Pancreatic Heterotopia of Small Intestine with Tubercular Ileitis
Dinesh Kumar1, Romi Srivastava2, Jay Prakash3, Kachnar Varma4, Vatsala Misra5
1 Junior Resident, Department of Pathology, Moti Lal Nehru Medical College, Allahabad, Uttar Pradesh, India.
2 Junior Resident, Department of Pathology, Moti Lal Nehru Medical College, Allahabad, Uttar Pradesh, India.
3 Junior Resident, Department of Pathology, Moti Lal Nehru Medical College, Allahabad, Uttar Pradesh, India.
4 Associate Professor, Department of Pathology, Moti Lal Nehru Medical College, Allahabad, Uttar Pradesh, India.
5 Professor and Head, Department of Pathology, Moti Lal Nehru Medical College, Allahabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dinesh Kumar, House no. 1535 Sector-3 Huda, Rohtak-124001, Haryana, India. Phone : 09559546553, E-mai : dinodoc21@gmmail.com
Pancreatic heterotopia is defined as pancreatic tissue outside the boundary of pancreas that lacks an anatomic and vascular connection to it. Till today, no case of pancreatic heterotopia along with tubercular ileitis has been reported. We report one such case that presented in our institution.
Appendicitis, Laparotomy, Small Intestine
Case Report
A 25-year-old male presented with clinical features of acute intestinal obstruction. An exploratory laparotomy with ileal resection and appendicectomy was carried out. A segment of small intestine measuring 19 x 3 cm and whole appendix was received