Appendicitis in a Child due to Streptococcus Pneumoniae: A Rare Case Report
Dnyaneshawari Purushottam Ghadage1, Deepali Shivajirao Kamble2, Swati Shivajirao Nale3, Arvind Vamanrao Bhore4
1 Professor and Head, Department of Microbiolgy, Smt.Kashibai Navale Medical College & General HospitalNarhe, Pune, India.
2 Tutor, Department of Microbiolgy, Smt.Kashibai Navale Medical College & General Hospital Narhe, Pune, India.
3 Assistant Professor, Department of Microbiolgy, Smt.Kashibai Navale Medical College & General HospitalNarhe, Pune, India.
4 Dean, Department of Microbiology, Smt.Kashibai Navale Medical College & General HospitalNarhe, Pune, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepali Shivajirao Kamble, Smt.Kashibai Navale Medical College, Department of Microbiology Narhe, Pune-411041, India. E-mail : Deepali19kamble@yahoo.com
A variety of bacterial species play a major role in appendicitis. Both aerobic and anaerobic gram positive and gram negative bacteria such as, Bacteroides fragilis, Streptococcus species, Escherichia coli, Klebsiella species and Citrobacter freundii cause appendicitis. Appendicitis is usually polymicrobial. The case assumes importance because of single aetiological agent i.e. unimicrobial and no predisposing factors are present to cause infection. We report a rare case of appendicitis due to Streptococcus pneumoniae in child. This case emphasizes that Streptococcus pneumoniae can cause wide spectrum of disease like appendicitis.
Appendicitis, Streptococcus pneumoniae, Unimicrobial
Case Report
In 2013 at Kashibai Navale Medical College and General hospital seven-year-old female child presented with a history of pain in abdomen in right iliac fossa and fever for two days. On general physical examination the patient was found to have pulse rate 108/min and blood pressure 100/60mmHg. Abdominal examination showed tenderness to all over abdomen. The respiratory system was normal. There was no other finding which suggested bacterial peritonitis. Biochemical results showed a serum urea 45mg/dl, Blood glucose 85mg/dl, serum creatine 89mg/dl, serum sodium 125meq/L and serum potassium 3.8meq/L.
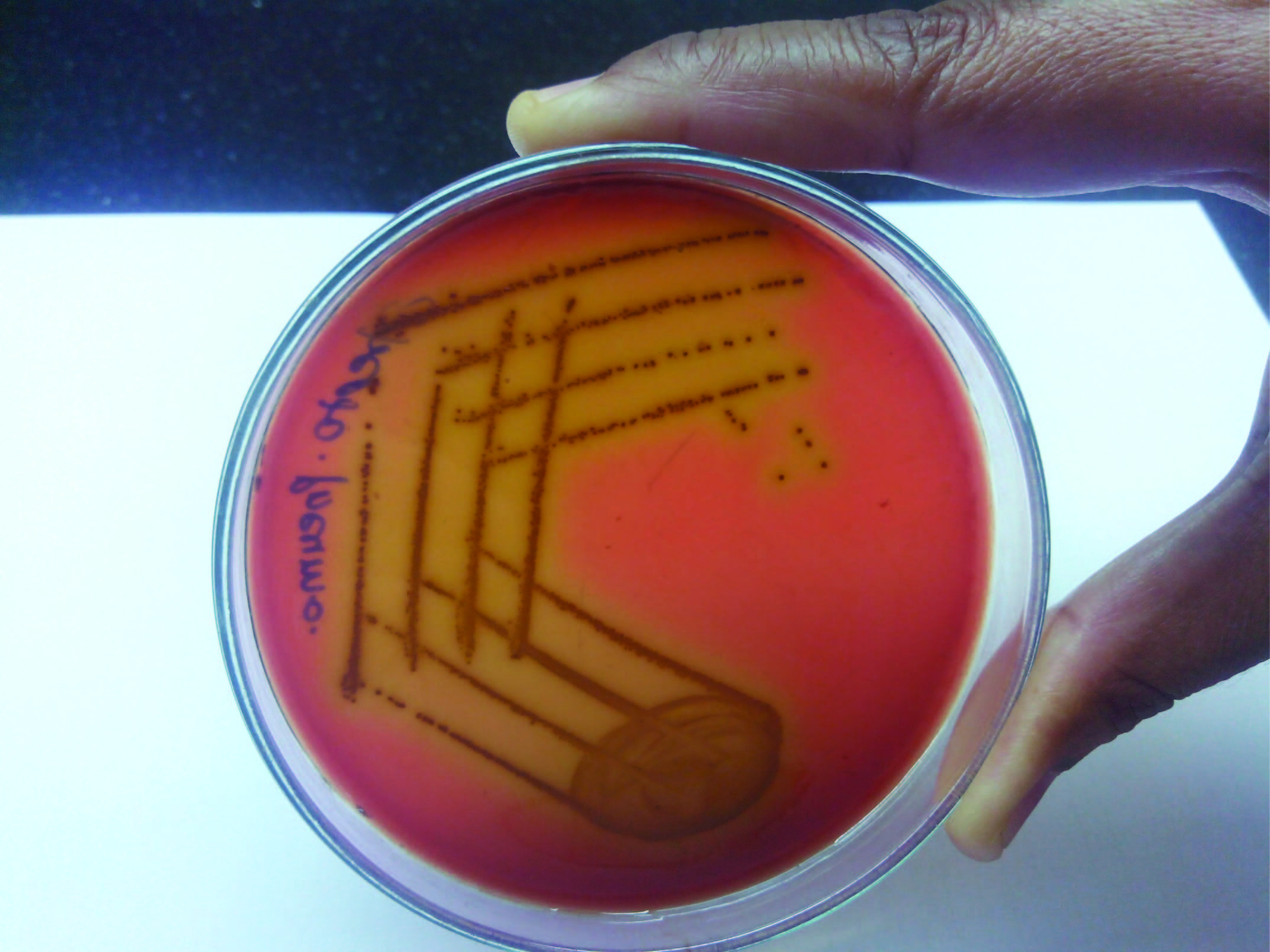
Ultrasonography of the abdomen was suggestive of appendicitis. The abdomen was opened by transverse right lower quadrant muscle incision. Enlarged and inflamed appendix was found preoperatively. Periappendicular pus was present. Pus was collected and appendicetomy was done. Pus was sent to microbiology laboratory for culture and sensitivity. Direct Gram stained smear showed Gram positive diplococci. Pus was inoculated aerobically on Blood agar and MacConkey’s agar and anaerobically in RCM. After incubation blood agar showed alpha haemolytic draughtman’s appearance colonies [Table/Fig-1]. There was no growth on MacConkey’s agar. No anaerobes were isolated. The organism was identified as Streptococcus pneumoniae by standard procedure. Sensitivity was done and it was found to be sensitive to penicillin (10 units), cefotaxime (30mcg), erythromycin (15mcg), Co-trimoxazole (25mcg), gentamycin (10mcg) and doxycycline (30mcg). We suggested blood culture, which was negative.
