Effect of Unintentional Periapical Extrusion of Metapex in Immature Teeth- A Case Report
Virat Galhotra1, Anshu Singla2, Sanjeev Jindal3, Anjali Sofat4
1Professor, Department of Pedodontics and Preventive Dentistry,Gian Sagar Dental College & Hospital, Village Ramnagar, Banur, Rajpura, District Patiala, Punjab, India.
2Reader, Department of Pedodontics and Preventive Dentistry,Gian Sagar Dental College & Hospital, Village Ramnagar, Banur, Rajpura, District Patiala, Punjab, India.
3Reader, Department of Oral Medicine & Radiology,Gian Sagar Dental College & Hospital, Village Ramnagar, Banur, Rajpura, District Patiala, Punjab, India.
4Reader, Department of Prosthodontics,Gian Sagar Dental College & Hospital, Village Ramnagar, Banur, Rajpura, District Patiala, Punjab, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Virat Galhotra, House No 600, Sector-7, Panchkula-134109, India.
E-mail: docvirat@gmail.com
The paper discusses a case of an immature premolar tooth with a large periapical lesion, in which Metapex (calcium hydroxide paste containing iodoform and barium sulphate as a radiopacifier) was used. There was an un-intentional extrusion of calcium hydroxide during application. The patient was evaluated for periapical healing at 12 and 24 months. The follow up revealed that the accidental extrusion of metapex did not have any detrimental effect on periapical healing. However, delayed resorption of Metapex as well as healing of the periapical lesion may be attributed to the presence of BaSO4 and iodoform as compared to plain Calcium hydroxide.
Apexification, Barium sulphate, Periapical Lesion
Case Report
A 14-year-old boy was referred to the Department of Pedodontics and Preventive dentistry with complain of pain in right mandibular posterior teeth since three weeks. Careful intraoral examination revealed a sinus tract found on the buccal gingiva of the right lower second premolar. Hard tissue examination revealed the presence of a deep pit in right mandibular second premolar. Radiographic examination revealed deep pit communicating with the pulp space, presence of blunderbuss canal and the presence of large irregular radiolucency suggestive of chronic abscess with bone resorption associated with mandibular right premolar teeth [Table/Fig-1]. The presence of sinus tract with periapical radiolucency indicative of chronic periapical abscess confirmed the necrosis of pulp. Nonsurgical endodontic treatment with apexification was considered keeping in view the age and amount of trauma expected during surgical treatment. Pulpal necrosis confirmed the non vitality of the tooth. Hence, the need of giving local anesthesia was excluded. The informed written consent was taken from the parents. Access opening was done under rubber dam isolation. Due to exudation of pus from the canal, the access cavity was left open. In next appointment the biomechanical preparation was done using circumferential filling till size 80K file. Sodium hypochlorite 1% solution was used as root canal irrigant throughout the procedure. In the same sitting calcium hydroxide and iodoform combination (Metapexô, META Biomed Co. Ltd., Korea) was placed in the canal which was accidentally extruded into the periapical lesion [Table/Fig-2]. The patient was then recalled after two weeks. The healing of sinus and history of no pain was evident in the recall appointment
Patient was followed for 3, 6 & 12 months. During these appointments, the follow up radiograph revealed, metapex that had extruded in the periradicular region has not resorbed; in addition, the periapical lesion was seen to have decreased in size [Table/Fig-3]. At the end of 12 months apical barrier was formed. A file was used that can easily reach the apex to gently probe for a stop at the apex. At that time, the medicament was removed from the canal using H-file followed by irrigation with 1.25% sodium hypochlorite. After confirming dryness of canal, the root canal was finally obturated after 12 months with Gutta-percha by using the cold lateral condensation technique. After root canal treatment, the patient was seen again after 6 & 12 months. At 2-year recall, the patient was completely asymptomatic and intraoral periapical radiograph of the same tooth revealed complete resolution of the lesion but not the metapex [Table/Fig-4] but this extruded metapex doesn't cause any complication.
