Non-communicable diseases (NCDs) such as diabetes and CVD have now become the main public health challenge for the 21st century, as a result of their impact on personal and national health system and the premature morbidity and mortality associated with the NCDs [1]. CVD is a global health problem and a leading cause of death in developed countries and increasing in developing countries [2].
Millions of patients with chest pain present annually to emergency departments, and many more present with other symptoms potentially indicative of ischemia. A low threshold for consideration of a myocardial aetiology of chest pain (or related symptoms) is necessary, because the presentation of an ACS is often atypical and a missed diagnosis of ACS carries considerable risk to patients. The diagnosis of patients of ACS is based on clinical, electrocardiogram and few biochemical markers like cardiac troponin T (TnT). Recently developed, High-sensitivity troponin hs-TnT assays detect small amounts of cardiomyocyte injury that could not be detected by earlier versions of the assays. This at first glance appears to be an additional value of the biomarker but has implications on how elevated hs-TnT has to be interpreted in the clinical practice. The rule-in of acute myocardial infarction (AMI) has become more challenging with the introduction of high sensitivity assays. Especially patients with non-ACS-related troponin elevations have an adverse outcome and require careful patient management [3].
According to certain studies serum hs-TnT parameter has to rise 100% of original value in next six hours of the original estimation if the levels are non-confirmatory [4,5]. There may be false high estimation of hsTnT due to other causes which further would not increase to significant levels in next six hours. This is crucial time for diagnosis of MI and for its treatment. Hence, we look forward to a parameter which would rise in early six hours of myocardial ischemia and help in rule in strategy of ACS.
A biomarker that reliably detects myocardial ischemia in the absence of necrosis would be useful for initial identification and for differentiating patients with chest pain of aetiology other than coronary ischemia, and could provide clinical utility complementary to that of cardiac troponins (cTn), the established markers of necrosis. H-FABP, have been suggested to have clinical utility as indicator of cardiac ischemia [6]. Fatty acid-binding proteins (FABP) are small (15 kDa) cytoplasm proteins that are abundantly expressed in tissues with an active fatty acid metabolism such as heart and liver [7,8]. H-FABP is found in abundance in cardiomyocytes. H-FABP is a low molecular weight cytoplasmic protein. Because of its small size and location, it is released rapidly into the blood following myocardial damage before the cell gets disrupted [9,10]. We hypothesized that h-FABP would have greater diagnostic value when hs-TnT results are not confirmatory. The aim of study was to test the diagnostic performance of hs-TnT and h-FABP.
Materials and Methods
The study was carried out at Pramukhswami Medical College and Shri Krishna Tertiary Care Teaching Hospital, Gujarat, India from September 2012 to September 2013. Diagnosis of MI was done on the basis of third universal definition of MI given by Joint ESC/ACCF/AHA/WHF Task Force for universal definition of MI [11].
The following criteria meet the diagnosis for MI: Detection of a rise and/or fall of cardiac biomarker values {preferably cardiac troponin (cTn)} with at least one value above the 99th percentile upper reference limit (URL) and with at least one of the following:
Symptoms of ischemia.
New or presumed new significant ST-segment–T wave (ST–T) changes or new left bundle branch block (LBBB).
Development of pathological Q waves in the Electrocardiography ECG).
Imaging evidence of new loss of viable myocardium or new regional wall motion abnormality.
Identification of an intracoronary thrombus by angiography or autopsy.
Exclusion Criteria
Patients with renal diseases, acute stroke and myopathy.
Patients with liver cirrhosis and cancer.
Patient taking alcohol, tobacco, oral contraceptives, hormone replacement or supplementation therapy.
Patients with Modified physiological states – pregnancy, psychological and mental disorders such as severe stress and depression.
This cross sectional study group consisted of 88 patients of age group >25, admitted in emergency department and in intensive cardiac care unit within six hours of clinical signs and symptoms of ACS. The patients had been diagnosed and classified as ischemic chest pain and non-ischemic chest pain depending upon the assessment as per the clinical signs, symptoms and diagnostic criteria mentioned earlier.
