The possible deleterious effects of “tongue thrust” swallowing received particular emphasis in the 1950’s and 1960’s. Laboratory studies show that individuals who place the tongue tip forward usually do not have more forces against the teeth than those who keep the tongue tip back. Tongue thrust swallowing in older patients superficially resembles the infantile swallow. Tongue thrusting in young children is usually a normal transitional stage in swallowing [1,2].
The modern viewpoint is that, the presence of an anterior open bite conditions the child or adult to place the tongue between the anterior teeth as a necessary physiologic adaptation. Therefore anterior tongue placement should be considered a result and not the cause of anterior open bite. It follows therefore that therapy to alter the way a child swallows is unwarranted [1,2].
As it has been proved that short term heavy forces such as those exerted during swallow and speech are not as relevant as long duration low forces [2]. In the present study, an attempt has been made to compare the tongue position of normal and open bite subjects at rest. An attempt has also been made to see whether there is any difference in the hyoid and posterior pharyngeal wall position in normal and open bite subjects and whether any correlation exists between soft tissue variables and underlying hard tissues.
Materials and Methods
The material analysed in this study consisted of 48 individuals out of which 24 had normal occlusion and 24 had open bite malocclusion. These individuals were further divided sex-wise. The age of the subjects ranged from 16 to 25 y. These subjects were selected after screening the patients visiting the out patients department of the government dental college and hospital, Nagpur. The age group of 16 to 25 y was taken to minimize the effect of growth on the data obtained.
