Congenital Kyphosis in Thoracic Spine Secondary to Absence of Two Thoracic Vertebral Bodies
Priya Kale1, A. Dhawas2, S. Kale3, A. Tayade4, S. Thakre5
1 Assistant Professor, Department of Radiodiagnosis, MGIMS, Sewagram, Wardha, MS, India.
2 Resident, Department of Radiodiagnosis, MGIMS, Sewagram, Wardha, MS, India.
3 Professor, Department of Radiodiagnosis, MGIMS, Sewagram, Wardha, MS, India.
4 Professor and Head, Department of Radiodiagnosis, MGIMS, Sewagram,Wardha, MS, India.
5 Deputy Superintendent, GMCH, Nagpur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priya Kale, Assistant Professor, Department of Radiodiagnosis, MGIMS, Sewagram, Wardha, MS, India.
E-mail: drsubhasht@rediffmail.com
Congenital thoracic kyphosis at D6-D7 vertebral body level has been encountered in an 18-month-old boy without neurological deficit. The constellation of the spine malformation complex such as incomplete development of the vertebral bodies associated with defective ossification of the thoracic pedicles causing effectively the development of spinal cord injury at the kyphotic level of D6-D7 were present. Congenital kyphosis in thoracic spine secondary to absence of two thoracic vertebral bodies has been reported in a few studies. It is the absence and asymmetry of growth plates that may contribute to a congenital defect. Congenital Kyphosis refers to the normal convex curvature of the spine as it occurs in the thoracic and sacral regions since birth. Congenital kyphosis is an uncommon, but potentially devastating anomaly of the spine. It is one of the important aetiology for spinal cord compression leading to further neurological complications. Congenital kyphosis although rare, is more associated with neurological complication. Early identification not only helps in understanding its natural history but also helps in deciding its management.