Alpha haemolytic colonies on blood agar
After procedure, patient fully recovered on the treatment of Cefotaxime 1 gm IV 12 hourly and Metronidazole 300 mg IV eight hourly for five days.
Discussion
Pneumococcal appendicitis are found in approximately 0.3% of the appendectomy cases [1–3]. The common predisposing factor causing pneumococcal infection are alcoholism, HIV, splenectomy, connective tissue diseases, haemophilia A, steroid use, diabetes mellitus and intravenous drug use [4–5]. In the present case there was no risk factor for invasive pneumococcal infection. This correlates with finding of Heltberg et al., and Bhattacharya et al., who reported no predisposing factor for invasive pneumococcal infection [3,6].
Appendicitis is usually caused by more than one organism i.e. it is polymicrobial. Stone et al., reported polymicrobial isolates from case of perforated appendix [7]. Appendicitis due to single aetiological agent is rare. Bhattacharya et al., [6,8] reported unimicrobial isolate [5,8]. Similarly Ronchetto and Pistono, reported seven cases of unimicrobial infection from 43 intraoperative samples of appendicular pus. Streptococcus pneumoniae were isolated in only two cases but in association with Bacteroides fragilis and Escherichia coli [9].
Primary pneumococcal peritonitis is rare in children and is usually associated with an underlying medical condition such as nephrotic syndrome or with upper genital tract disease [1,9]. Peritonitis in the present case may be because of perforation of appendix.
Pneumococcus commonly and asymptomatically colonizes the upper respiratory tract of children; a breakdown of the normal mucosal barrier plays a major role in the development of bacteremia [10,11]. We suspect that bacteraemia may have been the most probable source of appendicitis in this case; though blood culture was negative. Blood culture negativity may be due to prior administration of antibiotics.
Conclusion
Unimicrobial appendicitis is uncommon. Appendicitis due to Streptococcus pneumonia is rare. Our case emphasizes that Streptococcus pneumoniae can cause wide spectrum of disease like appendicitis also. Pneumococcal infections are fatal if not treated immediately especially of extreme ages.
[1]. Dan M, Igor D, Miriam Z, Sergio S, Carlos Primary Streptococcus pneumoniae appendicitis in a child: Case report and ReviewPed Infect Dis Jour 2003 22(3):282-84. [Google Scholar]
[2]. Capdevila O, Pallares R, TubauI G, Pneumococcal peritonitis in adult patientsArch Intern Med 2001 161:1742-48. [Google Scholar]
[3]. Heltberg O, Korner B, Schouenborg P, Six cases of acute appendicitis caused by Streptococcus pneumoniaeEur J Clin Microbiolo 1984 :141-43. [Google Scholar]
[4]. Taylor SN, Sanders CV, Unusual manifestations of invasive pneumococcal infectionAm J Med 1999 107(14):12-24S. [Google Scholar]
[5]. Jennifer A, Mark A, Pneumococcal appendicitis in a man with HIV infectionN Engl J Med 1993 328:1282 [Google Scholar]
[6]. Bhattacharya S, Kanungo R, Natarajan MK, Mahalakshmi VN, Unimicrobial appendicitis due to non-vaccine serotype of Streptococcus pneumoniae: Implications for and Management and PreventionInd J Med Microbiolo 2001 19 2(30):59-61. [Google Scholar]
[7]. Stone JH, Bacterial flora of appendicitis in childrenJ Pediatr Surg 1976 :11-37. [Google Scholar]
[8]. Gerome P, Bourilhon N, Soullie B, Foucher B, Otto MP, Milou F, Acute appendicitis due to both Klebsiella pneumoniae and serotype 35B Streptococcus pneumoniae, an emergent serotypeAnn Biol Clin(Paris) 2011 69(4):485-88. [Google Scholar]
[9]. Ronchetto F, Pistono PG, More on Pneumococcal appendicitisN Engl J Med 1993 329:1428 [Google Scholar]
[10]. Sirotnak AP, Eppes SD, Klein JD, Tubovarian abscess and peritonitis caused by Streptococcus pneumonia serotype 1 in young girlsClin Inf Dis 1996 22:993-96. [Google Scholar]
[11]. Steele RW, Pediatric Pneumococcal Bacteremiaemedicine. medscape.com/article/967600/overview [Google Scholar]