Ethics Committee approval was taken from the institutional ethics committee and informed consent was taken from the subjects. The duration of the study was 18 months and subjects were randomly selected.
Criteria for selection of subjects
Normal subjects
All subjects had normal occlusion when observed clinically, with first permanent molars in class 1 relationship with a normal overjet and overbite.
Full complement of teeth upto the second permanent molars were present.
No previous orthodontic treatment was taken by any of the subjects.
Open bite subjects:The subjects had a clinically seen openbite.
No attempt was made to categorize the open bite into skeletal and dentoalveolar groups.
All subjects had a class 1 molar relationship.
Full complement of teeth upto the second permanent molars were present.
No previous orthodontic treatment was taken by any of the subjects.
Methods
The subjects were seated in the cephalostat with the FH plane parallel to the floor and the head stabilized. They were asked to protrude their tongue as much as possible. The dorsum of the tongue was then coated with a palatable suspension of Barium Sulphate (MICROBAR) with a flat brush. The subjects were asked to swallow on command. 10 seconds after the swallow the cephalograms were taken, since after approximately 10 seconds of the initiation of swallow, the tongue goes into rest position.
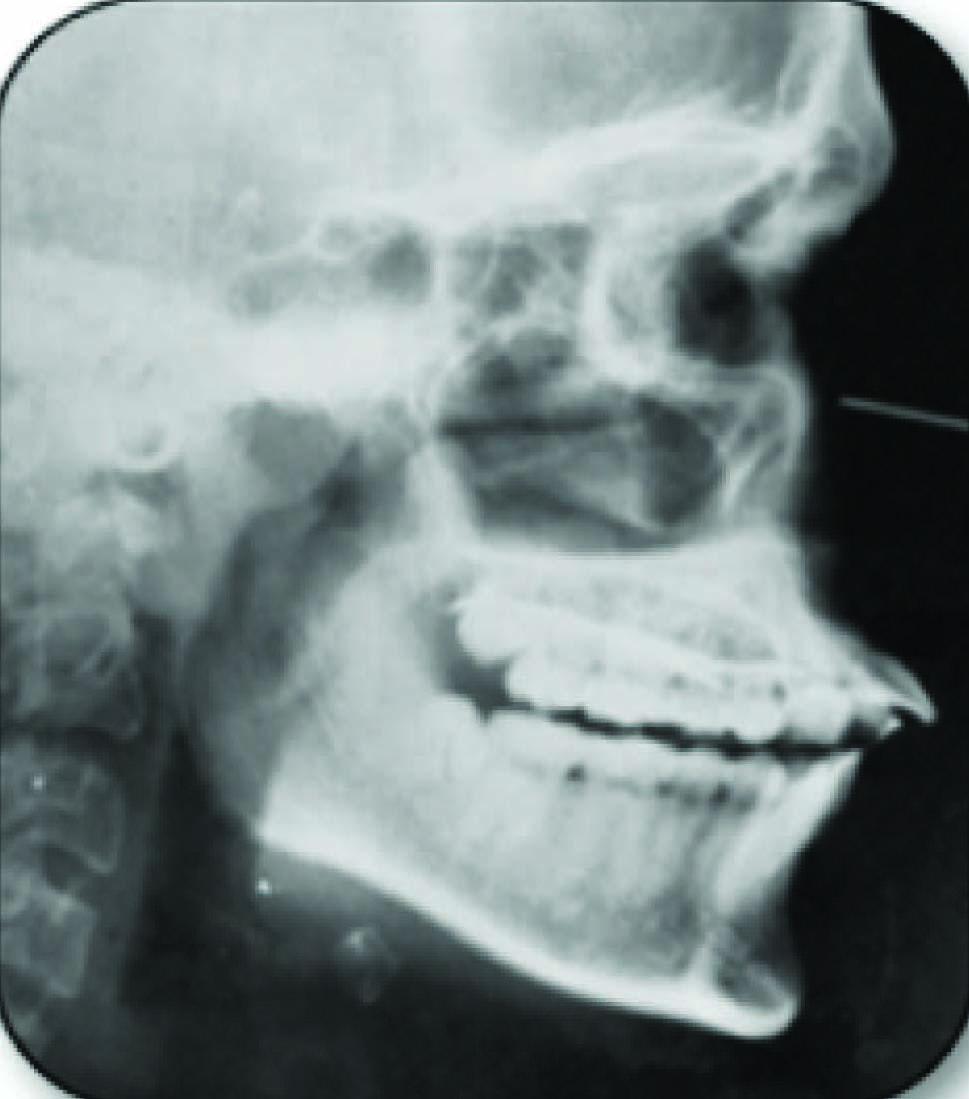
[Table/Fig-1,2]. Shows X-ray films in 8” x 10” dimensions in cassettes with intensifying screens were used in this study. The cephalograms were taken with a 5ft target film distance, voltage 85 Kvp, current 37 mA and exposure time of 1.3 sec. The structures were reproduced as accurately as possible. Wherever two borders were seen, the mean was taken.
