Ultrasonics: A Novel Approach for Retrieval of Separated Instruments
Harleen Chhina1, Manoj Kumar Hans2, Subhash Chander3
1Post-Graduate Student, Department of Conservative Dentistry & Endodonticsy, Vyas Dental College & Hospital, Jodhpur, Rajasthan, India.
2Associate Professor, Department of Conservative Dentistry & Endodontics, Vyas Dental College & Hospital, Jodhpur, Rajasthan, India.
3Reader, Department of Conservative Dentistry & Endodontics, Vyas Dental College & Hospital, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manoj Kumar Hans, Associate Professor, Department of Conservative Dentistry & Endodontics, Vyas Dental College & Hospital, Near Kudi Haud, NH-65 Pali Road, Jodhpur, Rajasthan, India.
E-mail: hansie51@yahoo.com
An instrument fracture within the root canal interferes and hinders the outcome of the successful root canal treatment. Fracture of endodontic instrument often results from incorrect use or overuse. This article reports a case of retrieval of separated endodontic instrument with help of ultrasonic and discusses the factors influencing the removal of fractured instrument.
Hero shapers, Retrieval, Ultrasonic
Case Report
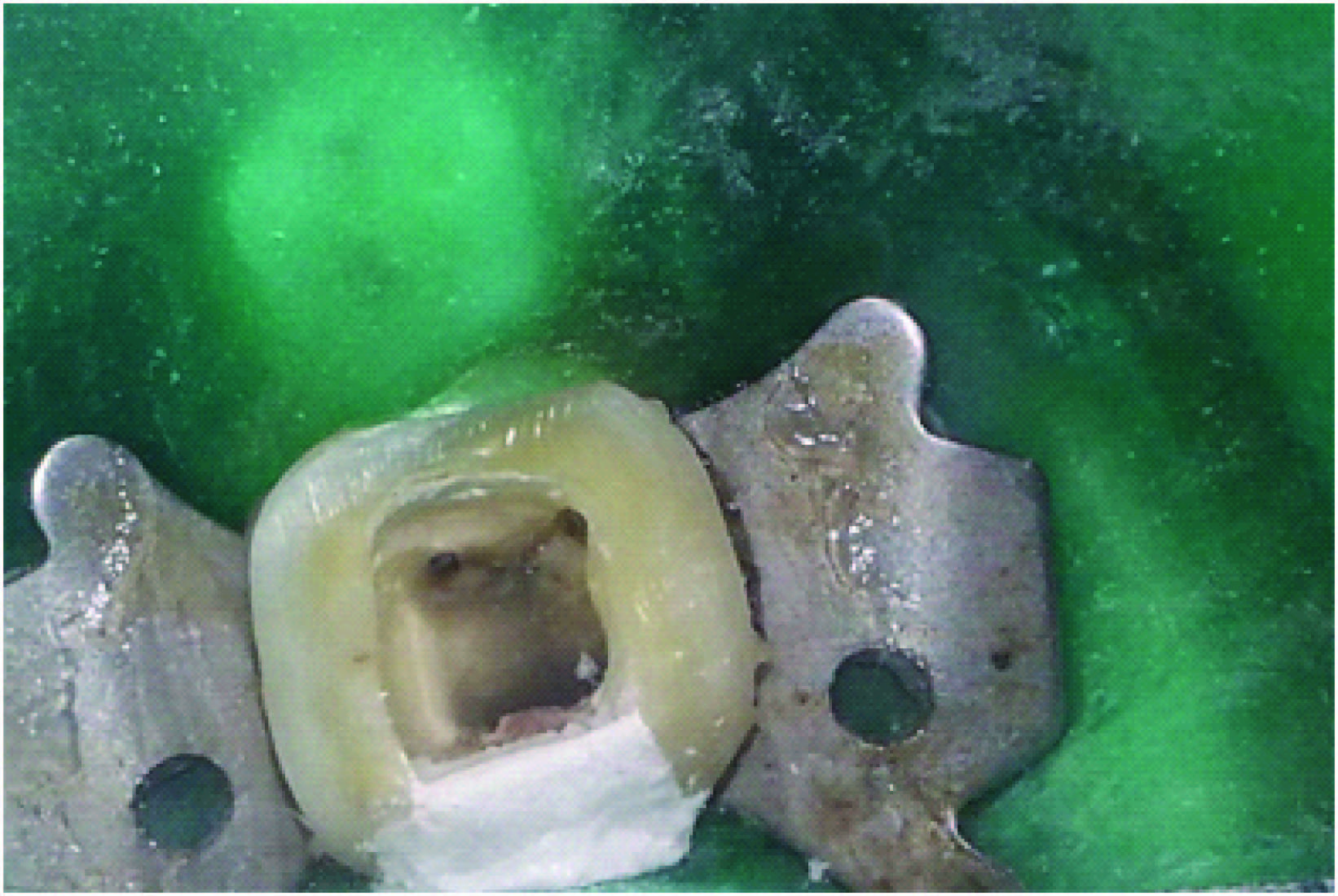
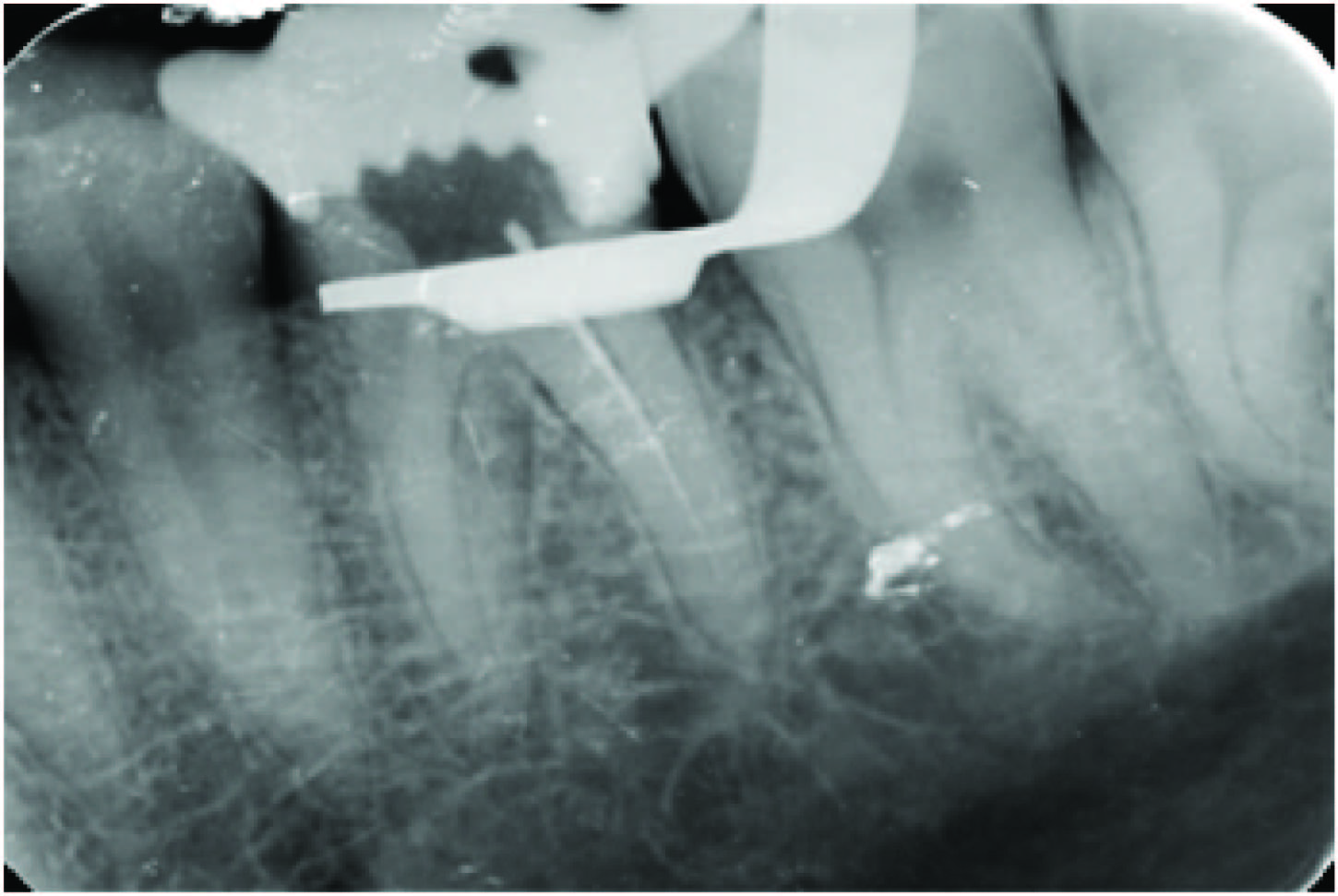
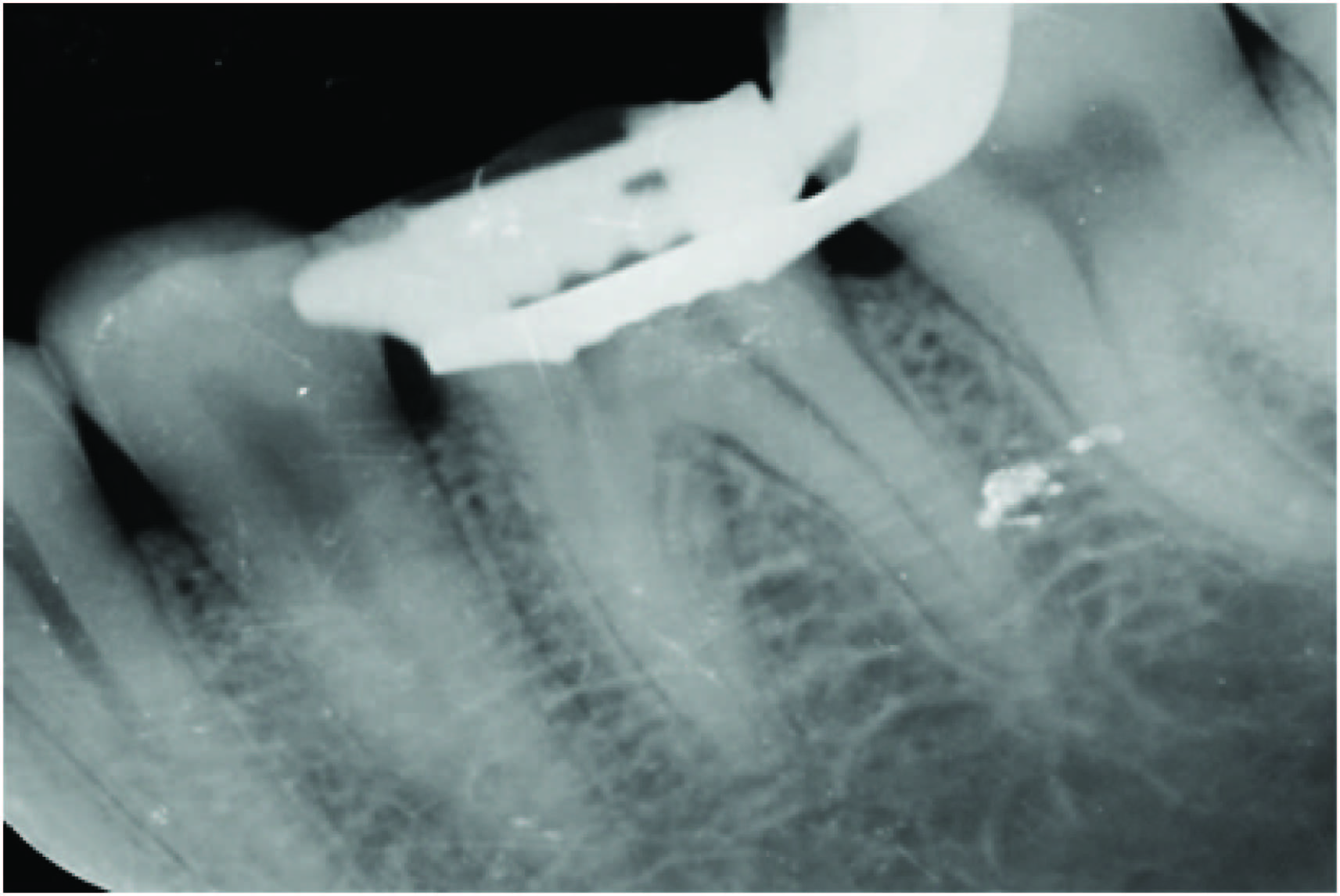
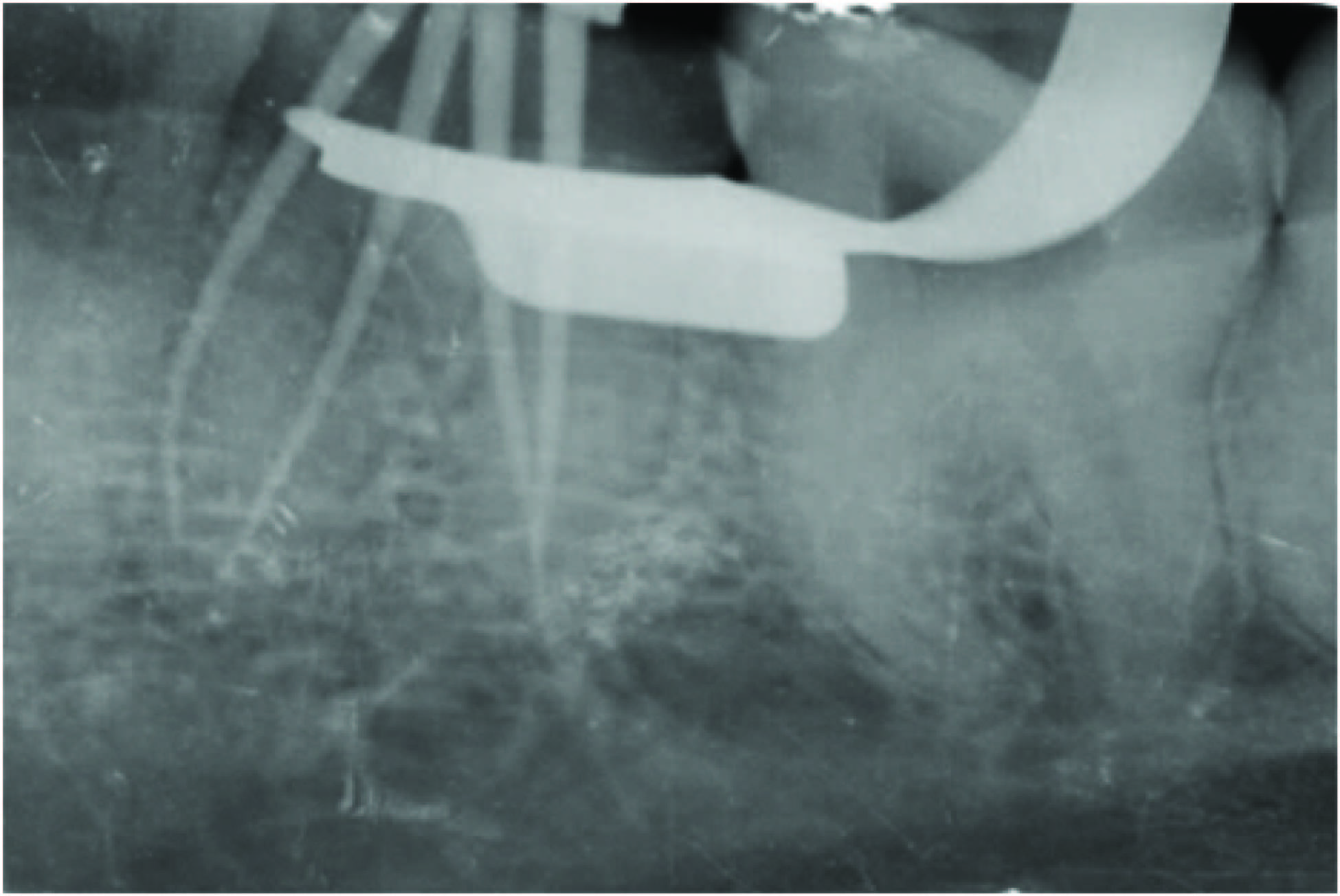
