Accidental Subclavian Artery Catheterization During Attempted Internal Jugular Central Venous Catheter Placement: A Case Report
Bharat Paliwal1, Manoj Kamal2, Anamika Purohit3, Kirti Rana4, Dilip Singh Chouhan5
1 Assistant Professor, Department of Anesthesiology, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
2 Associate Professor, Department of Anesthesiology, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
3 Medical Officer, District Hospital, Paota, Jodhpur, Rajasthan, India.
4 Associate Professor, Department of Radiodiagnosis, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
5 Professor, Department of Anesthesiology, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bharat Paliwal, Sector-23, House No. 14, Choupasni Housing Board Colony, Pal Road, Jodhpur, Rajasthan- 342008, India.
E-mail: docbpali@gmail.com
Central venous catheter placement has been routinely employed for anesthetic and intensive care management. Despite proper technique used and expertise complications do occur; some of which are related to catheter misplacements. We report a case in which subclavian artery was accidently catheterized during attempted internal jugular venous cannulation.
Central venous catheters, Catheter misplacements, Internal jugular vein cannulation, Subclavian artery catheterization
Case Report
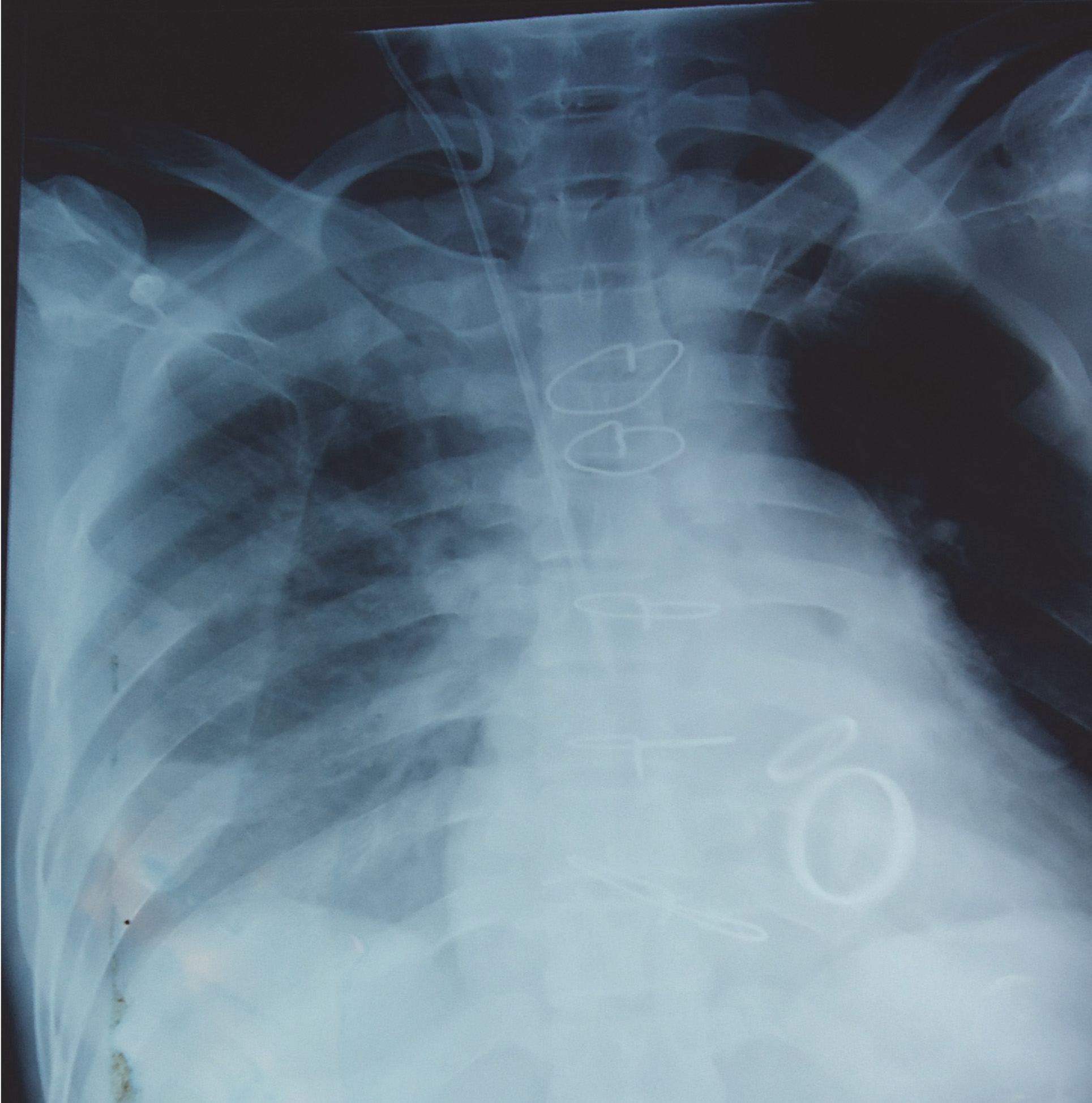
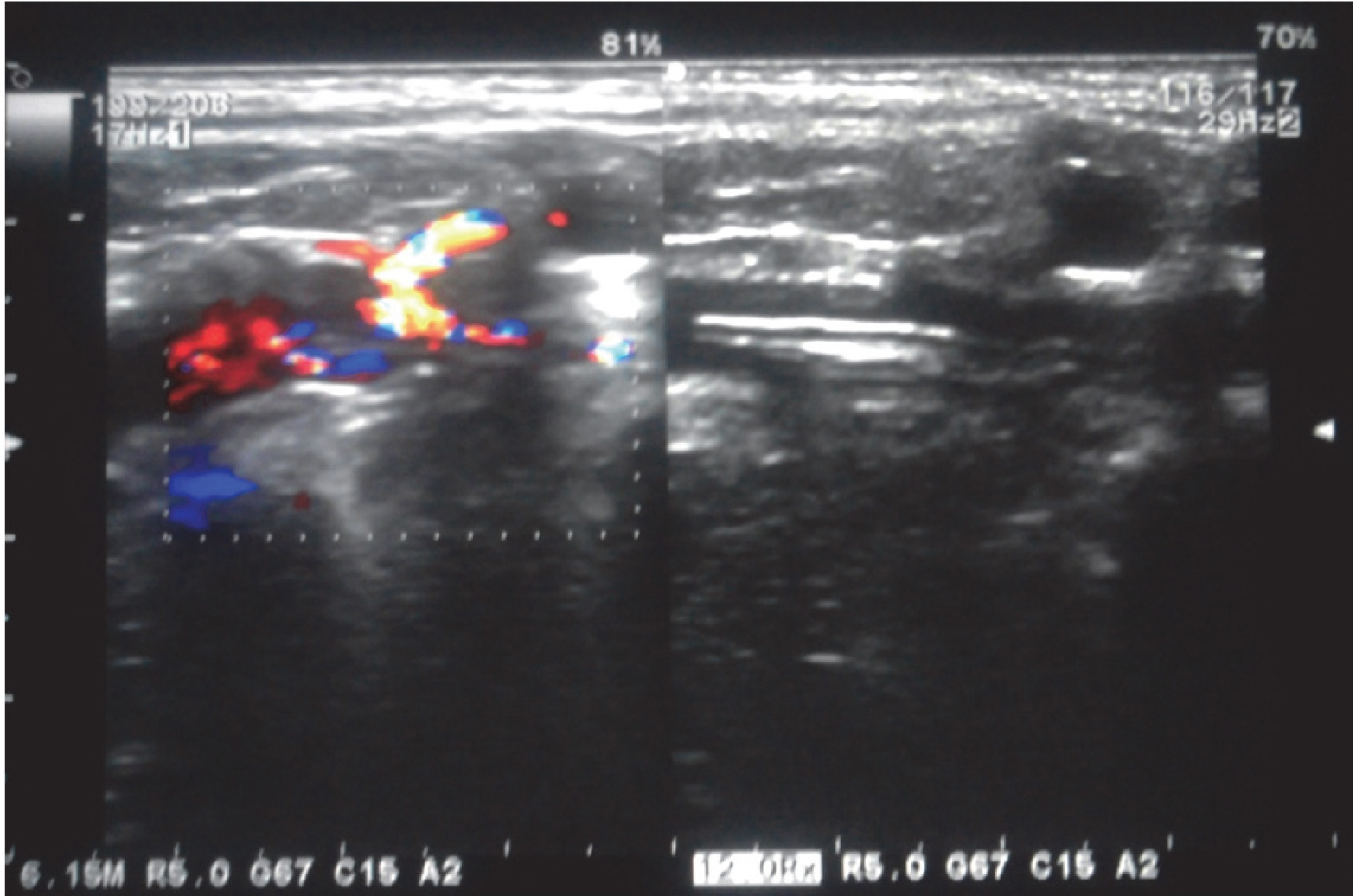
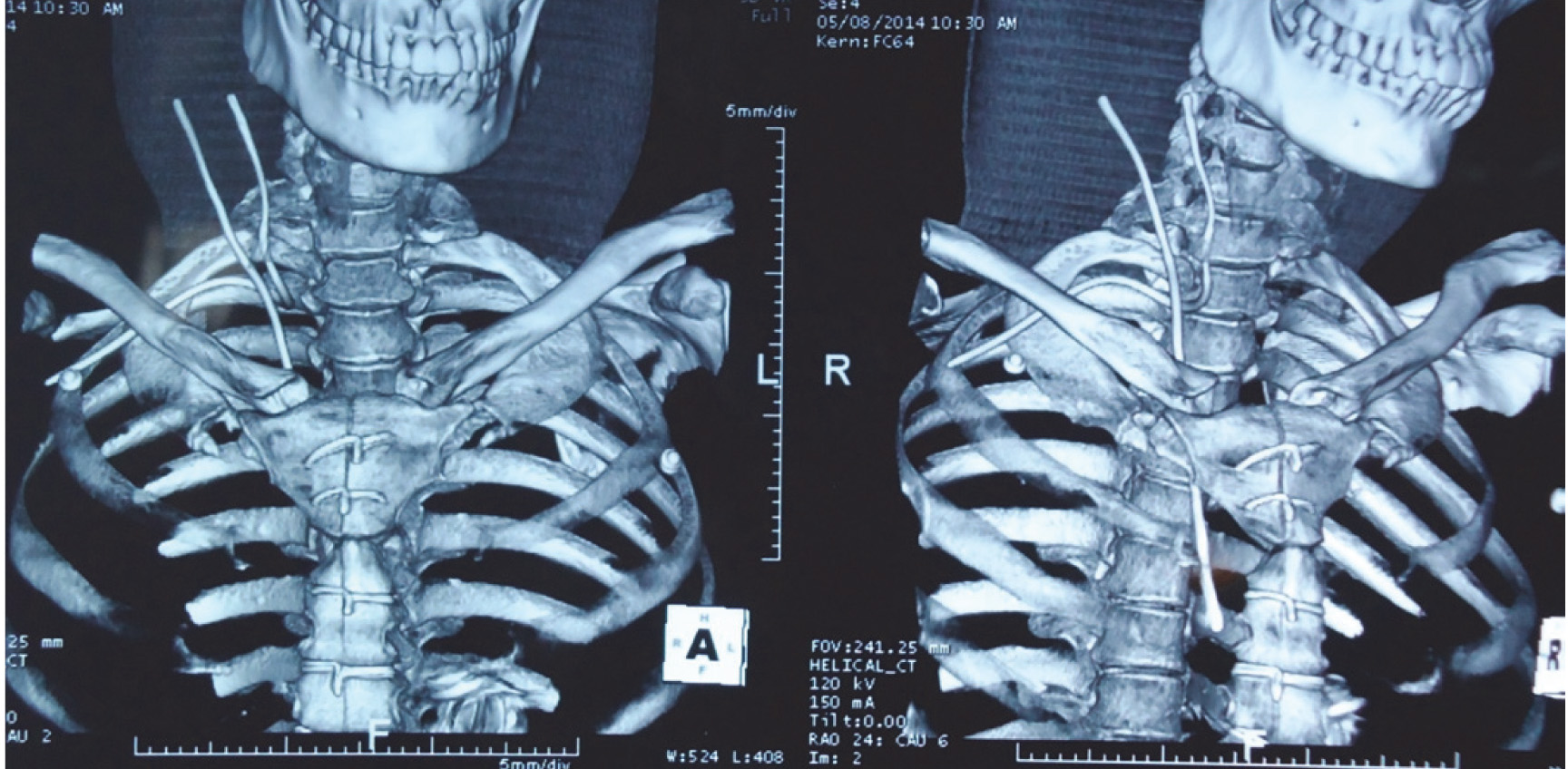
A 48-year-old man with severe mitral stenosis and moderate aortic stenosis was posted for valvular replacement. After securing peripheral venous access with 16 gauge i.v. cannula in right basilic vein and arterial line with 20 gauge arterial cannula in left femoral artery patient was given general anesthesia. Patient was placed in trendelenburg position (15°) and neck prepared aseptically for right internal jugular vein (IJV) catherization. Using anatomical landmarks and the apical approach IJV was located with 25 gauge finder needle and dark, non-pulsatile blood was aspirated. This was followed by puncture with 18 gauge Y-shaped needle attached to a syringe. Smooth aspiration of not so bright red blood was accomplished with no spontaneous filling of the syringe with blood. After inserting guide wire without resistance the vessel was dilated and a 15 cm, 7 Fr triple lumen catheter was placed using Seldinger technique. When the transducer was connected