Small Bowel Obstruction- A Surprise
Jeffrey Daniel Mathew1, Ganesh Babu CP2, Balachandar M3, Ramanathan M4
1Post Graduate, Department of General Surgery, Mahatma Gandhi medical college and Research Institute, Pondicherry, India.
2Professor, Department of General Surgery, Mahatma Gandhi medical college and Research Institute, Pondicherry, India.
3Assistant Professor, Department of General Surgery, Mahatma Gandhi medical college and Research Institute, Pondicherry, India.
4Professor, Department of General Surgery, Mahatma Gandhi medical college and Research Institute, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jeffrey Daniel Mathew, Plot no 20, 3rd Cross, East Extn, Near Patrick School, Thanthai Periyar Nagar, Pondicherry-605005, India.
E-mail: danieljeffrey33@yahoo.com
Trans - omental hernia is very rare, accounting to 1-4% of all internal hernias which is an unusual cause of small bowel obstruction. Here we present a case report of a small bowel obstruction in a female due to trans - omental hernia presenting with central abdominal pain, distension and bilious vomiting. She had no previous history of trauma, surgery. Plain X-ray abdomen erect showed multiple air fluid levels with dilated small bowel loops. Emergency laparotomy revealed a segment of congested small bowel loop (ileum) through a defect in greater omentum. On table the herniated bowel loop was reduced and the defect in greater omentum was closed primarily. There was no necessity for bowel resection as it regained normal colour after reduction. Postoperative period was uneventful with complete resolution of symptoms. This case is presented for its rarity and its importance in clinical differential diagnosis of acute abdomen due to small bowel obstruction.
Greater omentum, Internal hernia, Small bowel obstruction
Case Report
A 28-year-old unmarried female presented to the emergency department with complaints of bilious vomiting for three days which contained undigested food particles. She also complained of central abdominal distension with pain and constipation for two days. The patient denied previous surgeries in the past. On examination at the time of admission, patient was febrile with temperature of 101o F. Blood pressure was 110/70mm Hg, Pulse Rate, 88/min. Abdomen was soft, central abdominal distension was present, tenderness was present in the umbilical region, bowel sounds were sluggish. Digital rectal examination revealed normal findings. Plain X-ray abdomen erect revealed multiple air fluid levels with dilated small bowel loops.
Laboratory studies were: Leucocytes 7100/cu mm, platelet 2.04lakhs /cu mm, Hb -10.8gms%, RBS – 93gm/dl. , Blood Urea 19mg/dl, Serum Creatine 0.6mg/dl, Urine routine – normal. Bleeding time, Clotting time, Serum electrolytes, Chest X-ray and ECG were normal. USG abdomen revealed dilated bowel loops and free fluid in the pouch of Douglas.
Patient was taken for emergency exploratory laparotomy. A midline incision was made for adequate visualisation . Intraoperative findings were:
• Minimal free fluid was present in the abdominal cavity
• Dilated jejunal bowel loops were present
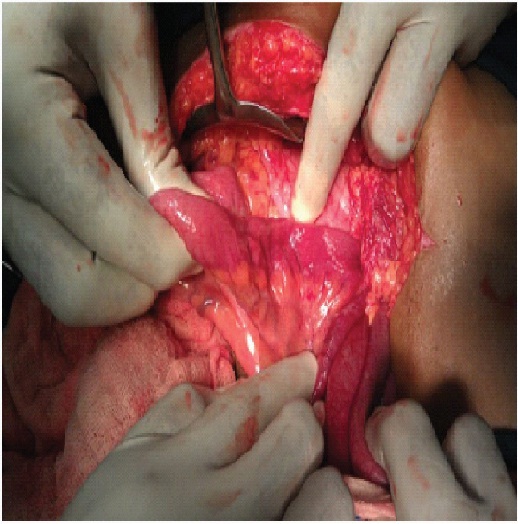
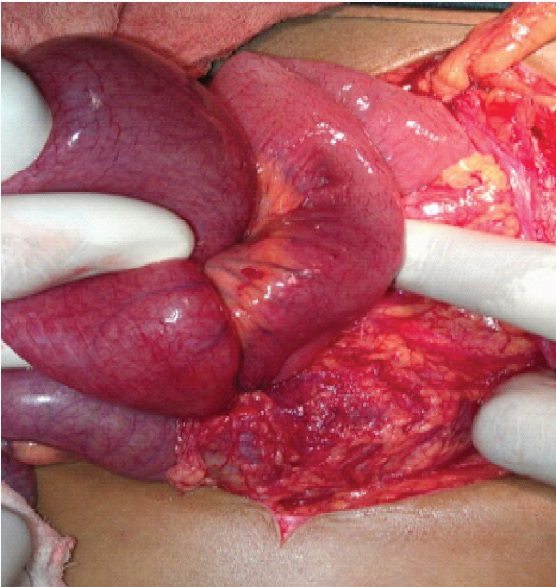
• A loop of ileum, 15cms from the ileocaecal junction was herniating • through the rent in the greater omentum. - [Table/Fig-1,2,3,4].