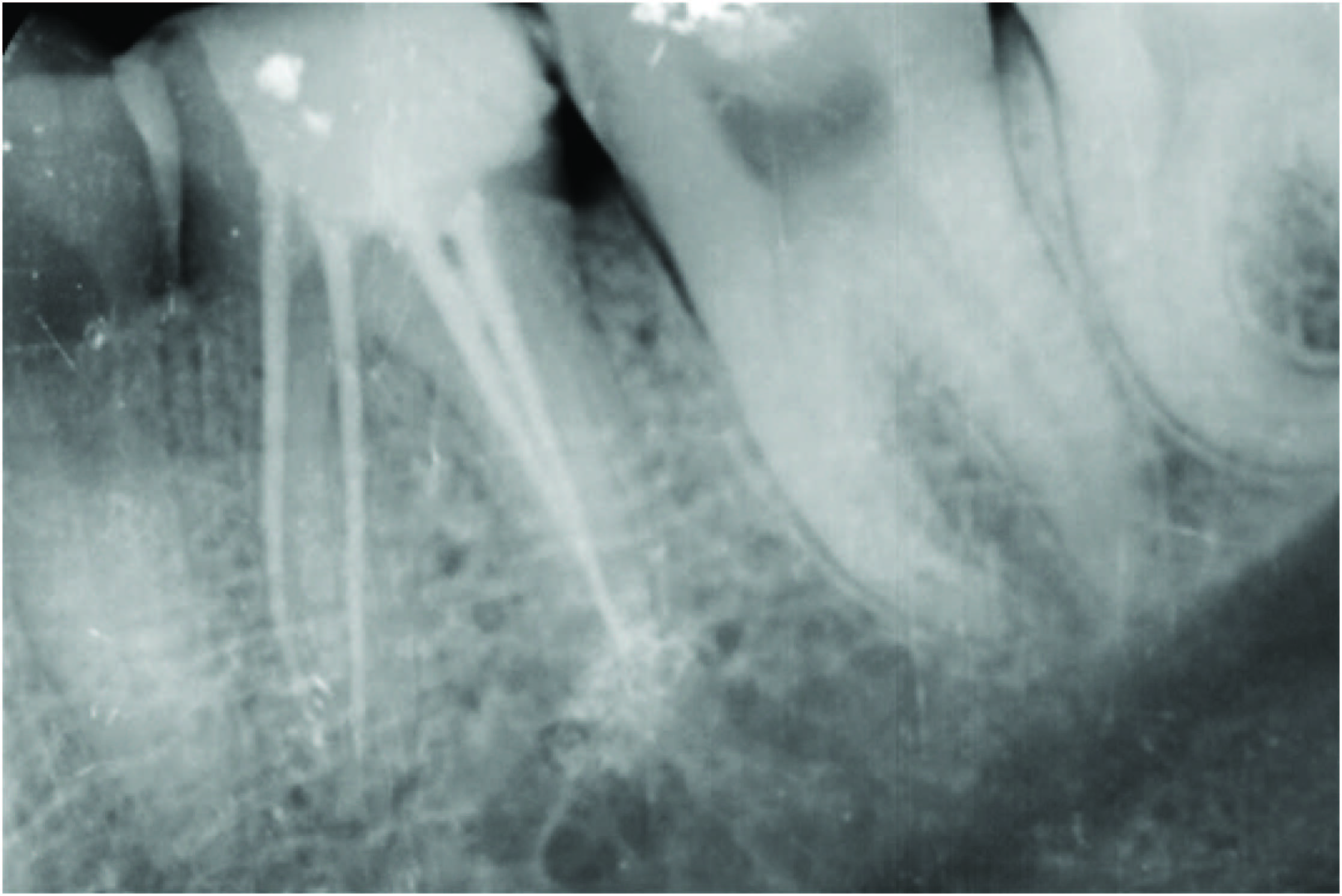
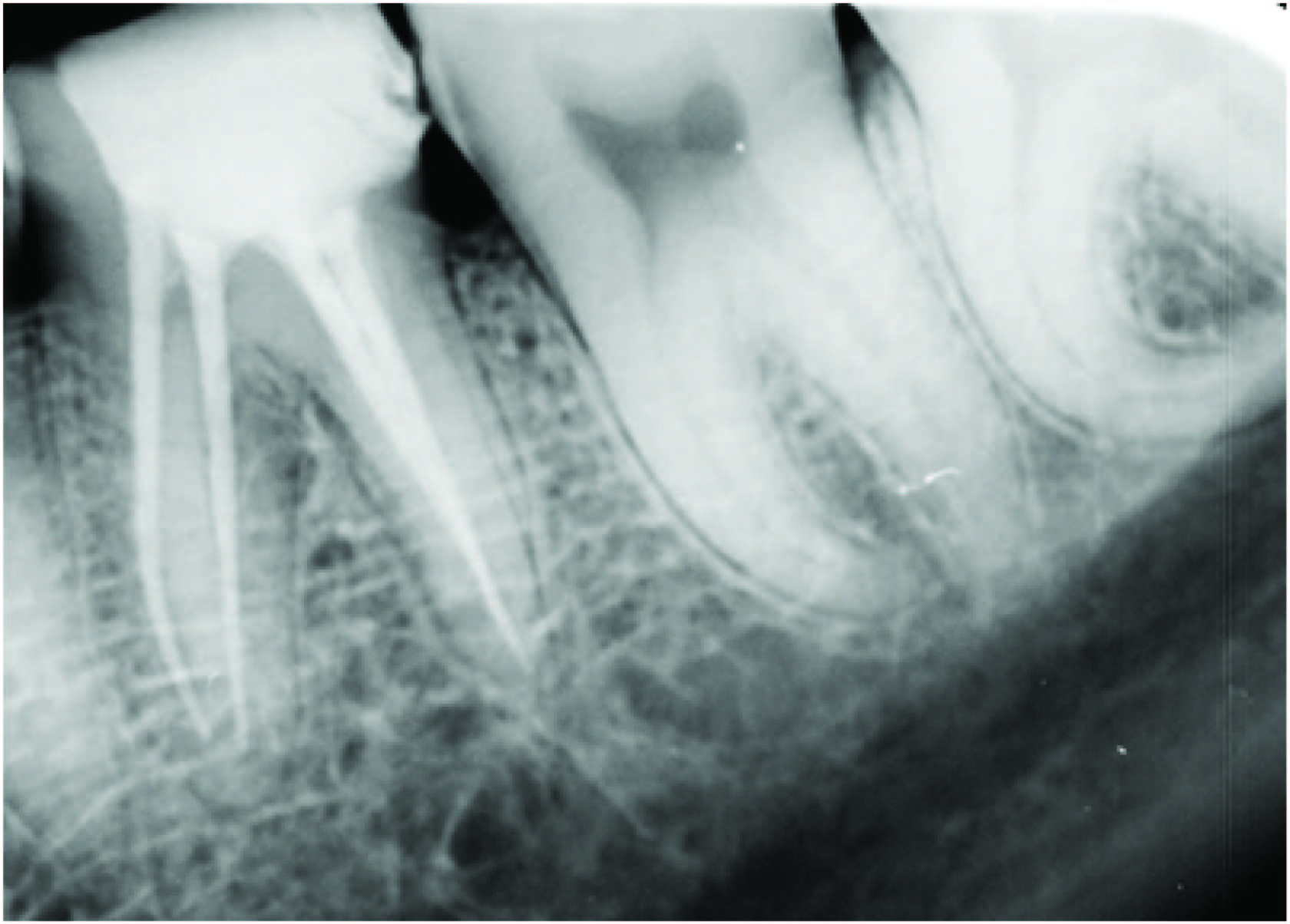
A 32-year-old male reported to department with chief complaint of pain in left lower back tooth region for last two days. Pain was sharp, severe and aggravated on taking hot and cold food stuffs. Patient was having disturbed sleep also. Clinical examination revealed carious lesion on distal aspect of mandibular left first molar. The tooth was sensitive to percussion also. A detailed radiographic examination revealed carious lesion on distal half approximating pulp and slightly widened periodontal ligament space around both roots [Table/Fig-1]. The tooth elicited positive