for central venous pressure (CVP) monitoring, we noted arterial waveform on monitor with pressure of 94/64 mmHg [Table/Fig-1]. There was also spontaneous filling of transducer line with blood and visible arterial pulsations [Table/Fig-2]. The anatomical proximity of carotid artery to IJV made us to think that carotid artery was the vessel being catheterized. The catheter was left in situ and another attempt was taken to secure right IJV which was successful. After completion of surgery patient was shifted to ICU and Chest X-ray was done. Chest X-ray showed that one of the catheters was abnormal in location [Table/Fig-3]. Colour Doppler [Table/Fig-4] and computed tomography of thorax [Table/Fig-5] revealed cannulation of subclavian artery. After correction of patient’s elevated international normalized ratio (INR), catheter was removed in operation theatre on postoperative day 2 in presence of vascular surgeon and direct pressure applied. No cardiovascular or neurological complications related to arterial cannulation were noted.
Waveform from central catheter similar to arterial waveform
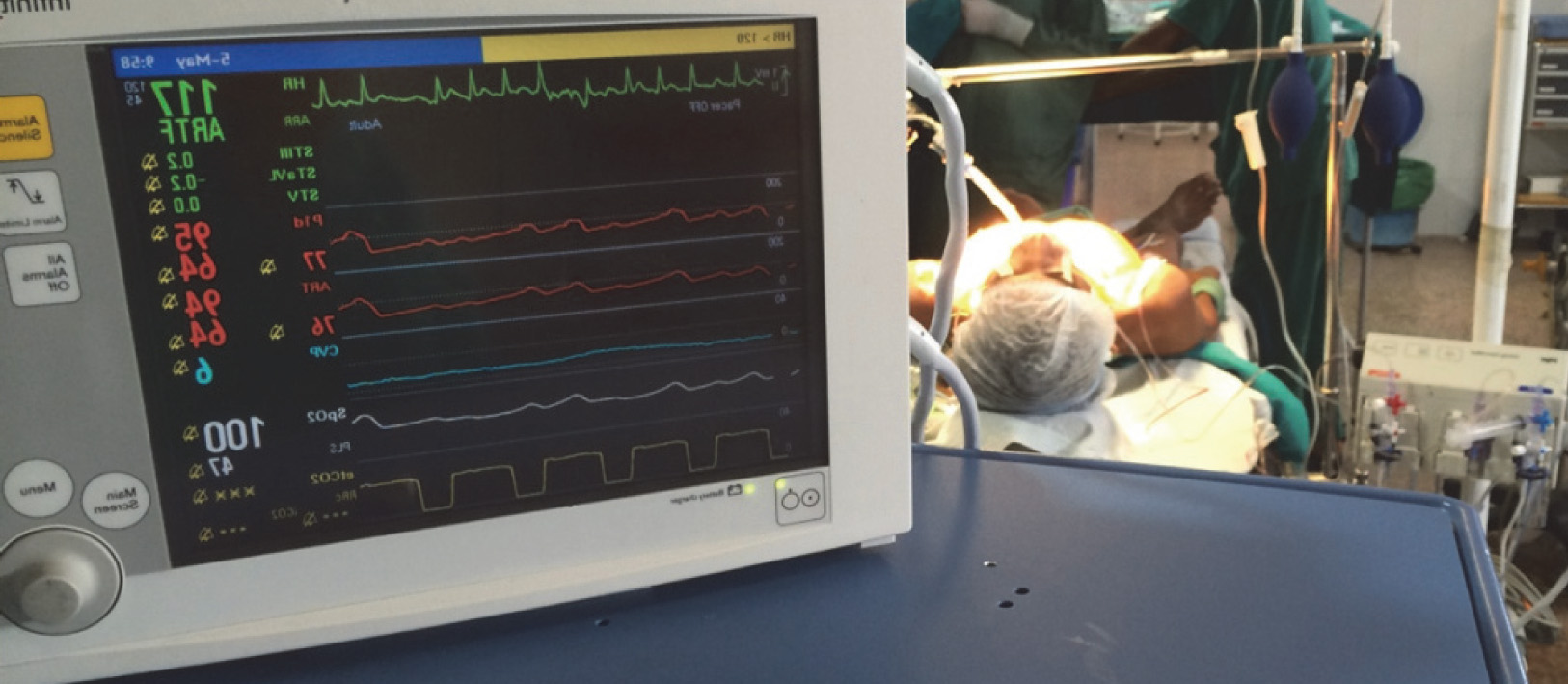
Upper catheter(blue)placed in subclavian artery showing filling of transducer line with blood

