Google Scholar]
[24]. AK Sajani, NM King, Early prediction of maxillary canine impaction from panoramic radiographJ Orthod Dentofacial Orthop 2012 142:45-51. [Google Scholar]
[25]. R Manverna, A Gracco, Different diagnostic tools for the localisation of impacted canines: clinical considerations Progress in Orthodontics 2007 8(1):28-44. [Google Scholar]
[26]. HS Orton, MT Garvey, MH Pearson, Extrusion of the ectopic maxillary canine using a lower removable applianceAm J Orthod Dentofacial Orthop 1995 107:349-59. [Google Scholar]
[27]. PW Goatz, SC White, Radiologia odontoiatrica. Principi e interpretazionePadova: Piccin 1986 [Google Scholar]
[28]. CF Clark, A method of ascertaining the relative position of unerupted teeth by means of film radiographsProc R Soc Med Odontol Sectn 1910 3:87-90. [Google Scholar]
[29]. SG Jacobs, Radiographic localisation of unerupted maxillary anterior teeth using the vertical tube shift technique. The history and the application of the methodwith some case reportsAm J Orthod Dentofacial Orthop 1999 116:415-23. [Google Scholar]
[30]. J Faber, J Faber, M Berto, M Quaresmaa, Rapid prototyping as a tool for diagnosis and treatment planning for maxillary canine impactionAm J Orthod Dentofacial Orthop 2006 129:583-89. [Google Scholar]