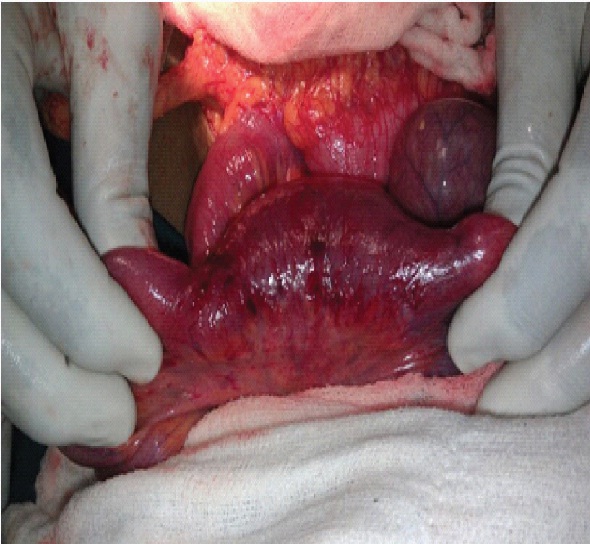
The herniated segment of the bowel loop was viable. Herniated bowel loop was freed from the rent in the greater omentum and Sectionreduced. The rent was then sutured primarily. The duodeno jejunal flexure was identified and the entire length of small bowel was milked to ileocaecal junction and the contents moved freely into large bowel. After a routine peritoneal lavage abdomen was closed in layers, after placing an ADK drain in the pelvis. The drain was removed on the 4th postoperative day. Skin sutures were removed on 10th postoperative day. Postoperative period was uneventful. When the patient was followed up after one month, she was free of any symptom and laparotomy wound was found healed well by primary intention without any complication.
Discussion
Internal hernia is defined as herniation of a viscus through a normal or abnormal aperture in the peritoneal cavity. Around 0.2-4% of intestinal obstruction is due to internal hernia [1,2]. Various causes of the omental defect have been suggested. These include a congenital or acquired origin [1,2], such as trauma, inflammation and atrophy due to old age. Around 50% of reported hernias in the literature are paraduodenal [3,4]. Patients with a trans-omental hernia usually have vague symptoms of bowel obstruction, which become worse as strangulation and gangrene ensue. Therefore, it takes a long time to diagnose ileus [4].
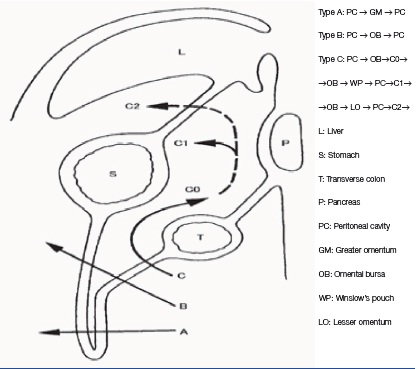
Yamaguchi [5] classified trans-omental hernias as Type A, Type B and Type C. In his study Type A was slightly more than Type C. Type B was not detected. Our case is Type A. Types of trans - omental hernia according to the classifications of Yamaguchi is shown in [Table/Fig-4]. Preoperatively internal hernia are difficult to diagnose by physical examination , therefore image is relied for diagnosis. Plain X-ray abdomen erect shows air- fluid levels. CT is the most important diagnostic tool [6,7]. Definitive diagnosis is mainly intraoperative. On exploratory laparotomy herniated bowel loop is reduced and the defect is closed. If there is bowel gangrene resection and anastamosis is required.
Bowel herniating into greater omentum
Bowel herniating into greater omentum
Bowel viable after reduction
Yamaguchi classification of trans omental hernia
Conclusion
Internal hernia should always be kept in mind in differential diagnosis of intestinal obstruction. Early intervention prevents unnecessary resection anastomosis. Imaging studies like ultrasonography and CT, are useful for early diagnosis.
[1]. M Onda, H Takasaki, K Furukawa, Nationwide Investigation of 21,899Cases of Intestinal ObstructionNihonFukubukyukyuIgaku 2000 20:629-36. [Google Scholar]
[2]. Li Jimmy CM, Chu David W, Small-bowel Intestinal Obstruction Caused by an Unusual InternalHerniaAsian Journal of Surg 2005 28:62-64. [Google Scholar]
[3]. CR Steinke, Internal hernia:Three additional case reportsArch Surg 1932 25:909-25. [Google Scholar]
[4]. JD Hull, Transomental herniaAm. Surg 1976 42:278-84. [Google Scholar]
[5]. T Yamaguchi, A case of incarceration of sigmoid colon into hiatus of greater omentumRinshoGeka 1978 33:1041-45. [Google Scholar]
[6]. K Uehara, H Hasegawa, S Ogiso, A case of transepiploic hernia successfully diagnosed preoperativelyNihonrinshogeka 1999 60:1930-33. [Google Scholar]
[7]. T Takada, H Yoshida, M Tsukada, A Case of Transomental Hernia in A 95- Year-old WomanJpnJGastroenterolSurg 2001 34:244-48. [Google Scholar]