Chest X-ray showing position of both catheters
Colour Doppler showing catheter in subclavian artery
CT thorax showing position of both catheters
Discussion
Central venous catheter (CVC) misplacements have been reported in literatures. This case reports misplacement of CVC into subclavian artery while securing IJV. Case reports of subclavian artery catheterization during subclavian vein cannulation and of carotid artery catheterization during IJV cannulation [1] have been reported. Also subclavian artery has been reported to be injured during IJV catheterization [2] but authors could not find case report of subclavian artery catheterization during IJV cannulation. Hence presented as the first report of its kind. Use of IJV for CVP monitoring, fluid and blood products administration and hemodynamic monitoring are in routine practice. The right IJV has been the preferred site for central venous access because of its easily identifiable landmarks, short course to the junction of the superior vena cava and right atrium, and easy accessibility. Even though it is a relatively simple procedure in well-trained hands, it is not without complications. Trauma to nearby nerves or arteries [1,3] is one of the common complications of IJV cannulation. Arterial cannulation is associated with atherosclerotic plaque dislodgement, stroke, hemothorax, pseudoaneurysm and arteriovenous fistula formation, and even death [3,4]. The complication rate varies among institutions and with the experience of individuals performing the catheterization. According to a study insertion of a catheter by a practitioner who has placed 50 or more central lines is 50% less likely to cause a mechanical complication than an insertion by a practitioner who has not done so [5]. Some of the complications are technique related. Excessive rotation or extension of the head may increase the likelihood of arterial puncture by altering cervical vascular anatomy [6]. Even with correct positioning of the patient and needle at the insertion site [7] complications may occur. Anatomicaly IJV is joined by subclavian vein at middle one third of clavicle to form innominate vein. The subclavian artery lies above and posterior to the vein. Second part of subclavian artery, representing the highest part of the arch of the artery make it more susceptible to cannulation, as in our case [Table/Fig-6,7].