response on electric and thermal pulp testing. Based on subjective and objective findings, a diagnosis of acute irreversible pulpitis was made and decision to do root canal treatment was taken. Root canal treatment was initiated under rubber dam isolation. Four canals were located and negotiated with size 8, 10 and 15 stainless steel K-file to their apices. Working length was determined using apex locator (Root ZX {J.morita,Tokyo,Japan}) with 15 K- file in all four canals. Cleaning and shaping was initiated with Rotary NiTi HERO Shapers under copious irrigation with 5.25% sodium hypochlorite and normal saline. During preparation of the distobuccal canal, approximately 10 mm of the size of 20, 0.04 taper HERO Shaper instrument fractured which was extending from the cervical third to the middle third of the root canal [Table/Fig-2]. A radiograph was taken to confirm the instrument separation [Table/Fig-3]. Following this event the patient was informed about the fractured instrument and the preparation of the rest of the canals were continued. Mesiolingual, mesiobuccal, distolingual canals were prepared with a size of 25, 0.04 taper HERO Shaper (MicroMega, Besancon, France). Prior to the filling of the canals, an attempt was made to retrieve the broken instrument from distobuccal canal with the help of the ultrasonic tip ET25 (satellac aceton, France). A radiograph was taken to confirm the instrument retrieval [Table/Fig-4]. On that attempt the instrument was removed successfully from the distobuccal canal [Table/Fig-5] and then was prepared till a size of 25, 0.04 taper HERO Shaper [Table/Fig-6]. All the four canals were then dried with paper points and obturated with gutta percha of a size 25 , 0.04 taper HERO Shaper and AH plus sealer (Dentsply Maillefer, Ballaigues, Switzerland) and a post obturation restoration was done with composite (SOLARE X GC corporation, Tokyo, Japan) [Table/Fig-7] . Follow up radiograph; after six months of treatment [Table/Fig-8] .