Photograph of cephalogram of normal subject in rest position

Photograph of cephalogram of openbite subject in rest position
Rationale: Study was done with tongue in postural rest position in open bite subjects requiring orthodontic treatment and in normal subjects after obtaining the due consent from the subjects.
Barium Sulfate was coated on the tongue to facilitate the recording of actual radiographic image of tongue for position and volume.
Cons: No recorded allergic reactions to use of Barium Sulfate.
Study did not consider skeletal & Dental Open bite or type of swallowing pattern, [Table/Fig-3,4,5].
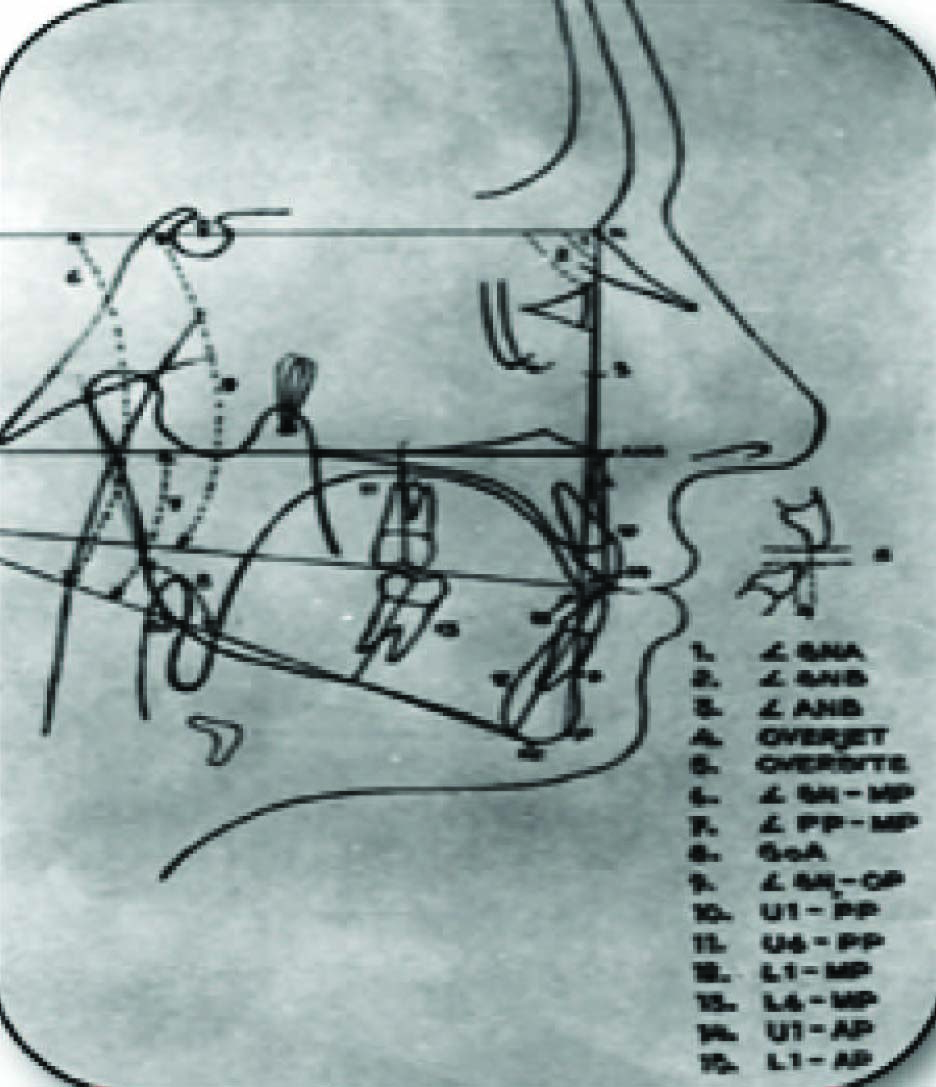
Photograph of cephalometric trading showing dentoskeletal measurements
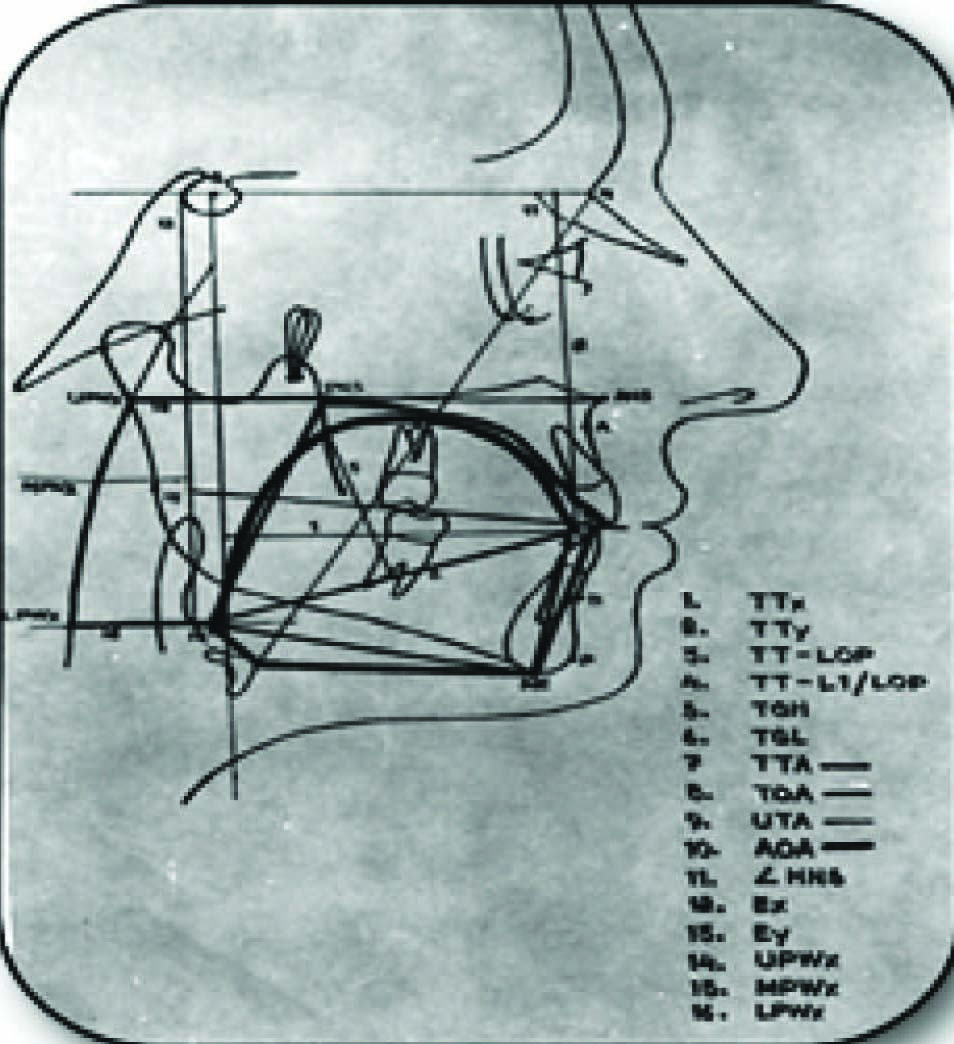
Photograph of Cephalometric trading showing tongue and soft tissue measurments
Dentoskeletal Landmarks / Lines and Planes / Linear Measurements ( in MM) / Angular Measurements (in Degrees)
| Dentoskeletal Landmarks | Lines & Planes | Linear Measure-ments (Mm) | Angular Measur-ements (Degrees) | Tongue, Hyoid & Phyrangeal Variables | Area Measur-ements (Mm2) |
|---|
| Sella (S) | S-N | OJ | SNA | TTx | TTA |
| Nasion (N) | Go-Me | OB | SNB | TTy | UTA |
| Gonion( Go) | Vertical reference line | U1-PP | ANB | Ex | TOA |
| Pogonion (Po) | ANS-PNS | U6-PP | SN-NP | Ey | UOA |
| Menton (Me) | Occulusal plane | L1-MP | PP-NP | UPWx | TTA/TOA (%) |
| Subspinale (A) | LOP | L6-MP | GoA | MPWx | UTA/AOA (%) |
| Supramentale (B) | NA Line | UI-AP | SN-OP | LPWx | |
| U6 | NB line | L1-AP | HNS | H | |
| U1 | NH line | PGL | | | |
| L6 | | TGH | | | |
| Ll | | TT-LOP | | | |
| Anterior nasal spine(ANS) | | TT-LI/LOP | | | |
| Posterior nasal spine (PNS) | | | | | |
Results