Group 1 included 34 patients out of 88 patients with acute chest pain and evidence of early myocardial ischemia and AMI depending upon the assessment as per the clinical symptoms such as chest pain with or without radiation, chest heaviness, shortness of breath, lower jaw pain, left arm pain, epigastric pain, palpitations and signs like hypotension and ECG changes suggestive of MI. These were labeled as “Ischemic chest pain”. These patients had hs-TnT <100 pg/mL but more than 14pg/mL within six hours of symptoms and subsequent hs-TnT level after 6-12 h of the first estimation rose by 100% of the original value.
Group 2 included 29 out of 88 patients with acute chest pain but no subsequent evidence of myocardial ischemia. Their subsequent hs-TnT level after 6-12 h of first estimation did not rise by 100% of the original value. Group 3 included 25 apparently healthy persons who came for routine health checkup were taken in control group.
Blood was collected from all the enrolled patients within one hour of admission, before any treatment was started, in red top vaccutainer tubes, containing no anticoagulant. Specimens were routinely centrifuged within 1 hr of collection for 15 min at 1500g, and serum was separated. hs-TnT was measured quantitatively using ECL (electrochemiluminescence) immune assay based on ECL technology (hs-TnT, Cobas e411, Roche, Mannheim, Germany) on cobas e411. While serum H-FABP levels were determined using a human H-FABP ELISA method [12] (Hycult Biotech, the Netherlands).
A study protocol was set before undertaking this study and it was approved by institutional Human Research Ethical Committee. Analysis was performed using the commercially available statistical software SPSS – 14.0 version, Medcalc version 12.5 and Microsoft excel.
Results
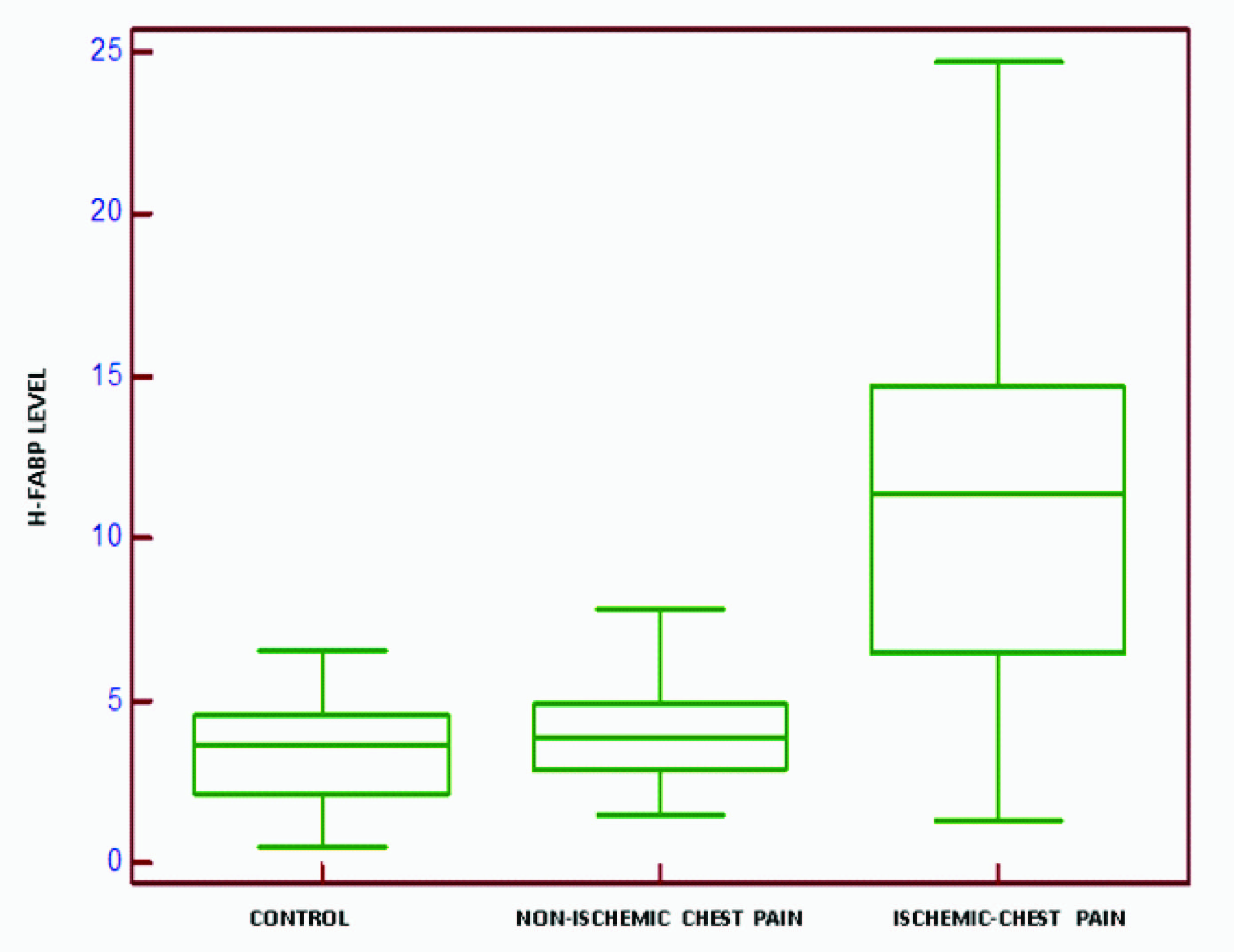
The mean H-FABP levels were 3.29 ± 1.57 ng/mL for control group, 4.31 ± 2.36 ng/mL for non-ischemic chest pain group and 10.68 ± 5.56 ng/mL for ischemic chest pain group. The unpaired t-test performed between non ischemic chest pain and control groups showed no significant difference (p=0.065) while between non ischemic chest pain and ischemic chest pain groups showed significant difference (p=<0.001) [Table/Fig-1].
Box and whisker plot showing comparison of H-FABP levels (ng/mL) between control group, non-ischemic chest pain and ischemic chest pain
ROC curve analysis for H-FABP
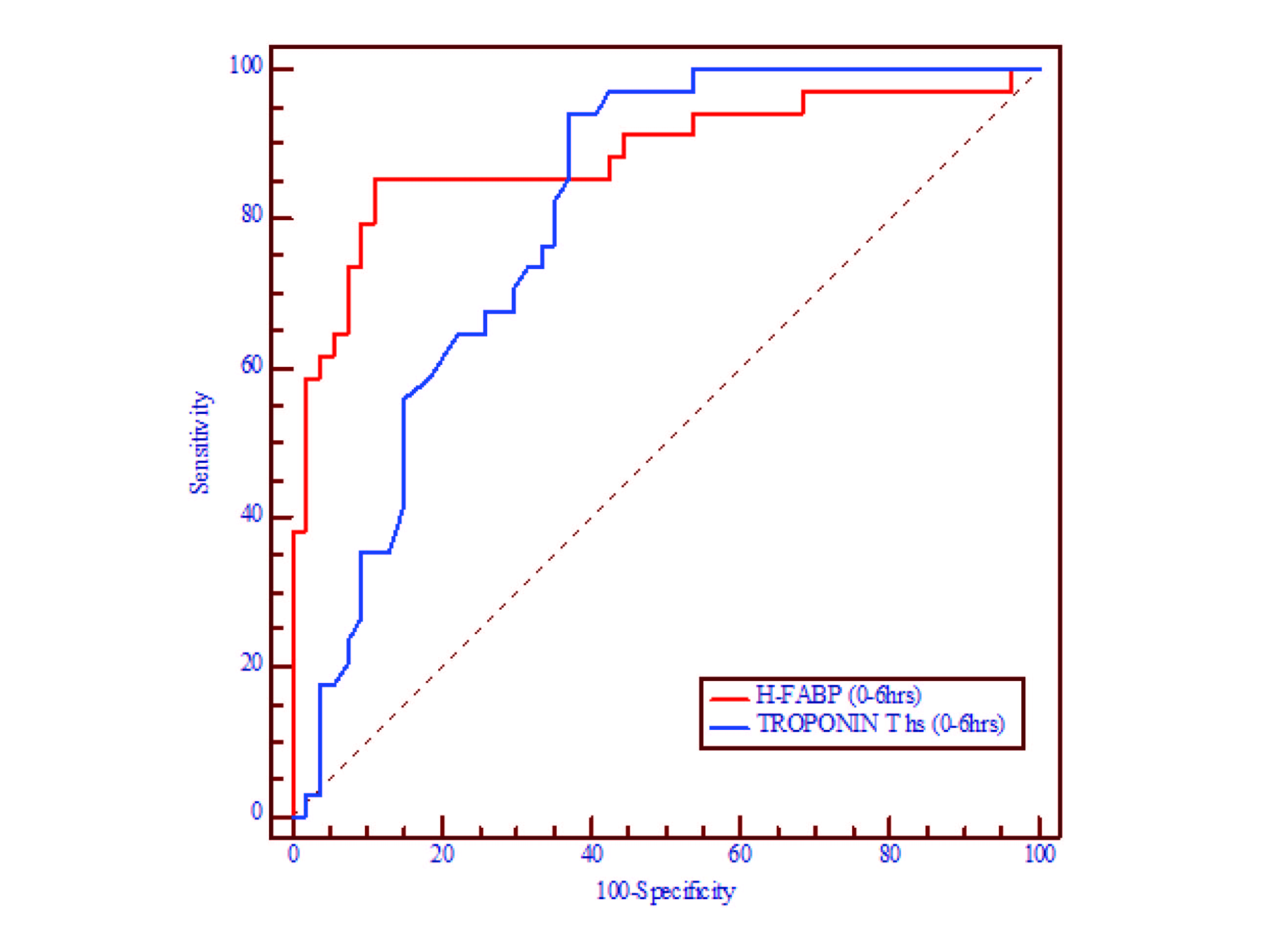