Discussion
Fracture of an instrument often results from improper use or overuse of an endodontic instrument [1]. Fractured instrument in the root canal is a concern to the patient and the dentist. Most of the stainless steel instruments fail by excessive torque and NiTi rotary files usually fracture because of torsional stress and cyclic loading. Aggressive movements, such as penetrating the canal too rapidly or forcing an instrument to an arbitrary length or among a sharp curve, can also lead to fracture [2]. With the advent of rotary NiTi files, there has been an unfortunate increase in the occurrence of broken instrument. Today, separated instruments can usually be removed due to technological advancements, ultrasonic instrumentation, and microtube delivery methods [3]. The factors influencing broken instrument removal should be identified and fully appreciated. The ability to nonsurgically access and remove a broken instrument will be influenced by the diameter, length and position of the obstruction within a canal. The potential to safely remove a broken instrument is further guided by anatomy, including the diameter, length, and curvature of the canal, and additionally limited by root morphology, including the thickness of dentin and the depth of external concavities [3]. In general, if one-third of the overall length of an obstruction can be exposed, it can usually be removed. Instruments that lie in the straightaway portions of the canal can typically be removed [3]. Separated instruments that lie partially around canal curvatures, although more difficult, can oftentimes be removed if straightline access can be established to their most coronal extents. If the broken instrument segment is apical to the curvature of the canal and safe access cannot be accomplished, then removal is usually not possible and, in the presence of signs or symptoms, surgery or an extraction will at times be required [3]. The type of material comprising an obstruction is another important factor to be considered. As an example, stainless steel files tend to be easier to remove as they do not further fracture during the removal process. Nickeltitanium broken instruments may break again, albeit deeper within the canal, during ultrasonic efforts due to heat buildup [3]. Whether a separated file’s cutting action was clockwise versus counterclockwise is important to visualize and know as this factor will influence the correct ultrasonic removal technique. Another factor that is central to successful instrument removal is integrating the best presently developed and proven technologies [3]. Traditionally, retrieving broken instruments posed formidable challenges. One time-honored technique has been the use of small files in efforts to either remove, or at least bypass, the broken instrument [3].
Over time, retrieval techniques evolved but were oftentimes ineffective because of limited vision and/or restricted space. Frequently, efforts directed toward instrument retrieval, even when successful, weakened a root due to overzealous canal enlargement, which in turn predisposed to a hopeless fracture and the loss of a tooth [3]. Indeed, the prognosis of a tooth can be seriously compromised if the efforts to remove a broken instrument lead to iatrogenic events, such as a ledged canal or root perforation. When retrieval efforts are unsuccessful, cleaning, shaping and obturation procedures are compromised and the ultimate prognosis is in doubt. Today, most broken instruments can be safely and efficiently removed with the use of advanced technologies and proper training [3]. The concept of using US in endodontics was first introduced by Richman in 1957. However, it was not until Martin et al. described the ability of ultrasonically activated K-type files to cut dentin that this application found common use in the preparation of root canals before filling and obturation. The term endosonics was coined by Martin and Cunningham and was defined as the ultrasonic and synergistic system of root canal instrumentation and disinfection [4,5].
Procedural errors in endodontics can occur at some point in the process of root canal treatment that can be a result of factors which the operator can have control or may not have any control. Factors affecting failures are instrumentation technique, use of torque controlled motor, dimension and surface condition of the instrument, rotation rate, radius of canal curvature, presence of straight line access and glide path to apical portion of the canal [6]. The success rate of removing fractured stainless steel instruments varies from 55% to 70%, whereas the success rate of removing fragments from distal canals of mandibular molars is 67%. Removal of broken NiTi fragments from the root canal is more challenging than that of stainless steel fractured instruments. Ultrasound is sound energy with a frequency above the range of human hearing, which is 20 kHz. The range of frequencies employed in the original ultrasonic units was between 25 and 40 kHz. Subsequently the so-called low-frequency ultrasonic handpieces operating from 1 to 8 kHz were developed, which produce lower shear stresses, thus causing less alteration to the tooth surface. There are two basic methods of producing ultrasound. The first is magnetostriction, which converts electromagnetic energy into mechanical energy. A stack of magnetostrictive metal strips in a handpiece is subjected to a standing and alternating magnetic field, as a result of which vibrations are produced. The second method is based on the piezoelectric principle, in which a crystal is used that changes dimension when an electrical charge is applied. Deformation of this crystal is converted into mechanical oscillation without producing heat. Piezoelectric units have some advantages compared with earlier magnetostrictive units because they offer more cycles per second, 40 versus 24 kHz [5]. The tips of these units work in a linear, back-and-forth, “piston-like” motion, which is ideal for endodontics. In this case fractured instrument is retrieved with the Aceton satelec P5 neutron which is the latest piezoelectric ultrasonic generator. Lea et al., demonstrated that the position of nodes and antinodes of an unconstrained and unloaded endosonic file activated by a 30-kHz piezon generator was along the file length [7]. As a result the file vibration displacement amplitude does not increase linearly with increasing generator power. This applies in particular when “troughing” for hidden canals or when removing posts and separated instruments. In addition, this motion is ideal in surgical endodontics when creating a preparation for a retrograde filling. A magnetostrictive unit, on the other hand, creates more of a figure eight (elliptical) motion, which is not ideal for either surgical or nonsurgical endodontic use. The magnetostrictive units also have the disadvantage that the stack generates heat, thus requiring adequate cooling [5,8]. Partially fatigued instruments, when flexed, reveal fractures associated with surface flaws , and prolonged clinical use of rotary NiTi instruments significantly reduces their cyclic flexural fatigue resistance [9]. When retrieval is impossible, some authors recommend that the fragment be fully bypassed for a more thorough cleansing of the canal and then sealed into the obturation [10]. Consequently, the clinicians had to adapt to the new characteristics of the new instruments. Operator-related factors have a significant influence on fracture incidence of rotary NiTi instruments [11]. Some of the studies further suggested that in most cases the retained fractured instrument can be incorporated into the final root canal filling, although recently developed techniques have made removal more predictable [12-14]. In our case of fractured instrument, the instrument is retrieved successfully with the help of the ultrasonic tips with minimal loss of root canal dentin.