Kyphoscoliosis, Neurological, Sclerotome
Case Report
An 18-month-old male came with history of progressive swelling over back region secondary to kyphosis at D6-D7 vertebral body level. At birth he had no abnormality. His mother first noticed swelling at the age of six months. Birth history was unremarkable. His milestones were appropriate for his age. Patient began to walk at the age of 15 months and no motor developmental delay was observed. He had normal language development. Overall neurological status was intact. On clinical examination he had kyphosis of thoracic spine. There was no neurological deficit or cutaneous stigmata. Later he was referred to Department of Radio Diagnosis for evaluation of kyphosis. He was subjected to CT and MRI.
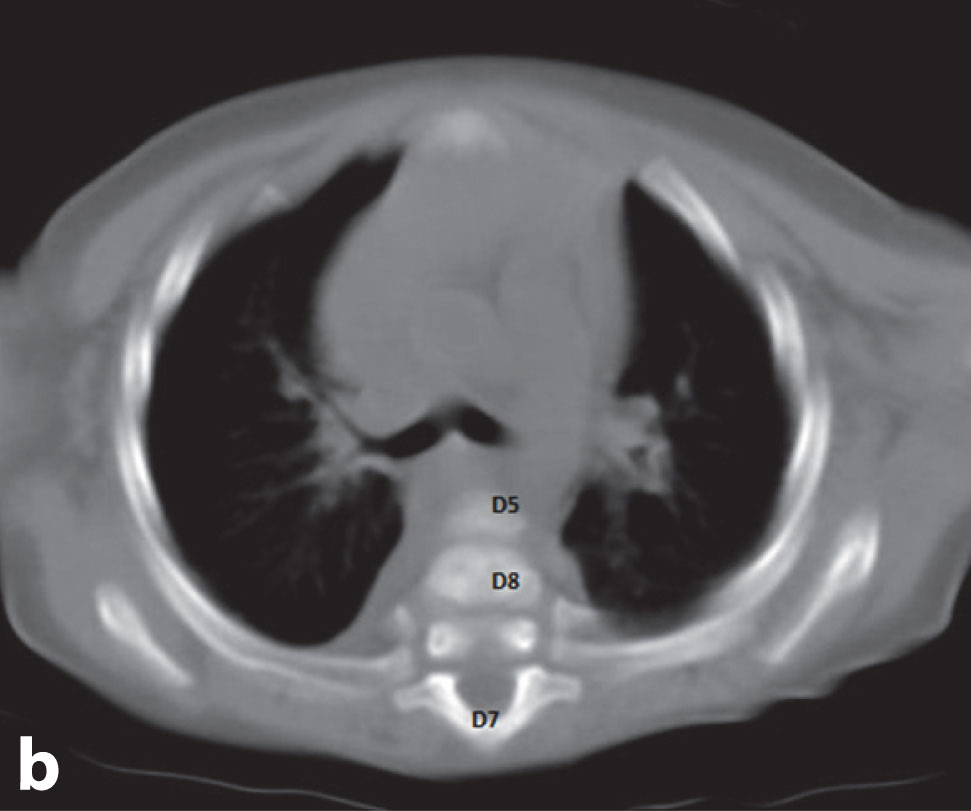
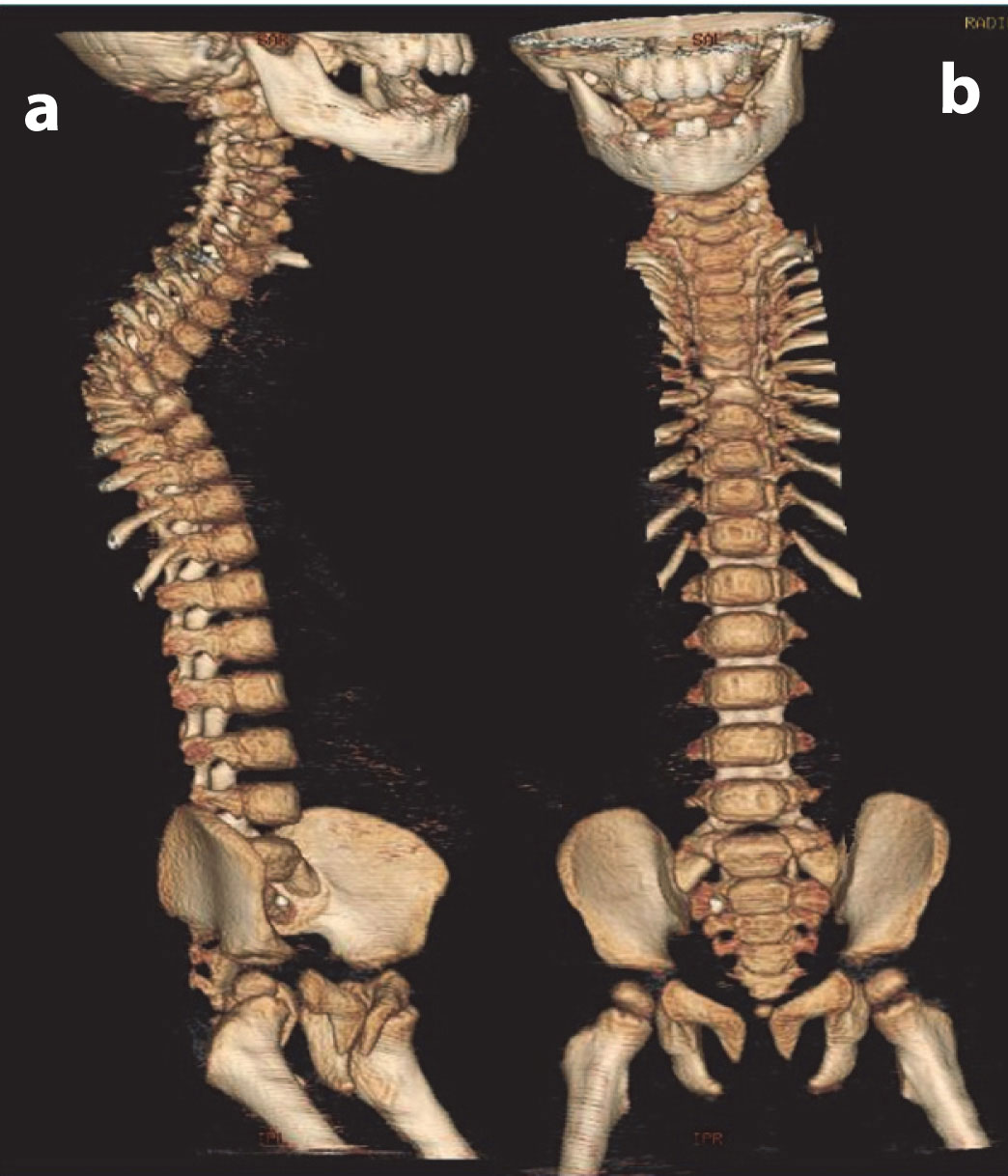
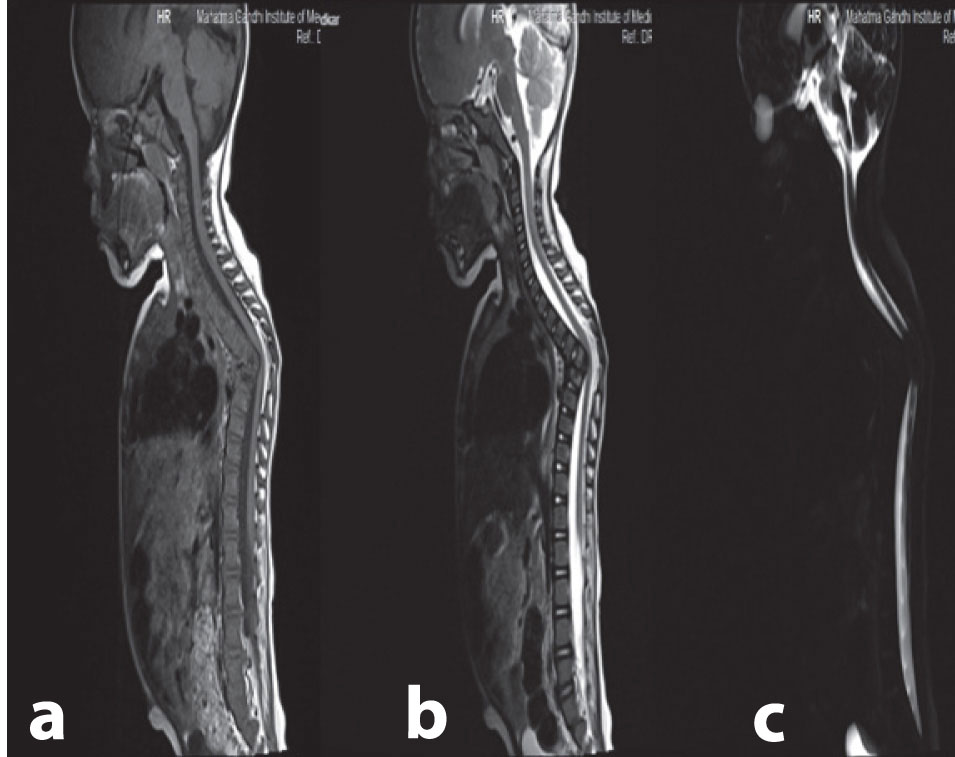
[Table/Fig-1a,b&2a,b] shows that CT showed kyphosis in thoracic spine with absence of D6, D7 vertebral bodies. However their posterior elements were normal. Angle of kyphotic deformity was approximately 700. [Table/Fig-3a&b] T1W and T2W sagittal images of thoracic spine show kyphosis with absence of vertebral body of D6 and D7 vertebra. [Table/Fig-3c] Myelography show obliteration of subarachnoid space at the level of kyphosis.
Sagittal reformatted images of CT whole spine show kyphosis with absence of vertebral body of D6 and D7 vertebra, D5 vertebra is facing downwards and resting on D8 vertebra

Axial CT spine image at the level of absent D6 and D7 vertebra shows angulated D5 and D8 vertebra with posterior elements of D7 vertebra
3D volume rendered images of same patient show thoracic kyphosis with absence of vertebral body of D6 and D7 vertebra and presence of posterior elements