for histopathological examination. On gross examination, intestine showed an area of stricture. On opening the mucosal surface in strictured area was flattened and ulcerated with numerous small coalescing ulcers and shaggy floor [Table/Fig-1a]. Multiple small well defined nodules were seen 5 cm away from the stricture. The largest one was measuring 0.8x0.8 cm in size [Table/Fig-1b]. Cut section of the nodule was yellowish white. Appendix was 3 x 1 cm in size and lumen was patent on opening.
Gross specimen showing a stricture

Grossly visible nodular area with overlying normal appearing mucosa

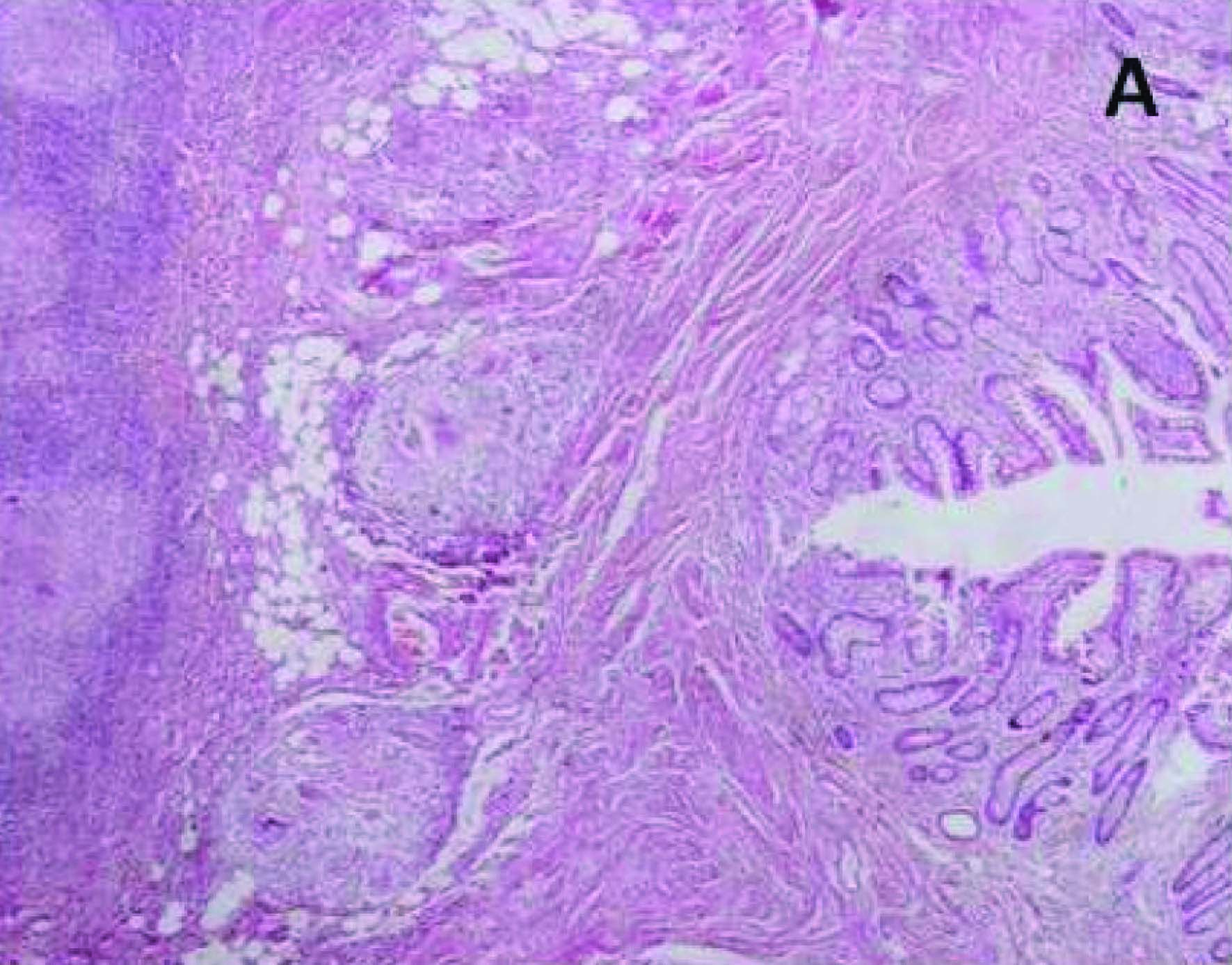
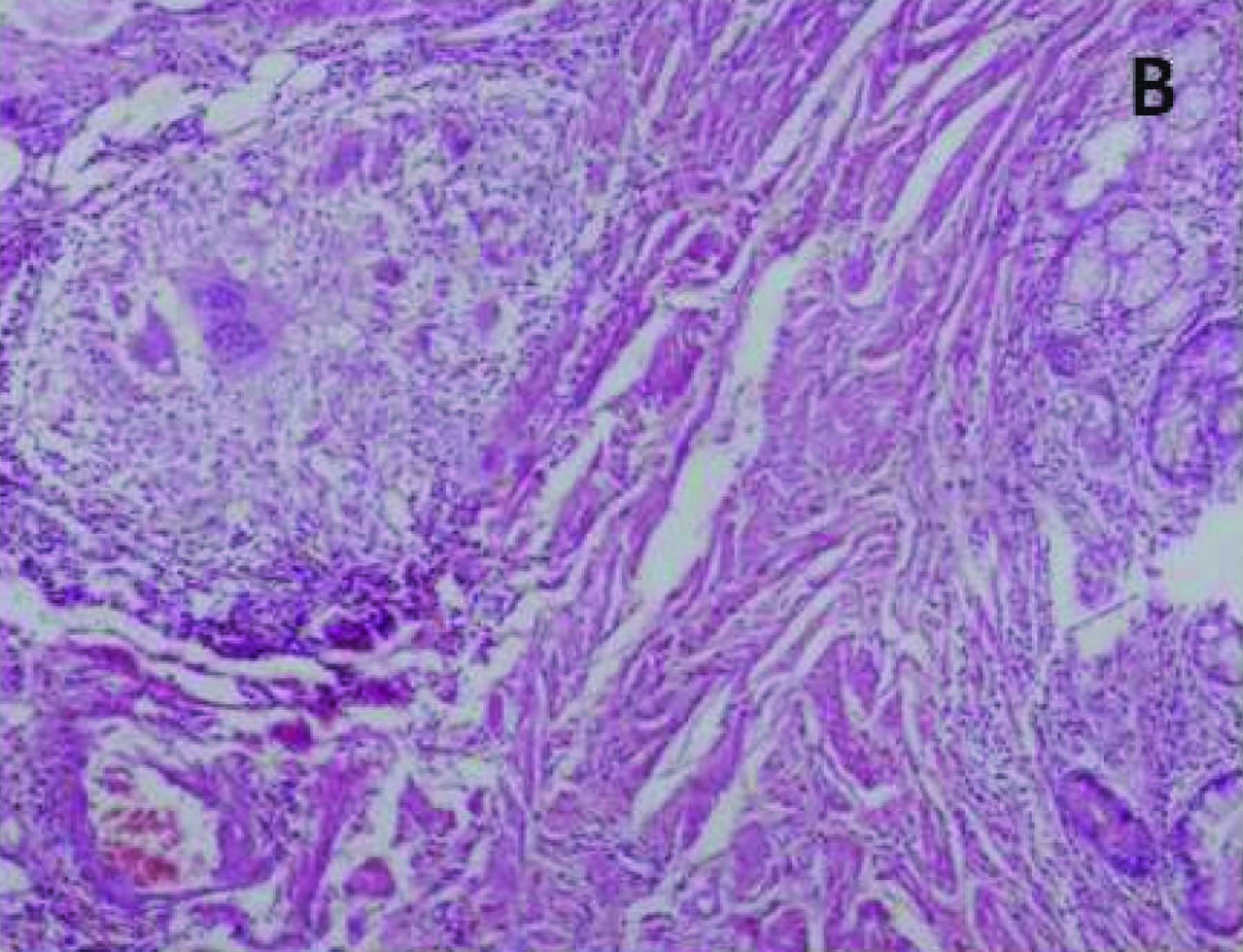
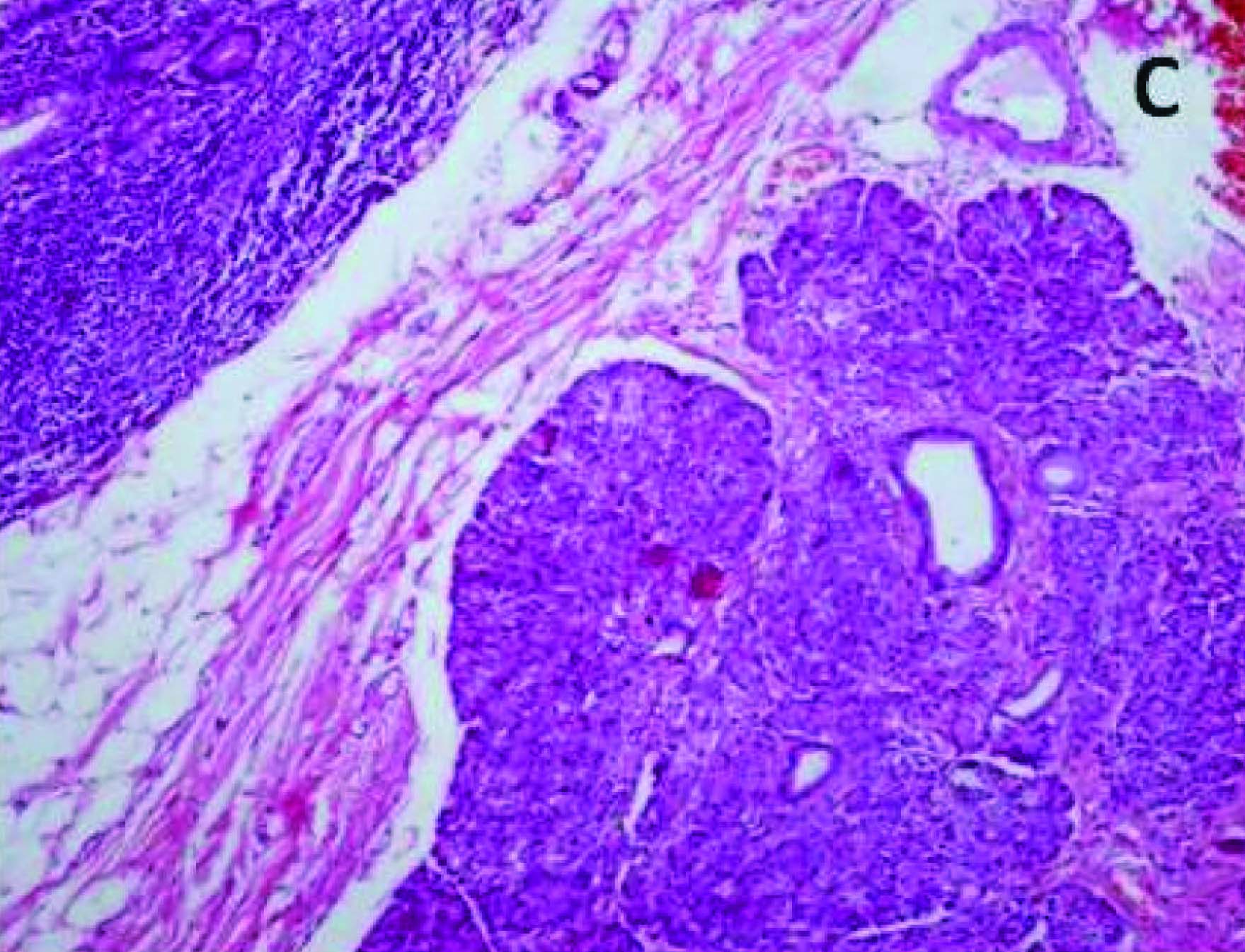
