Share of Tobacco Related Cancers: Gender and Time Gaps-Indian Scenario
Atul Juneja1, Tulsi Adhikari2, Arvind Pandey3, Shashi Sharma4, Ashok Sehgal5
1 Scientist C, National Institute of Medical Statistics (ICMR), New Delhi, India.
2 Scientist D, National Institute of Medical Statistics (ICMR), New Delhi, India.
3 Director, National Institute of Medical Statistics (ICMR), New Delhi, India.
4 Scientist E, Institute of Cytology and Preventive Oncology (ICMR), Noida, UP, India.
5 Scientist G, Institute of Cytology and Preventive Oncology (ICMR), Noida, UP, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Atul Juneja, National Institute of Medical Statistics (ICMR), Ansari Nagar, New Delhi-110029, India.
E-mail: atul_juneja@hotmail.com
Introduction: Cancer is one of the leading causes of mortality in Indian population with control approach of varied kind which the health system of the country needs to prioritize. The tobacco related cancer which account for major share of all the cancers could be largely controlled through primary prevention a strategy effective in terms of resources hence take priority in terms of cancer control activities. It would be worthwhile to study the cancer of sites and relative magnitude of the cancers which are tobacco related and are amenable for prevention.
Materials and Methods: The age specific cancer incidence rates of cancer as available from the consolidated reports of the National Cancer Registry Program of Indian Council of Medical Research for the years 1990-96 an 2001-04 were utilized for computing proportion of tobacco related cancers which included population based cancer registries at Bangalore, Bhopal, Barshi a rural registry in Maharashtra, Chennai, Delhi and Mumbai. As defined cancer of the sites oral cavity, lip, tongue, oropharynx, hypopharnx, pharynx, oesophagus, larynx, lung, urinary bladder were considered as tobacco related cancers.
The statistical evaluation of proportion of tobacco related cancers between two time periods under consideration was carried out by proportion test.
Results: There was a significant decline of proportion of tobacco related cancers from 1990-96 to 2003 for all the registries except Bhopal where around 50% of the total cancers attributed to tobacco habits for the two time periods under consideration. The Barshi also reported a decline but was not statistically significant. In females the proportion of tobacco related cancers ranged between 17% in Bangalore 10% in Delhi for the two time periods under review. All the registries showed significant decline in proportion of tobacco related cancers for the periods under consideration, except Delhi and Bhopal, while rural registry at Barshi revealed an increase of 3.3 %. The gender difference of the proportion of tobacco related cancers ranges between 19.8% to 34% during the period 1990-96, while it was 18.5% to 35% for the period 2001-03. While examining the difference between gender gap between the two time periods, the results from Mumbai registry revealed significant decline.
Cancer, Gender gap, Proportion-tobacco related cancers, Tobacco
Introduction
With the demographic changes, non communicable diseases like cancer have become a matter of concern in developing countries like India with the health delivery system [1]. Cancer of various sites has multi-faceted control strategies requiring different magnitude of resources as issue with the health planners. Now cancer is one of the Leading cause of mortality in Indian population with control approach of varied kind which the health system of the country needs to prioritize [2]. The disease could be prevented or detected early, i.e., in the localized state where complete cure is possible through secondary prevention. Cancer of the uterine cervix which is one of the leading malignancy could be efficiently checked through secondary prevention by choosing appropriate screening strategy depending on resources and to an extent, by modifying the behavioral risk factors [3,4]. The tobacco related cancer which account for major share of all the cancers could be largely controlled through primary prevention a strategy effective in terms of resources hence take priority in terms of cancer control activities. Hence, tobacco related cancers deserve a closer look in terms magnitude and share of load could be one of the approaches in terms of having prioritization of health delivery resources. In developed countries like USA, tobacco use already accounts for large share of cancer deaths [5]. In India, tobacco related cancer deaths account for 42% and 18% among males and females respectively in age group of 30-69 y [6]. As per the studies conducted in different regions in India, the tobacco habits widely vary between men and women [7,8].
It would be worthwhile to study the cancer of sites and relative magnitude of the cancers which are tobacco related and are amenable for prevention. It was interestingly observed from the study by Zang which examined the gender difference between the risks of lung cancer with smoking considering the dose response, it was observed that risk was 1.2 to 1.7 times higher for women than men [9]. Hence, it is important to consider the gender issue in tobacco related cancers in Indian settings.