The difference between the over jet and overbite in the normal and open bite groups was found to be statistically highly significant. The open bite subjects had a larger over jet and as compared to the normal subjects [Table/Fig-5]. The mandibular plane angle (SN-MP) in both the groups showed a difference that was statistically highly significant, showing that the open bite subjects had steeper mandibular planes [Table/Fig-6].
Dentoskeletal Variables-Comparision of Means Between Normal and Openbite Subjects
| Variable | Normal Group | Open Bite Group | t-value |
|---|
| Mean±S.D. | Mean±S.D. |
|---|
| SNA (deg) | 81.25±4.22 | 81.52±4.52 | -0.209 |
| SNB (deg) | 79.75±3.86 | 80.08±3.88 | -0.482 |
| ANB (deg) | 1.58±1.28 | 1.44±2.12 | 0.271 |
| OJ (mm) | 2.85±1.06 | 5.46±2.43 | -4.72** |
| OB (mm) | 1.83±1.37 | -2.92±1.93 | 9.62** |
| SN/MP (deg) | 30.67±6.03 | 35.33±4.96 | -2.86** |
| PP/MP (deg) | 23.08±5.54 | 31.04±5.33 | -4.97** |
| GoA (deg) | 118.40±7.95 | 124.60±5.40 | -3.11** |
| SN/OP (deg) | 12.54±4.22 | 12.08±5.02 | 0.34i |
| Ul/PP (mm) | 29.13±3.42. | 30.79±3.56 | -1.61 |
| U6/PP (mm) | 24.08±2.36 | 26.13 ±2.45 | -2.89** |
| Ll/MP (mm) | 43.79±4.03 | 45±4.35 | -0.99 |
| L6/MP (mm) | 33.46±3.29 | 32.92 ±4.64 | 0.455 |
| Ll/AP (mm) | 4.92±2.18 | 9.42 ±3.35 | -5.4** |
| Ul/AP (mm) | 8.08±2.52 | 14.83 ±3.45 | -7.58** |
t < 2.01 Not significant
t > 2.01 Significant at 5% level (Significant *)
t > 2.69 Significant at 1% level (Highly significant **)
Comparison of the angle between Palatal plane and Mandibular plane between the two groups showed a difference that was highly significant, also the Gonial angles and Supraeruption of maxillary first molars in the open bite group as compared to the normal group were significantly larger in the open bite subjects [Table/Fig-6].