ROC curves were constructed using result obtained from all groups (n=88) to test the performance of hs-TnT and H-FABP for rule-in and rule-out of AMI and earlier prediction in patients with an initially less high sensitive TropT result that turned positive within 6-24 h after admission. AUC for H-FABP was 0.885 (0.79-0.94) and that of hs-TnT in initial six hours was 0.805(0.70-0.88) [Table/Fig-2].
Comparison of ROC curves of hs-TnT and H-FABP during initial 0-6 hours
On considering the cut off as >5.09 ng/mL for H-FABP which was obtained from ROC curve, the sensitivity was 85% (68.9-95.0), specificity was 88% (77.4-95.8), positive predictive value (PPV) was 82% (66.4-93.4) and negative predictive value (NPV) was 90% (79.3-96.9). Positive likelihood ratio (LR+) was 7.08 while negative likelihood ratio was (LR-) 0.17.
While in case of hs-TnT the cut off value was taken is 14 pg/ml. The sensitivity was 94% (80.3-99.3), specificity was 62% (48.7-75.7), PPV was 61% (47.0-74.7) and NPV was 94% (81.3-99.3) during 0-6 hrs which was obtained from ROC curve. LR+ was 2.47 while (LR-) was 0.10. Diagnostic accuracy was determined by obtaining cut off value from AUC. Sensitivity (94%) and NPV (94%) was higher for hs-TnT H-FABP, however, had higher specificity (85%), positive (7.0), and PPV (82%).
If we contemplate hsTnT and H-FABP together for the diagnosis of ACS, Obtained sensitivity was 100%, Specificity was 88.89%, PPV was 85%, NPV was 100%, PLR was 9 and NLR was 0 (zero).