The present communication attempts to evaluate the change in proportion of tobacco related cancer between two time periods for male and females based on the data from National Cancer Registry Program of India. Effort has also been made to study the change in the proportion of tobacco related cancers between male and females for the two time periods under consideration with statistical evaluation. The computations have been carried out for the population based cancer registries located at Bangalore, Barshi, Bhopal Chennai, Delhi and Mumbai. Of these, the registry at Barshi in Maharashtra represents rural population while rest is urban registries.
Materials and Methods
The age specific cancer incidence rates as available from reports of the National Cancer Registry Program of Indian council of Medical Research for the years 1990-96 and 2001-03 were utilised for computing proportion of tobacco related cancers [10,11]. As defined cancer of the sites oral cavity, lip, tongue, oropharynx, hypopharnx, pharynx, oesophagus, larynx, lung, urinary bladder were considered as tobacco related cancers.
The statistical evaluation of proportion of tobacco related cancers between two time periods under consideration was carried out by proportion test. It may be mentioned that the incidence data in the consolidated reports Population based cancer registries of National Cancer Registry Program of ICMR 2001-04 pertains for the period 2001-03.
Statistical Analysis
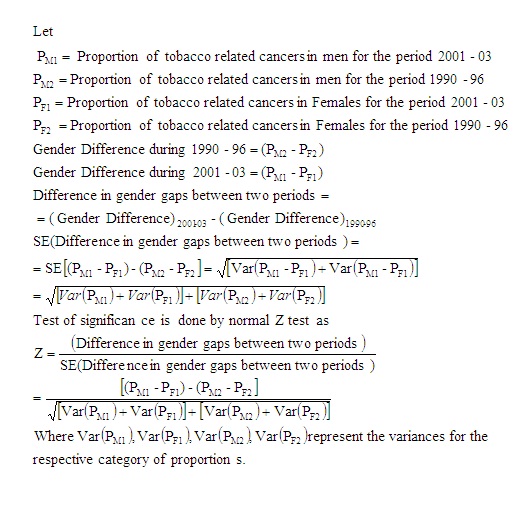
The change in the proportion of tobacco related cancers was estimated through proportion test. The computation of standard error of the gender difference of tobacco related cancers between the two periods was computed as described by Sharma et al., [12]
Results
Comparison of Proportions among Males
The proportion of tobacco related cancers among males ranged between 37% in Bangalore to 50 % in Bhopal during the period 1990-96 while during the period 2001-03 it ranged between 34% to 50% in the same regions i.e. Bangalore and Bhopal. Thus, there was a significant decline among tobacco related cancers from 1990-96 to 2001-2003 for all the registries except Bhopal. It is also observed that in Bhopal, 50% of the total cancers attributed to tobacco habits for the two time periods under consideration. The Barshi also reported a decline but was not statistically significant [Table/Fig-1].
Change in the tobacco related cancers between two periods-Male
| Registry | Tobacco related cancers-1990-96 (%) (Total cancers) (1) | Tobacco related cancers-2001-03 (%) (Total cancers) (2) | Difference (d) (2) – (1) | p | 95% CI |
|---|
| Banglore | 37.04 (10240) | 34.66 (6112) | -2.37 | 0.002 | -3.90 to -0.85 |
| Barshi | 40.75 (638) | 39.42 (317) | -1.32 | 0.5 | -7.91 to+ 5.27 |
| Bhopal | 50.01(2539) | 50.34 (1595) | 0.32 | 0.85 | -2. 81 to+ 3.45 |
| Chennai | 43.61(11366) | 41.02 (6214) | -2.59 | 0.009 | -4.11 to -1.07 |
| Delhi | 38.23 (26218) | 36.93 (16112) | -1.30 | 0.007 | -2.25 to -0.35 |
| Mumbai | 44.68 (28953) | 40.57(13727) | -4.11 | <0.001 | -5.11 to -3.11 |
Comparison of Proportion among Females
In females, the proportion of tobacco related cancers ranged between 17% in Bangalore to 10% in Delhi for the two time periods under review. All the registries showed significant decline in proportion of tobacco related cancers, except Delhi and Bhopal, while rural registry at Barshi revealed an increase of 3.3%. (p=0.10) [Table/Fig-2]. The number of cases studied at Barshi registry is much less than the other urban registries.