(a,b) T1W and T2W sagittal images of thoracic spine show kyphosis with absence of vertebral body of D6 and D7 vertebra (c) Myelography show obliteration of subarachnoid space at the level of kyphosis
MRI confirmed the same findings. However, no intra-spinal abnormality was detected. Anterior subarachnoid space was obliterated at the level of kyphotic deformity which was indenting on spinal cord. There was no compression on spinal cord.
Discussion
Cases of congenital kyphosis due to defect in vertebral body formation have been reported. However, congenital kyphosis due to complete lack of vertebral body formation is very rare. Here, we report a case of congenital kyphosis due to absence of D6 and D7 vertebral bodies with intact posterior elements without any other congenital defect.
It is documented that the notochord and somites are the most significant structures responsible for the development of the future vertebral column [1]. Each somite develops into two parts: a sclerotome and adermomyotome. The cells of the sclerotome are responsible for the formation of the spine [2]. One complete vertebra requires two somites to interact properly with each other in order to develop normally. Fusion of parts of the adjacent sclerotomes creates the centrum, which further develops into the vertebral body. The centrum allows bone to continually develop around it. The cells that initially migrated adjacent to the neural tube, rather than the notochord, develop into the neural arches, which serve to protect the spinal cord, vessels and nerve roots. The centrum and the two halves of the vertebral arches develop separately and must fuse to one another. Ossification centers can be found in three main areas in the vertebrae: one in the centrum and one on each side of the vertebral arch [1,2].