In CT thorax(longitudinal axis) point of entry of catheter into subclavian artery is seen as defect
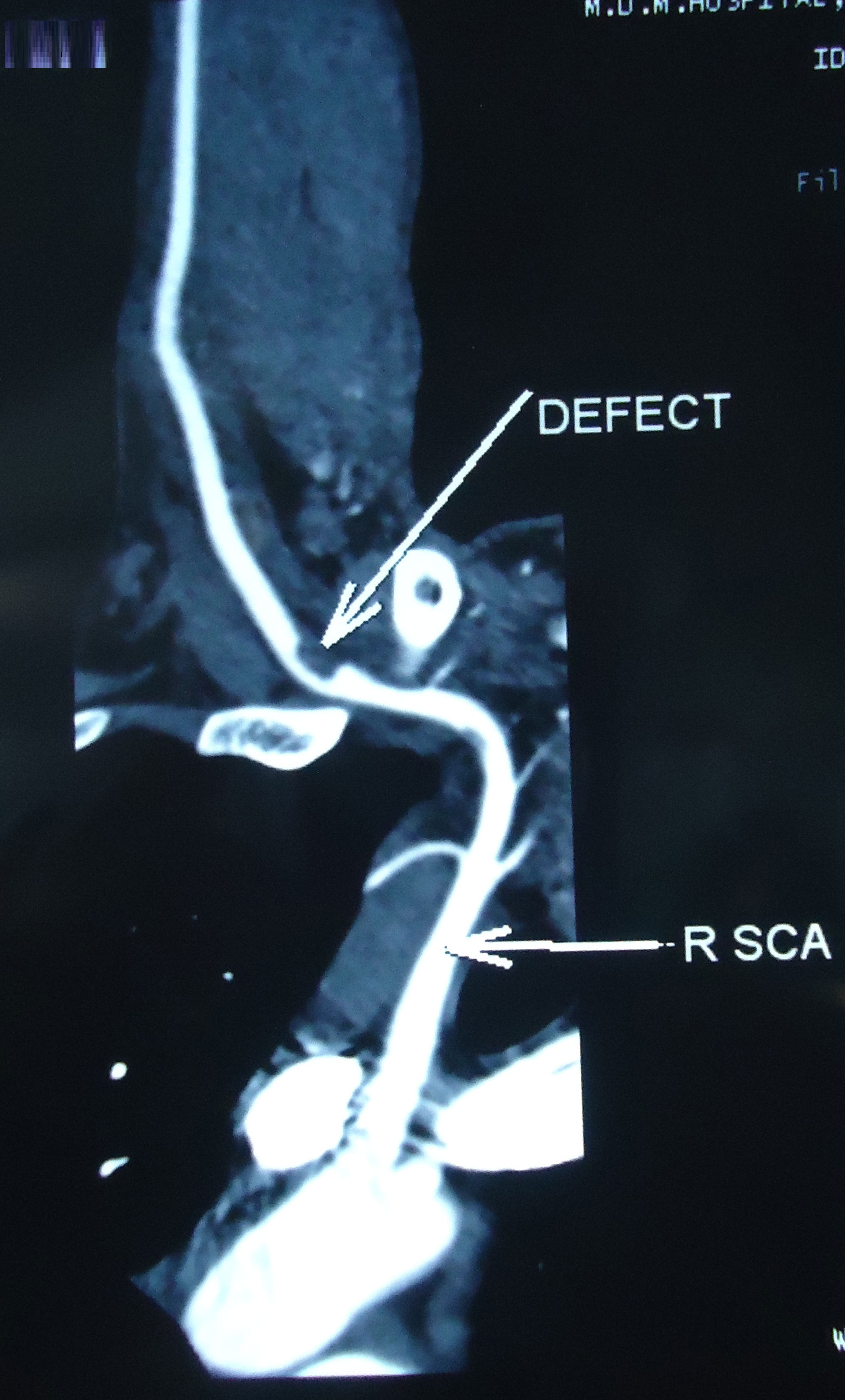
In CT thorax(saggital axis) point of entry of catheter into subclavian artery is seen as defect

Since dark, non-pulsatile blood was aspirated on the first attempt, we opine that the finder needle was initially placed in the IJV but the introducer needle had been erroneously advanced into the subclavian artery prior to guidewire insertion. Since patient was to be given heparin during the surgical procedure (cardiopulmonary bypass pump utilization) expecting uncontrolled bleeding the catheter was left in situ. Also since CVP monitoring was essential and vasopressors and vasodilators need to be infused another attempt was taken to secure right IJV.
Accidental artery cannulation is usually identified immediately by color and pulsatile or high-pressure backflow jet of the blood. However, looking for dark non-pulsatile venous blood for differentiation from bright red pulsatile back flow of arterial blood may not hold true in patients who are hypovolemic, hypotensive or with reduced oxygen content of blood [8]. Colour differentiation also becomes unreliable in case of high mixed venous oxygen saturations due to left-to-right shunts which reduce the arterio-venous gradient [9]. Similarly decreased cerebral oxygen consumption in anaesthetised and hypothermic patients could make colour comparison less sensitive [10]. Accidental cannulation of the artery is easily recognised clinically by difficulty in administering IV fluids. Other methods for confirming artery puncture [1,5,8] include comparison of PaO2 of the blood sample from the suspected catheter with an arterial sample, transduction of the catheter and looking for characteristic arterial waveform, colour doppler, transesophageal echocardiogram, and chest X-ray. As the right subclavian artery originates from the brachiocephalic artery, a catheter inserted in the right subclavian artery will lie above the clavicle [3] in chest X-ray [Table/Fig-3].