Preoperative intraoral periapical radiograph showing caries approximating pulp in mandibular left first molar

Clinical image showing separated instrument in distobuccal canal
Intraoral periapical radiograph showing separated instrument
Intraoral periapical radiograph showing retrieval of separated instrument
Clinical image of the retrieved broken instrument

Intraoral periapical radiograph showing master cone in all four canals
Intraoral periapical radiograph showing obturation in all four canals
Follow- up intraoral periapical radiograph after six months of treatment
Conclusion
Clinician should be aware of techniques and various instruments. With the proper knowledge about root canal anatomy, root canal treatment, various accidents like instrument fracture can be reduced. This report has described “Ultrasonics” a conservative and safe technique for removal of fractured instruments.
[1]. M Rahimi, P Parashos, A novel technique for the removal of fractured instruments in the apical third of curved root canalsInt Endod J 2009 42(3):264-70. [Google Scholar]
[2]. P Parashos, HH Messer, Rotary NiTi instrument fracture and its consequencesJ Endod 2006 32(11):1031-43. [Google Scholar]
[3]. CJ Ruddle, Broken instrument removal. The endodontic challengeDent Today 2002 21(7):70-72. [Google Scholar]
[4]. H Martin, W Cunningham, Endosonic endodontics: the ultrasonic synergistic systemInt Dent J 1984 34(3):198-203. [Google Scholar]
[5]. G Plotino, CH Pameijer, NM Grande, F Somma, Ultrasonics in endodontics: a review of the literatureJ Endod 2007 33(2):81-95. [Google Scholar]
[6]. GSP Cheung, Instrument fracture: mechanisms, removal of fragments, and clinical outcomesEndod topics 2009 16:1-26. [Google Scholar]
[7]. SC Lea, AD Walmsley, PJ Lumley, G Landini, A new insight into the oscillation characteristics of endosonic files used in dentistry Phys Med Biol 2004 49(10):2095-102. [Google Scholar]
[8]. JR Ward, P Parashos, HH Messer, Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: clinical casesJ Endod 2003 29(11):764-67. [Google Scholar]
[9]. MG Bahia, VT Buono, Decrease in the fatigue resistance of nickel-titanium rotary instruments after clinical use in curved root canalsOral Surg Oral Med Oral Pathol Oral Radiol Endod 2005 100(2):249-55. [Google Scholar]
[10]. G Nevares, RS Cunha, ML Zuolo, Success rate for removing or bypassing fractured instrument:A prospective clinical studyJ Endod 2012 38(4):442-44. [Google Scholar]
[11]. P Parashos, I Gordon, HH Messer, Factors influencing defects of rotary nickeltitanium endodontic instruments after clinical useJ Endod 2004 30(10):722-25. [Google Scholar]
[12]. JR Ward, P Parashos, HH Messer, Evaluation of an ultrasonic technique to remove fractured rotary nickel-titanium endodontic instruments from root canals: an experimental studyJ Endod 2003 29(11):756-63. [Google Scholar]
[13]. CJ Ruddle, Nonsurgical retreatmentJ Endod 2004 30(12):827-45. [Google Scholar]
[14]. P Spili, P Parashos, HH Messer, The impact of instrument fracture on outcome of endodontics treatmentJ Endod 2005 31(12):845-50. [Google Scholar]