The tip of the upper and lower incisor and the AP line in both the groups was statistically significant indicating that the lower incisors were more proclined in the open bite groups [Table/Fig-6].
The difference in mean values of Ey in both the groups was statistically significant, meaning that the epiglottis occupied a higher position in the openbite subjects as compared to the normal subjects [Table/Fig-7].
Tongue soft tissue variables - comparision of mean between normal and openbite subjects
| Variable | Normal Group N = 24 | Openbite Groups N=24 | t-value |
|---|
| Mean±S.D. | Mean±S.D. |
|---|
| TTx (mm) | 66.33±5.23 | 68.13±7.82 | -0.918 : |
| TTy (mm) | -81.67±4.43 | -82.63±6.38 | 0.593 |
| TT/LOP (mm) | -0.333±1.818 | -1.46±2.35 | 1.819 |
| TT-L1/LOP (mm) | 3.15±3.00 | 1.79±4.09 | 1.286 |
| TGH (mm) | 39.75±4.19 | 38.92±3.35 | 0.742 |
| TGL (mm) | 80.71±5.37 | 82.83±6.62 | -1.193 |
| TTA/TOA (%) | 71±6 | 70.8±6.3 | 0.11 |
| UTA/AOA (%) | 66.2±11.1 | 63.2±9.3 | 0.994 |
| EX (mm) | -9.04±6.46 | -10.46±7.87 | 0.669 |
| EY (mm) | -116.63±10.45 | -108.75±12.10 | -2.403* |
| HNS (deg) | 57.92±3.96 | 57.71±4.16 | 0.175 |
| UPWX (mm) | -11.13±4.03 | -9.58±4.17 | -1.28 |
| MPWX (mm) | -17.67±4.65 | -16.83±5.34 | -0.569 |
| LPWX (mm) | -28.67±8.36 | -29.75±9.71 | 0.404 |
< 2.01 Not significant
t > 2.01 Significant at 5% level (Significant *)
t > 2.69 Significant at 1% level (Highly significant**)
The ratio of the total tongue are to total oral area (TTA/TOA – UTA/AOA) increases the ratio of upper tongue area to anterior oral are also increases, and as the tongue tip moves forward apparently the hyoid bone also moves forward [Table/Fig-8].
Showing correlation coefficients and t-values
| Variables | ‘r’ | ‘t’ |
|---|
| TTx - Ll/AP |
| Normal | 0.705 | 4.66** |
| Openbite | 0.1808 | 0.862 |
| TTA/TOA - UTA/AOA |
| Normal | 0.668 | 4.320** |
| Openbite | 0.502 | 2.724** |
| TTx - HNS |
| Normal | 0.579 | 3.339** |
| Openbite | 0.1519 | 0.721 |
t > 1.717 Not significant
t > 1.717 Significant at 5% level (Significant *)
t > 2.508 Significant at 1% level (Highly significant**)
Discussion
Comparison of mean values for the angle SNA and SNB for both the groups which showed similar values and the difference was statistically insignificant, suggesting that the antero-posterior relationship of maxilla and mandible to the cranial base is normal in both the groups [Table/Fig-7]. In a similar study conducted by Takada & Lowe [3], there was no significant difference in angle SNA and SNB in the normal as well as open bite groups. Similar findings were seen in the studies conducted by Takada & Lowe [3], Subtelny and Sakuda [4], Nahoum [5,6] and Issacson [7].
It is true that the MPA increases in long faced individuals nevertheless as stated by Fields and colleagues not all long faced patients have open bite and vice versa [8].
The study did not aim at evaluating aberrant tongue function and its effect on orofacial structures. The steepness of the mandibular plane is because of molar extrusion, or it may be because of short ramus height.