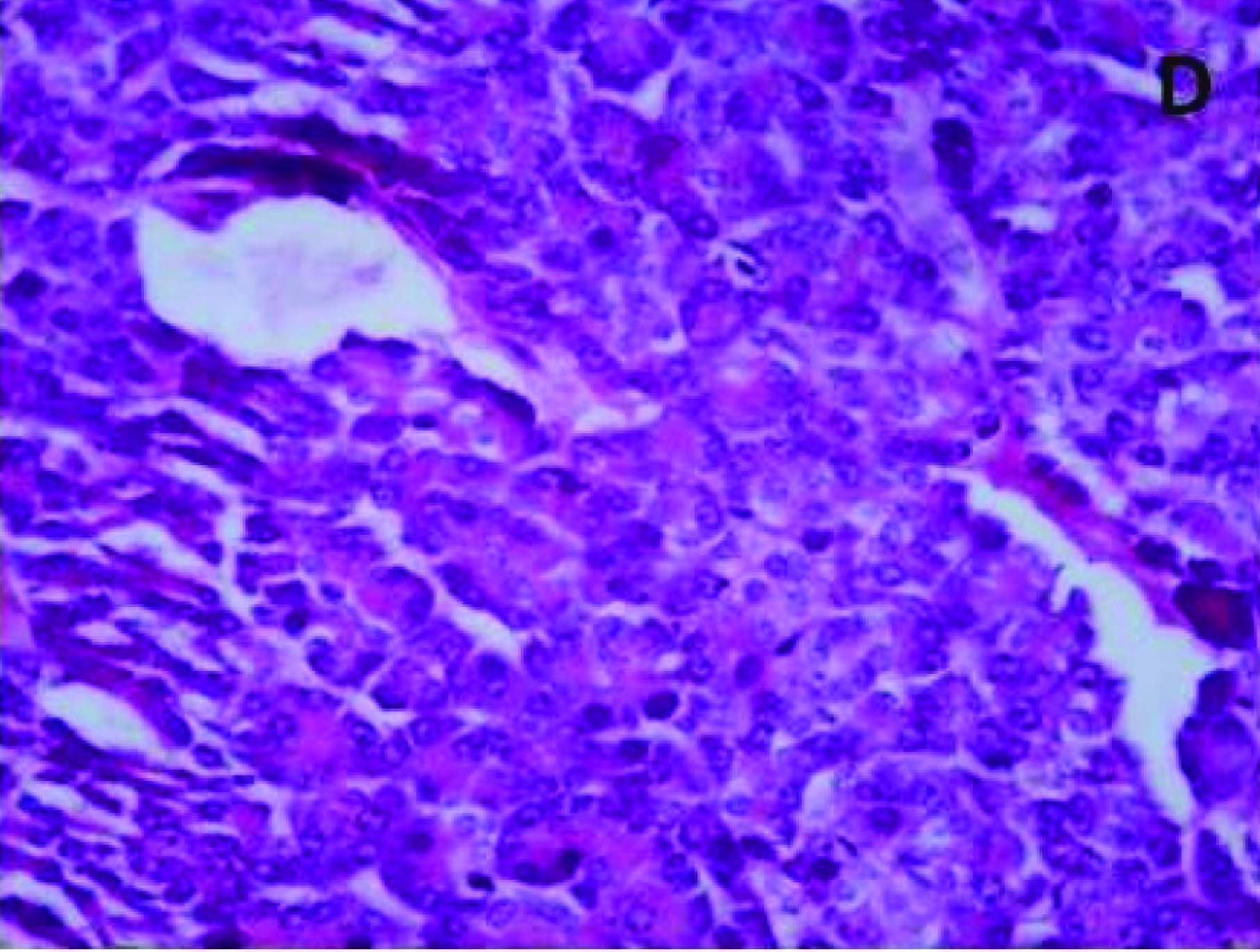
On histopathology, sections from areas of stricture showed small intestinal mucosa with partially flattened villi and focal areas of surface ulcerations. Numerous granulomas composed of langhans’ type giant cells and epithelioid cells along with perilymphocytic cuffing were seen transmurally. Hyperplastic lymphoid follicles were seen in adjacent areas [Table/Fig-2a,b]. Sections from nodular areas showed normal small intestinal mucosa. Submucosa showed foci of normal pancreatic acini along with ducts (Type 1 heterotopic pancreas).Pancreatic tissue showed both acinar cells and islets cells [Table/Fig-2c,d]. Sections from appendix showed features of acute appendicitis.