Available literature reveals that bone ossified from the secondary centres will contribute to the formation of growth plates. It is the absence and asymmetry of growth plates that may contribute to a congenital defect. It is evident from the literature that, defects in both chondrification and ossification cause several of the most common congenital abnormalities. Molecular signals from the notochord are responsible for differentiation and eventually, chondrification and ossification of the vertebrae. Abnormal mesenchyme, an abnormal notochord and genetic abnormalities affecting signaling can predispose a foetus to abnormal development of the bony skeleton [3].
TKim HW et al., suggested that there are six common forms of deficiency of the centrum, depending on location of defect in them resulted in pure kyphosis or kyphoscoliosis [4].
Congenital kyphosis was first classified into failure of vertebral body formation and failure of segmentation [5]. Winter et al., classified the deformity into three type I - failure of formation, type II - failure of segmentation and type III - mixed failure of formation and segmentation [6]. In a series by Mc master and Singh, anomalies were classified into four groups, 65% due to anterior failure of vertebral body formation, 20% segmentation defects , 10% mixed anomalies and 5% could not be classified. In their study, type I deformity was further classified into posterolateral quadrant vertebra (35%), posterior hemivertebra (7%), butterfly vertebra (13%) and anterior wedged vertebrae (5%) [7].
Dubosset classified failure of formation into: two types: Type I is partial failure with a well aligned spinal canal and intact posterior arch and type II is partial failure with dislocated canal [4]. Zeller and colleagues [8] called it congenital vertebral displacement and congenital dislocated spine respectively to describe deformities in which anterior and posterior elements were abnormal with posterior displacement of anomalous vertebrae.
Type I is most common in thoracolumbar region followed by upper thoracic and least common in lumbar region [5]. Segmentation failure is most commonly seen in thoracic spine followed by thoracolumbar spine [9]. Type I is more associated with progression and neurological complications as compared to type II. The rate of neurological complications with congenital kyphosis is about 18%. Type I progresses about 7o per year, more rapid during growth spurt [4].
Anomalies associated with congenital kyphosis are that of lower limb, cardiac and renal [10]. Cutaneous stigmata can also be present. Another entity is segmental spinal dysgenesis which is a rare anomaly characterised by localised agenesis or dysgenesis of the lumbar or thoracolumbar spine, severe congenital kyphosis or kyphoscoliosis and focal abnormalities of underlying spinal cord and nerve roots [10].
In our case, kyphosis was due to absence of two thoracic vertebral bodies with normal posterior elements. No other renal or spinal anomaly was present. This is a very rare case as the cause of congenital kyphosis is due to aplasia of vertebral bodies. Hypoplasia and aplasia of vertebral body may be due to spectrum growth deficits of the centrum during late stages of chondrification and ossification, when there is rapid increase in vertebral size [4]. Principle of treatment in congenital kyphosis is early fusion to prevent severe deformity and neurological deficits.
Conclusion
Congenital kyphosis although rare, is more associated with neurological complication. Early identification not only helps in understanding its natural history but also helps in deciding its management.
[1]. O’Rahilly R, Human embryology and teratology 1996 New YorkJohn Wiley & Sons [Google Scholar]
[2]. Moore K, Persaud TVN, The developing human: clinially oriented embryology 1998 6th edPhiladelphiaW.B. Saunders Company [Google Scholar]
[3]. Kaplan K M, Embryology of spine and associated congenital anomaliesThe Spine Journal 2005 5:564-76. [Google Scholar]
[4]. Kim HW, Weinstein SL, Atypical congenital kyphosis Report of two cases with long term follow upJ Bone Joint Surg(Br) 1998 80-B:25-29. [Google Scholar]
[5]. Herkewitz HN, Pediatrickyphosis: Scheurmanns disease and congenital deformity, Harry N. Herkowitz 2011 6th editionPhiladelphiaElsevier Saunders:451-68. [Google Scholar]
[6]. Winter RB, Moe JH, Wang JF, Congenital kyphosis: Its natural history and treatment as observed in a study of one hundred and thirty patientsJ Bone Joint Surg Am 1973 55:223-56. [Google Scholar]
[7]. McMaster MJ, Singh H, Natural history of congenital kyphosis and kyphoscoliosis: A study of one hundred and twelve patientsJ Bone Joint Surg Am 1999 81:1367-83. [Google Scholar]
[8]. Zeller RD, Ghanem I, Dubosset J, The congenital dislocated spineSpine 1096 15(10):1235-40. [Google Scholar]
[9]. Mayfield JK, Winter RB, Bradford DS, More JH, Congenital kyphosis due to defects of anterior segmentationJ Bone Joint Surg Am 1980 62:1291-301. [Google Scholar]
[10]. Lonstein JE, Congenital spine deformities: scoliosis, kyphosis and lordosisOrthop Clin North Am 1999 30(3):387-405. [Google Scholar]