Comparison of the angle between palatal plane and mandibular plane between the two groups showed a difference that was highly significant. The findings are in agreement with those Takada & Lowe [3] and Nahoum [5,6]. This could be due to an upward cant of the palatal plane or due to a downward and backward rotation of the mandible.
Gonial angles were significantly larger in the open bite subjects as was also seen in the studies of Takada & Lowe [3], Subtelny and Sakuda [4] and Nahoum and Harrowitz [6]. This increase may be due to vertical growth pattern in the openbite subjects. The difference in the occlusal plane angle (SN-OP) in both the groups showed no statistical significance [Table/Fig-6]. Similar results were obtained by Takada & Lowe [3].
In an attempt to compare the upper incisor eruption with respect to the palatal plane, the distance between the upper incisor tip and the palatal plane was measured. The difference in the two groups was statistically insignificant as was also seen in the study by Takada & Lowe [3]. However, significantly greater eruption was seen in a similar study conducted by Parker [9] and Subtelny and Sakuda [4].
The linear distance between the occlusal midpoint of the maxillary first molar and the palatal plane was measured (U6-PP). The difference in the two groups was highly significant, indicating supraeruption of maxillary first molars in the open bite group as compared to the normal group [Table/Fig-6].
This finding is in agreement with the findings of Takada and Lowe [3], Subtelny and Sakuda [4], and Parker [9]. The increase in the molar eruption could account for the increase in the mandibular plane angle and also for the increase in the PP-MP angle.
The linear distance between the mandibular incisor tip and the mandibular plane was measured in both the groups and the difference was not significant. Similar findings were seen in the study by Takada and Lowe [3] indicating that there was no difference in the level of eruption of lower incisor in both the groups. Same findings were also seen in studies conducted by Subtelny and Sakuda [4], and Issacson [7].
The mandibular first molar also did not show any difference in eruption in both the groups as was also seen in a similar study by Subtelny and Sakuda [4], Nahoum and Harrowitz [6], Takada and Lowe [3].
The difference in the mean values of the distance between the tip of the lower incisor and the AP line in both the groups was statistically significant indicating that the lower incisors were more proclined in the open bite groups [Table/Fig-6].
The upper incisors were more proclined in the openbite group and the difference was highly significant. The findings are similar to those of Takada and Lowe [3]. In the present study, the increased proclination could be responsible for the decreased distance between the upper incisor tip and the palatal plane [Table/Fig-6].
The mean values of the tongue tip from the vertical reference line (TTx) in the openbite group was slightly larger than that of the normal subjects, indicating that the tip of the tongue was placed slightly forward in the openbite group [Table/Fig-7]. However, the difference was not statistically significant. In a similar study conducted by Takada and Lowe [3], the tongue tip was found to be significantly forward in the openbite group.
The vertical distance of the tongue tip from the SN plane (TTy) denotes the supero-inferior position of the tongue tip. A comparison of the mean values between the two groups showed that the tongue tip is slightly lower in the openbite group. However this difference was not statistically significant [Table/Fig-7]. Similar findings were observed by Takada and Lowe [3].
TT-LOP indicates the relationship of the tongue tip to the lower occlusal plane in a vertical direction. In the present study, the tongue tip was found to be above the lower occlusal plane in both the groups [Table/Fig-7]. In the openbite group, the tip was higher than in the normal group [Table/Fig-7]. The difference was, however, not of statistical significance. Takada and Lowe [3] found the tongue tip to lie significantly above the lower occlusal plane in the openbite group.
Mean values for TGH in both the groups showed no significant difference indicating that the height of the tongue is more or less the same in both the groups [Table/Fig-7].
The finding contradict those of Takada and Lowe [3], who found that the height of tongue was significantly larger in the open bite subject.
TGL or the tongue length is the distance between the tongue tip & Epiglotis. There was no significant difference in the mean values in the normal & open bite groups in the present study [Table/Fig-7]. Similar findings were seen in the study of Takada and Lowe [3].
TTA/TOA or the total tongue occupancy area is the ratio of the total tongue area to the total oral area. In the present study, there was no significant difference in both the groups [Table/Fig-7]. In the Takada and Lowe [3] study, the total tongue occupancy area was significantly larger in the open bite groups.
UTA / AOA or the partial tongue occupancy area is the ratio between the upper tongue area & the anterior oral area. On comparison of the means, no difference in the partial tongue occupancy area was seen between the groups [Table/Fig-7]. Similar findings were observed in the Takada and Lowe [3] study.