Change in the tobacco related cancers between two periods-female
| Registry | Tobacco related cancers-1990-96 (%) (Total cancers) (1) | Tobacco related cancers-2001-03 (%) (Total cancers) (2) | Difference (d) (2) – (1) | p | 95% CI |
|---|
| Banglore | 17.29 (11740) | 16.17 (7247) | -1.1 | 0.05 | -2.21 to-0.03 |
| Barshi | 10.18(766) | 13.48 (356) | 3.3 | 0.10 | -0.84 to +7.43 |
| Bhopal | 15.69 (2250) | 14.76 (1409) | -0.93 | 0.43 | -3.31 to +1.48 |
| Chennai | 16.83 (12355) | 15.44(6689) | -1.3 | 0.01 | -2.49 to -0.29 |
| Delhi | 10.4(25861) | 10.07(15044) | -0.33 | 0.28 | -0.94 to +0.28 |
| Mumbai | 16.96 (27091) | 15.03 (13792) | -1.93 | <0.001 | -2.66 to -2.62 |
Comparison of the Difference in Gender Gaps
The exercise also attempted to examine the difference between proportion of tobacco related cancers for male and female (gender difference) between two time periods. Among all the registries, the gender difference of the proportion of tobacco related cancers ranged between 19.75% to 34.33% during the period 1990-96, while it ranged between 18.5% to 35.6% for the period 2001-03.
While examining the difference between gender gap between the two time periods, the results from Mumbai registry revealed significant decline [Table/Fig-3]. This was mainly as a result of significant decline of proportion of tobacco related cancers from 1990-96 to 2001-03 among males, thus making the proportion of tobacco related cancers closer between male and female in 2001-03. The results from Chennai indicate the change of 1.3% (p=0.1) while Delhi 1%. [Table/Fig-3] presents the gender gap along with statistical significance and 95% Confidence intervals.
Difference of difference of proportion of tobacco related cancers between male and female for two periods
| Registry | D1(m-f ) for 1990-1996 | D2(m-f ) for 2001-2003 | D=D2-D1 | p | 95%CI |
|---|
| Banglore | 19.75 | 18.50 | -1.2 | 0.188 | -3.11 to +0.61 |
| Barshi | 30.56 | 25.94 | -4.6 | 0.24 | -12.40 to +3.16 |
| Bhopal | 34.33 | 35.60 | 1.25 | 0.553 | -26.8 to+ 5.18 |
| Chennai | 26.78 | 25.57 | -1.3 | 0.103 | -3.08 to +0.66 |
| Delhi | 27.83 | 26.85 | -0.97 | 0.09 | -2.10 to +0.15 |
| Mumbai | 27.72 | 25.54 | -2.18 | 0.0003 | -3.57 to -1.07 |
Discussion
Tobacco related cancers are mainly considered for the sites viz. oral cavity, lip and tongue, oropharynx, hypopharynx, pharynx oesophagus, larynx, lung and urinary bladder. As per data available from National Cancer Registry Program, tobacco related cancers in men account for about 40 to 50% of all cancers. In females the tobacco related cancers account for around one fifth of Cancers [10,11].
The current results are based on data from five population based cancer registries which include one rural registry at Barshi. Since the cancer registries are mainly based in urban settings the result of one registry may not be representative of other rural settings. The issue of tobacco related cancer becomes all the more important in view of the recent results of WHO which predicts that tobacco related deaths may exceed 1.5 million by 2020 [13]. This is based on certain assumptions since data on tobacco consumption at national level is not available. Even if the assumptions do not hold well, the estimates only as a result of population growth and demographic transition would be enough to scare group responsible for health delivery.
Based on estimates of WHO, the prevalence of tobacco consumption is 65% and 33% in men and women respectively in India. Some studies have highlighted that tobacco habits in females range from 15% in Gujarat to more than 80% in Andhra Pradesh [7].
In the present study we have tried to evaluate the proportion of tobacco related cancers in men and women for the two time periods and further study the gender gap for the two reference periods- mainly in order to know trends in women as in men it any way very high. It was observed that the gender gap between the two periods remained the same as there was equal decline in proportion of tobacco related cancers in men and women except for Mumbai where the gap became narrower in 2001-03. In view of the changing society and expected change in behavior towards tobacco habits it was important to look at change in magnitude of tobacco related cancers.