Multi-marker approach for the diagnosis and monitoring of ACS using several biomarkers has been proposed for reconstructing risk stratification and boosting good patient outcomes. In the developing countries like India, cost of the laboratory tests in multi-marker approach might be a drawback. We noticed that sensitivity and NPV was 100% when we used hs-TnT and H-FABP together so, it will help in cut-down mortality among patients with ACS.
Discussion
The introduction of hs-TnT assay has caused both an increased number of diagnosis of AMI and troponin positive non AMI. Under these circumstances necessity calls for the availability of such a marker which helps in the rule in and rule out criteria for AMI especially in early presenters. H-FABP, a novel biomarker, has shown to improve the diagnosis in many studies. H-FABP being a low molecular weight protein has been found to increase in blood sera at the time of ischemia when the myocardial cells are structurally intact. CK-MB is relatively sensitive, but the specificity is in doubt as CK-MB is elevated in any condition following acute or chronic muscle injury, or in patients undergoing a surgical procedure [13] while prospects of IMA looked promising but these ischemic-related increases in IMA may be due to nonspecific injury of tissues other than the myocardium. Modifications to the N-terminal regions of albumin may be induced by mechanisms such as endothelial and extracellular hypoxia, acidosis, free radical injury and sodium/calcium pump disruptions. Those reasons make H-FABP, a promised marker for ACS [14].
Recent studies on H-FABP as an early diagnostic marker in ACS [15–17] showed that H-FABP is either superior to or adds incremental value to troponin in the early diagnosis of ACS, as demonstrated by ROC analyses. The studies compared the performance of H-FABP in combination with prior generation assays for cTn. CT Ruff et al., [18] observed that as compared to the performance of local cTn alone, the addition of H-FABP significantly increased clinical sensitivity for MI and NPV. However results in patients who presented during early hours showed that the addition of H-FABP yielded a NPV of 100 % when combined with sensitive cTnI assay. However, CT Ruff et al., [18] had used old generation cTnI assay and we used new generation hs-TnT This may be one of the reasons why we have got different results from their study.
Kurz et al., [19] study for hs-TnT showed an AUC of 0.817 and H-FABP had an AUC of 0.808. Sensitivity of H-FABP was more than hs-TnT while specificity of hs-TnT was more. Difference in result from our study may be because h-FABP serum levels might have been normalized on admission or during early follow-up with a minor AMI, which might explain the performance of h-FABP. The difference of method for H-FABP measurement might be the second reason for different result we obtained. Inoue et al., [20] compared the diagnostic performance of H-FABP to the latest (5th) generation of TnT, hs-TnT and other markers. The diagnostic accuracy quantified by the area under the receiver operating curve was highest for hs-TnT and H-FABP. Specificity and PPV of H-FABP was far better than hs-TnT in this study which is comparable to our study.
Reiter et al., [21] also studied the H-FABP in early diagnosis of AMI in comparison with hs-TnT and also received the same result like Inoue et al., [20]. Shortt et al., [22] suggested multi-marker approach. In their study, they had less sensitivity and higher specificity for H-FABP than hs-TnT. Most of the study shows that H-FABP is more specific but less sensitive compared to hs-TnT which is much more similar to our study. Seino et al., [23] suggested H-FABP as a novel biomarker to exclude non-AMI patients with <3 h chest pain.
There are minor differences in results of our study from other studies and it might be due to its cross sectional design, limited number of patients involved and different assays (kits) and different guidelines for MI diagnosis have been used in different studies. Few studies have compared old generations of cardiac TnT and TnI with H-FABP, which might be the other reason of variation in results we have received.
Conclusion
The hs-TnT assay is a useful diagnostic test that can be performed to rule out ACS in patients with chest pain. But because of its high sensitivity and less specificity compared to multi-marker approach, it is prone to give false positive results. Due to various non-cardiac ailments contributing for the rise in the high sensitive troponin levels, serial sampling becomes important for making confirmatory diagnosis, especially in early presenters. We conclude that H-FABP measured during early hours of chest pain has good diagnostic value as an adjunct to high sensitive troponin.