Discussion
A large number of different apical configurations can result if an immature tooth with an open apex is traumatized. Continued root development, apical doming, in-growth of bone and aberrant root formation have all been reported. Repair appears to be more related to the creation of an environment conducive to repair rather than type of medicament used [1].
Apexification is the treatment of choice after confirmation of pulpal necrosis in immature permanent teeth. Although a variety of materials have been proposed for induction of apical barrier formation, which include calcium hydroxide paste, calcium hydroxide powder mixed with different vehicles, tricalcium phosphate, collagen calcium phosphate, osteogenic protein-1, bone growth factor, oxidized cellulose, Mineral trioxide aggregate etc [2]. Calcium hydroxide has gained the widest acceptance, since its introduction by Hermann [3,4]. The therapeutic effect of calcium hydroxide is due to its ability to break down into calcium and hydroxyl ions. Hydroxyl ions show an affinity to various biologically active substances [5]. Hydroxyl ion forms a potent alkaline medium which causes the destruction of lipids which inturn leads to structural damage of bacterial proteins and nucleic acids [6]. Calcium hydroxide, is capable of activating tissue enzymes which favour tissue restoration through mineralization [7]. The calcium hydroxide activates alkaline phosphatase by its high pH [8,9]. Once this hydrolytic enzyme is activated it releases inorganic phosphate from the esters of phosphate which is responsible for the process of mineralization [10].
These phosphate ions further react with calcium ions from the blood stream to form calcium phosphate which is the molecular unit of hydroxyapatite [11]. The physio-chemical state of intercellular substance is altered by direct contact with Calcium hydroxide [8]. It has been observed that formation of mineralized tissue occurs after 7-10 d contact with calcium hydroxide [8,9]. To improve the properties like radiopacity, flow, and consistency of calcium hydroxide various substances have been added as in Metapex. The oily vehicles present in Metapex are responsible for the lowest solubility and diffusion of the paste within the tissues [11]. Iodoform is incorporated to improve the antibacterial properties of the material and BaSO4 as radiopaque agent in Ca(OH)2 pastes.
In this case report, the effect of accidental and voluminous Metapex Beyond apex into periradicular lesion and tissue on the prognosis of periapical healing in the mandibular premolar teeth with periapical lesion was evaluated. The presented case report showed that when Metapex was applied as an intracanal dressing and extruded through the periapical lesion associated with pulpless teeth, there was no detrimental effect; throughout the period after the metapex was extruded, the teeth were continuously free of symptoms. But complete resorption of the paste did not occur, although the periradicular radiolucency disappeared. The presence of BaSO4 and iodoform in the paste may be responsible for the incomplete resorption of paste. It was found that BaSO4 can obscure the apex and is not readily resorbed over time when extruded beyond the apex which in turn may prolong the healing property of the paste [12]. In addition, BaSO4 demonstrates a residual radiopacity. Webber et al., observed that residual radiopacity at the root apex is reduced by making ratio of BaSO4:Ca(OH)2 to 1:8 [13]. However, after 21 months the remnants of the paste were still obscuring the apex of a treated tooth in one case which makes radiographic interpretation of osseous healing more difficult. As 100 ml of water can dissolve only 0.02 g of BaSO4 it has been proposed to use resorbable iodine compounds like diatrizoate or iothalamate instead of BaSO4 due to the fact that these do not have a significant effect on the length of the healing period [12]. In a study conducted on the effect of accidental and voluminous Ca(OH)2 overextrusion into periradicular lesions and tissues on the prognosis of periapical healing by De Moor and De Witte [14] reported that in cases of extensive Ca(OH)2 overextrusion, repair took more than six months and observed that complete resorption of the paste including BaSO4 did not occur, eventhough the periradicular radiolucency disappeared. The time taken for periradicular radiolucency to disappear was approximately 24 months in the presented case which is in line with the findings of other researchers. The mechanical properties of the bone cement were negatively influenced by BaSO4 as reported in various studies related to orthopedic surgery. It was found that BaSO4 particles results in a decrease of the tensile strength when compared with the use of radiolucent cement in research conducted by Ginebra et al., [15]. As the water affinity of BaSO4 and Ca(OH)2 powders in different concentrations differed, so the amount of water to make the ideal paste would also be different [16]. Therefore, the present case highlights the longer healing period which might be due to the consistency of paste, the amount of extruded paste and the dimension of the lesion as well.