Section from intestine showing epithelioid cell granulomas in submucosa (H&E x40)
Higher magnification showing epithelioid cell granuloma (H&E X100)
Section from nodular area showing normal intestinal mucosa and pancreatic tissue (H&E X100)
Higher magnification showing pancreatic acini (H&E X 400)
Discussion
This case presented with intestinal obstruction due to tubercular ileitis. Finding of pancreatic heterotopia was incidental. In earlier studies also pancreatic heterotopia was mostly asymptomatic and discovered incidentally [1,2]. Although, it can occur throughout the entire gastrointestinal tract, it is most commonly found in the stomach (25%-38%), duodenum (17%-36%), and jejunum (15%-21%) [3]. Other rare sites reported are oesophagus, biliary tract, gallbladder, spleen, and mesentery. Usually it is seen as an isolated lesion and co-occurrence with other inflammatory and neoplastic lesion is rare [3].
Two theories have been put forward to explain the origin of pancreatic heterotopia. In embryo the pancreas develops from invaginations of endodermal tissue in the primitive duodenum. The head of the pancreas is formed by ventral aspect and dorsal aspect forms the body and tail [4]. According to misplacement theory, during rotation of the foregut, several elements of the primitive pancreas become separated and eventually form mature pancreatic tissue along the length of the gastrointestinal tract [3]. The second theory that is the metaplasia theory states that pancreatic heterotopia arises from areas of pancreatic metaplasia of the endoderm which migrate to the submucosa during embryogenesis [4].
An extensive search of literature failed to document any case with a dual histomorphological feature of pancreatic heterotopia with tubercular ileitis.
Whether there exists any causal relation between tubercular ileitis and pancreatic heterotopia deserves further probe. It is to be noted that pancreatic tuberculosis is itself a rare disease and thus it may not be implausible to assume that a pancreatic heterotopia in ileum may create a milieu unsuitable for growth of tubercular disease. The obvious hurdle to further study of this hypothesis is the overwhelming rarity of co-existence of pancreatic heterotopia with tubercular ileitis. It is equally possible that there may be cases of tubercular ileitis with pancreatic heterotopia where diagnosis of pancreatic heterotopic was missed/masked due to more attention towards tubercular lesion thereby causing a reduction in the documentation of such cases.
Majority of nodules presenting in ileum, especially those that are yellowish-white on cut section, are assumed to be carcinoid tumours. Other commonly considered diagnosis may be mesenchymal lesions like GIST or primary adeno carcinoma.
Conclusion
The case was considered worth documentation due to rare coexistence of tuberculosis along with pancreatic heterotopia and to make the young pathologists aware of presence of heterotopia at an uncommon site.
[1]. Tanaka K, Tsunoda T, Eto T, Yamada M, Tajima Y, Shimogama H, Diagnosis and management of heterotopic pancreasInt Surg 1993 78:32-35. [Google Scholar]
[2]. Eisenberger CF, Gocht A, Knoefel WT, Busch CB, Peiper M, Kutup A, Heterotopic pancreas--clinical presentation and pathology with review of the literatureHepatogastroenterology 2004 51:854-58. [Google Scholar]
[3]. Ormarsson OT, Gudmundsdottir I, Marvik R, Diagnosis and treatment of gastric heterotopic pancreasWorld J Surg 2006 30:1682-89. [Google Scholar]
[4]. Gupta MK, Karlitz JJ, Raines DL, Florman SS, Lopez FA, Heterotopic Pancreas. Journal of the Louisiana State Medical SocietyJ La State Med Soc 2010 162:310-13. [Google Scholar]