One of the studies carried out to study the role of intervention in reducing the tobacco habits in India revealed encouraging results [14]. The results indicated that suitable interventions can help, to reasonably keep a check on the problem of cancer due to tobacco (since it is 50% in men) and at least not allowing it to grow beyond its natural increase because of population dynamics. With intensive health educational campaign can help to combat in controlling significant number of cancer cases which are tobacco related.
It is not only active tobacco habit which is a matter of concern but also passive exposure which a person gets by occupation i.e. working in tobacco industry tobacco fields which has the same effect as that of active consumption [15].
In India the tobacco control issues need to be targeted not only from cancer point of view but from other heath dimensions such as pregnancy related hazards in females and sexual dysfunction in men which may convince the tobacco user to quit.
It is important to mention that tobacco habits in females have not reached what are observed in developing countries and can be checked with suitable interventions. Thus integrating the cancer control programs with other ongoing programs could be one of the ways to achieve it optimally. In fact WHO has initiated tobacco control programs particularly in developing countries. This has been initiated in our country but needs to be intensified [16]. This is feasible since it targets only through primary prevention.
The current communication targeted the magnitude of the tobacco related cancers in terms of relative share rather than absolute incidence. We were concerned only about the shift of the proportion. It might be important to know what kind of cancers were being added if there was a decline in tobacco related cancers but was found beyond the scope of objective of this paper.
[1]. http://www.inctr.org/about-inctr/cancer-in-developing-countries[cited 2014 November 02] [Google Scholar]
[2]. Gupta PC, Ray CS, Tobacco related cancer –It’s impact on Health EconomyHealth Administrator 2005 27(1):85-92. [Google Scholar]
[3]. Juneja A, Sehgal A, Mitra AB, Pandey A, A survey on risk factors associated with cervical cancerIndian J Cancer 2003 40(1):15-22. [Google Scholar]
[4]. Juneja A, Sehgal A, Sharma S, Pandey A, Cervical cancer Screening in India: Strategies RevisitedInd J Med Sci 2007 61(1):35-42. [Google Scholar]
[5]. http://www.who.int/mediacentre/factsheets/fs339/en/index.html[cited 2014 May 02] [Google Scholar]
[6]. Dikshit R, Gupta PC, Ramasundarahettige C, Gajalakshmi V, Aleksandrowicz L, Badwe Cancer mortality in India: a nationally representative surveyLancet 2012 379(9828):1807-16. [Google Scholar]
[7]. Bala DV, Bodiwala ILA N, Patel DD, Shah PM, Epidemiological Determinants of Tobacco Use In Gujarat State, IndiaIJCM 2006 31(3):173-76.(Downloaded free from http://www.ijcm.org.in [November 02, 2014] [Google Scholar]
[8]. Sinha D, Gupta PC, Pednekar M, Tobacco use in rural area of Bihar, IndiaIJCM 2003 28:167-70. [Google Scholar]
[9]. Zang EA, Wander EL, Differences in Lung Cancer Risk Between Men and Women: Examination of the EvidenceJNCI 1996 88(3/4):183-92. [Google Scholar]
[10]. National Cancer Registry Program Consolidated Report of PBCR 1990-1996. ICMR, New Delhi 2001 [Google Scholar]
[11]. National Cancer Registry Program Consolidated Report of PBCR 2001-2004. ICMR, New Delhi 2006 [Google Scholar]
[12]. Sharma PP, Singh P, Kumar A, A study of gender differentials in the prevalence of tuberculosis based on NFHS-2 and NFHS-3 dataIJCM 2010 35(2):230-57. [Google Scholar]
[13]. Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L, Tobacco use in India: prevalence and predictors of smoking and chewing in a national cross sectional house hold surveyTob Cntrol 2003 12:e 4doi:10.1136/tc.12.4.e4 [Google Scholar]
[14]. http://icmr.nic.in/cancer.pdf[cited 2014 May 02] [Google Scholar]
[15]. http://www.who.int/tobacco/resources/publications/wntd/2009/materials/ brochure/en/index.html [cited 2014 May 02] [Google Scholar]
[16]. Editorial Tobacco Control in IndiaIndian J Med Res 2006 123:579-82. [Google Scholar]