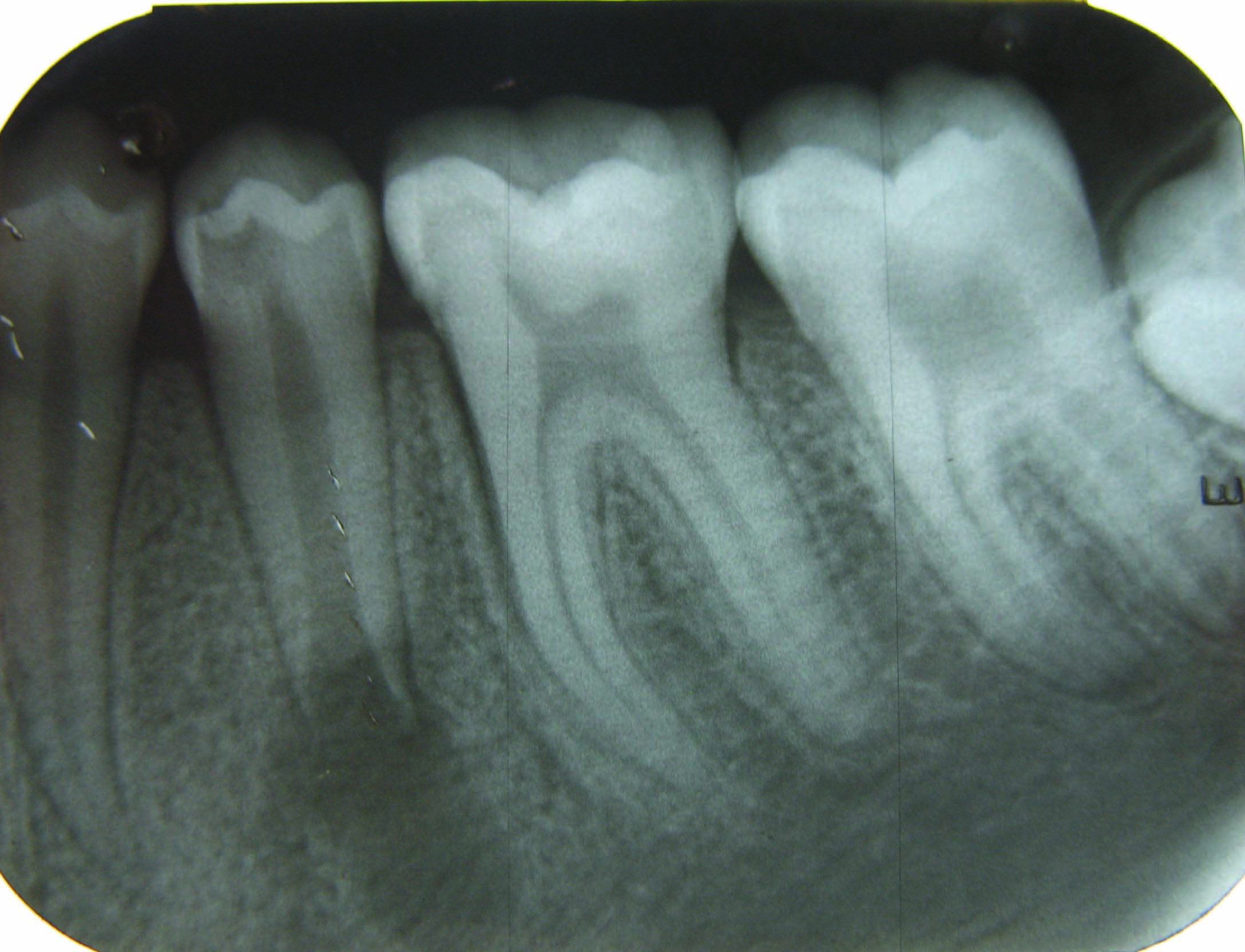
Radiograph of the Right mandibular premolar teeth with periapical radiolucency
Radiograph after placement of metapex with unintentional periapical overextrusion

Follow up radiograph after 1 year showing resorption of metapex

The 24-month radiograph showing healing of the periapical lesion and the presence of extruded metapex

Conclusion
The BaSO4 and iodoform has unknown effects on the healing process hence intentional overextrusion is not indicated even though patient reports with no symptoms. The long term success of the treatment with BaSO4 needs to be evaluated. So it is recommended that further clinical trials should be conducted on long term basis.