Ex is the horizontal distance of the deepest point of the Epiglottis from the vertical reference line. Comparison of the mean values in the two groups showed no significant difference meaning that the position of the Epiglottis is the same in both the groups [Table/Fig-7]. These findings are in agreement with these of Takada and Lowe [3].
Ey is the vertical distance of the deepest point of the Epiglottis from SN Plane. The difference in mean values in both the groups was statistically significant, meaning that the epiglottis occupied a higher position in the openbite subjects as compared to the normal subjects [Table/Fig-7]. The findings contradict those of Takada and Lowe [3] who did not find any difference in the two groups.
HNS or the hyoid angle is the angle formed between the SN plane and the NH line. No statistically significant difference was seen in the hyoid angle between the normal and openbite groups [Table/Fig-7]. Subtelny and Sakuda [4] also found no significant difference in the antero-posterior position or the vertical position of the hyoid bone in the two groups. Cleall [10] found the hyoid bone to be placed posteriorly in his tongue thrust group.
Takada and Lowe [3] in their study of normal and skeletal class 1 openbite subjects found the hyoid bone to be significantly forward in the openbite group. They had excluded the presence of digit sucking and tongue thrusting from their study group, whereas in the present study, the presence or absence of habits was not considered.
The upper pharyngeal wall (UPWx), the middle pharyngeal wall (MPWx) did not show any statistically significant difference in the present study [Table/Fig-7]. This was in contrast to the findings of Takada and Lowe AA [11] in a similar study. However, the (LPWx), i.e. the lower pharyngeal wall did not show any difference [Table/Fig-7], in the present study as well as the study of Takada and Lowe [3].
In the normal subjects there was a positive correlation between horizontal position of the tongue tip and the position of the lower incisors meaning that as the tongue tip was placed more anteriorly with reference to the vertical reference line, the lower incisors proclinate [Table/Fig-8]. In the openbite group too, a positive correlation was seen which was statistically insignificant. Similarly, a positive correlation was seen between the total tongue occupancy area and the partial tongue occupancy area which was statistically significant.
Many studies have demonstrated that tongue thrust plays an important role in the aetiology of open bite as well as in the relapse of treated open bite patients [12] however, studies also show that tongue posture (Mild to moderate with continous pressure) also plays a important role in aetiology of open bite.
'Thrust' is still an inappropriate word since the tongue is not really 'thrusting' during rest. However, it must be remembered that 'thrusting' in this instance is still a mild but continuous lingual pressure factor. The significance lies in whether or not this 'thrust, either during swallowing and other functional behaviors, or during rest, is responsible for, contributes to, or is a consequence of the development of a malocclusion.
Conclusion
In the present study,a forward tongue position and lower incisor position and increased mandibular plane angle, gonial angle, palatal plane, mandibular plane angle was found in open bite subjects. Additionally it was seen that as the total tongue area increased, the total oral area also increased. Similarlly as the upper tongue area increased the anterior oral area also increased.
Identifying the underlying cause(s) of open bite is essential for accurate diagnosis and precise treatment planning which is difficult because of the interrelatedness of genetic, environmental, and functional factors. In case of habits leading to the open bite the intensity as well as duration of the habit and the timing of growth is an important consideration. Although functional factors (such as nasal restriction, abnormal functional patterns of the tongue, oral habits, abnormal swallowing patterns, and speech problems) often play a role in the aetiology of open bite, they are just as often disregarded because of the inability of cephalometric analysis to measure functional and compensatory mechanisms.
For diagnosis of open bite malocclusion cephalometrics should not be the sole criteria. This may lead to inaccurate diagnosis which in turn can lead to poor treatment planning and prognosis as well as increase relapses. Functional factors including mastication should be considered for treatment success and better stability of results.
t < 2.01 Not significant
t > 2.01 Significant at 5% level (Significant *)
t > 2.69 Significant at 1% level (Highly significant **)
< 2.01 Not significant
t > 2.01 Significant at 5% level (Significant *)
t > 2.69 Significant at 1% level (Highly significant**)
t > 1.717 Not significant
t > 1.717 Significant at 5% level (Significant *)
t > 2.508 Significant at 1% level (Highly significant**)