Identification of misplaced central lines, searching for reason for error and taking preventive measures to avoid future occurrence are necessary for safe anesthesia practice. Bedside ultrasound enables visualization of the target vein and the adjacent arterial structures, and hence increases success and decreases procedural complications during central venous cannulations. Ultrasound visualization to confirm venous placement of the guide wire prior to dilation [11,12] and insertion of the catheter may help prevent this complication. Non availability of doppler ultrasound or lack of technical expertise in using it is limiting factors for anaesthesiologist for confirmation of proper catheter placement.
Conclusion
This case report emphasis on three important issues. First it highlights the probable event that lead to misinterpretation of the vessel accessed and discussed situations where similar situation may arise. Secondly, it also provide measures to confirm or refute the probability of arterial cannulation at the time of cannulation and thus favouring early intervention before some serious consequences occur. Finally, although confirmation of catheter misplacement can be through chest X-ray further investigations are warranted to confirm catheter location prior to decision for its removal. Consequently backup preparation should be done for subsequent management in case emergency situation, such as uncontrollable hemorrhage, arises from catheter removal. Blood and blood products must also be readily available as need for their transfusion can arise.
[1]. Shah PM, Babu SC, Goyal A, Mateo RB, Madden RE, Arterial misplacement of large-caliber cannulas during jugular vein catheterization: case for surgical managementJ Am Coll Surg 2004 198(6):939-44. [Google Scholar]
[2]. Fyntanidou B, Vasiliadou G, Papachristodoulou A, Pantazopoulou A, Megalopoulos A, Trellopoulos G, Endovascular repair of inadvertent subclavian artery injury during attempted internal jugular vein catheterization: A case reportThe Internet Journal of Endovascular Medicine. [Internet] 2008 Volume 1(Number 2)[Cited 2014 Nov 4]. Available from https://ispub.com/IJEVM/1/2/8278 [Google Scholar]
[3]. Guilbert MC, Elkouri S, Bracco D, Arterial trauma during central venous catheter insertion: case series, review and proposed algorithmJ Vasc Surg 2008 48(4):918-25. [Google Scholar]
[4]. Domino KB, Bowdle TA, Posner KL, Spitellie PH, Lee LA, Cheney FW, Injuries and liability related to central vascular catheters: a closed claims analysisAnesthesiology 2004 100(6):1411-18. [Google Scholar]
[5]. McGee DC, Gould MK, Preventing complications of central venous catheterizationN Engl J Med 2003 348(12):1123-33. [Google Scholar]
[6]. Sulek CA, Gravenstein N, Blackshear RH, Weiss L, Head rotation during internal jugular vein cannulation and the risk of carotid artery punctureAnesth Analg 1996 82(1):125-28. [Google Scholar]
[7]. Bailey PL, Whitaker EE, Palmer LS, Glance LG, The accuracy of the central landmark used for central venous catheterization of the internal jugular veinAnesth Analg 2006 102(5):1327-32. [Google Scholar]
[8]. Ezaru CS, Mangione MP, Oravitz TM, Ibinson JW, Bjerke RJ, Eliminating arterial injury during central venous catheterization using manometryAnesth Analg 2009 109(1):130-34. [Google Scholar]
[9]. Williamson K IP, Latto Internal jugular vein cannulation confused with carotid artery cannulationAnaesthesia 1999 54(4):399-400. [Google Scholar]
[10]. Neustein SM, Narang J, Bronheim D, Use of the color test for safer internal jugular vein cannulationAnesthesiology 1992 76:1062 [Google Scholar]
[11]. Stone M, Ultrasound detection of guidewire position during central venous catheterizationAM J Emerg Med 2009 27(4):516 [Google Scholar]
[12]. Howes B, Dell R, Ultrasound to detect incorrect guidewire positioning during subclavian line insertionAnaesthesia 2006 61:615 [Google Scholar]