[1]. AJ Moule, CA Moule, The endodontic management of traumatized permanent anterior teeth: a reviewAust Dent J 2007 52(1 Suppl):S122-37. [Google Scholar]
[2]. A de Jesus Soares, J Yuri Nagata , RC Casarin, J Flávio Affonso de Almeida, BP Gomes, A Augusto Zaia , Apexification with a New Intra-Canal Medicament: A Multidisciplinary Case ReportIran Endod J 2012 7(3):165-70. [Google Scholar]
[3]. A Bystrom, G Sundqvist, The antibacterial action of sodium hypochlorite and EDTA in 60 cases of endodontic therapyInt Endod Jr 1985 18(1):35-40. [Google Scholar]
[4]. DS Sharma, SP Chauhan, VK Kulkarni, C Bhusari, R Verma, Accidental periapical extrusion of non-setting calcium hydroxide:Unusual bone response and managementJ Indian Soc Pedod Prev Dent 2014 32(1):63-67. [Google Scholar]
[5]. JF Siqueira, HP Lopes, Mechanisms of antimicrobial activity of calcium hydroxide: A critical reviewInt Endod J 1999 32(5):361-69. [Google Scholar]
[6]. SD Tamburi, GM Vuleta, JM Ognjanovi, In vitro release of calcium and hydroxyl ions from two types of calcium hydroxide preparationsInt Endod J 1993 26(2):125-30. [Google Scholar]
[7]. C Estrela, GB Sydney, LL Bammann, O Felippe Júnior, Mechanism of action of calcium and hydroxyl ions of calcium hydroxide on tissue and bacteriaBraz Dent J 1995 6(2):85-90. [Google Scholar]
[8]. WH Binnie, DF Mitchell, Induced calcification in the subdermal tissues of the ratJ Dent Res 1973 52(5):1087-91. [Google Scholar]
[9]. L Tronstad, JO Andreasen, G Hasselgren, L Kristerson, I Riis, pH changes in dental tissues after root canal filling with calcium hydroxideJ Endod 1981 7(1):17-21. [Google Scholar]
[10]. G Granstrom, A Linde, A biochemical study of alkaline phosphatase in isolated rat incisor odontoblastArch Oral Biol 1972 17(8):1213-24. [Google Scholar]
[11]. N Sridhar, S Tandon, Continued root-end growth and apexification using a calcium hydroxide and iodoform paste (Metapex®): three case reportsJ Contemp Dent Pract 2010 11(5):63-70. [Google Scholar]
[12]. T Alaçam, G Görgül, H Omürlü, Evaluation of diagnostic radiopaque contrast materials used with calcium hydroxideJ Endod 1990 16(8):365ñ8 [Google Scholar]
[13]. RT Webber, KA Schwiebert, GM Cathey, A technique for placement of calcium hydroxide in the root canal systemJ Am Dent Assoc 1981 103(8):417ñ21 [Google Scholar]
[14]. RJ De Moor, AM De Witte, Periapical lesions accidentally filled with calcium hydroxideInt Endod J 2002 35(11):946-ñ58. [Google Scholar]
[15]. MP Ginebra, L Albuixech, E Fernandez-Barragan, Mechanical performance of acrylic bone cements containing different radiopacifying agentsBiomaterials 2002 23:1873-82. [Google Scholar]
[16]. AA Vernieks, LB Messer, Calcium hydroxide induced healing of periapical lesions: a study of 78 non-vital teethJ Br Endod Soc 1978 11:61-69. [Google Scholar]