Incidental Intravascular Lipoleiomyomatosis in A Hysterectomy Specimen: How To Manage?
Zehra Nihal Dolgun1, Rakhshanda Aslanova2, Nuray Can3, Sabri Berkem Okten4, Mehmet Musa Aslan5
1 Assistant Professor, Department of Obstetrics and Gynecology, Trakya University Medicine Faculty, Edirne, Turkey.
2 Resident, Design Department of Obstetrics and Gynecology, Trakya University Medicine Faculty, Turkey.
3 Assistant Professor, Department of Pathology, Trakya University Medicine Faculty, Turkey.
4 Resident, Department of Obstetrics and Gynecology, Trakya University Medicine Faculty, Turkey.
5 Resident, Writing, Department of Obstetrics and Gynecology, Trakya University Medicine Faculty, Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Zehra Nihal Dolgun, Assistant Professor, Department of Obstetrics and Gynecology, Trakya University Balkan Campus, 22000, Level 3, Edirne, Turkey. E-mai : dr_nihaldolgun@hotmail.com
Leiomyomas are common benign tumors in female gynaecologic surgery. They are originated from smooth muscle cells of the uterus and/or sometimes of the uterine vessels. Intravascular lipoleiomyomatosis is a very rare form of leiomyomas which grow within veins and can extend up to vena cava inferior and right heart chamber with cardiac symptoms and is diagnosed by cardiovascular surgeons. We report a case of incidental intravascular lipoleiomyomatosis which was confined to the uterus being diagnosed after a total abdominal hysterectomy by pathology and its management strategy.
Follow-up, Hysterectomy, Intravascular lipoleiomyomatosis
Case Report
A 49-year-old woman presented to our gynecology clinic with pelvic pain, abnormal uterine bleeding, discomfort and anemia with a hemoglobin level of 9.4 gr/dl. The gynaecologic examination revealed uterine bleeding with normal morphology cervix and external genitalia. She had a mild enlarged uterus with non-specific adnexal examination. Ultrasound imaging showed nothing more than a 2cm intramural myoma. She had a normal cervical smear cytology which was done 2 months ago. An endometrial sampling was performed and result was simple endometrial hyperplasia without atypia. Since she had two other endometrial samplings in the past year because of abnormal bleeding, she desired an operation. A total abdominal hysterectomy and bilateral salpingo-ooferectomy was performed to the patient without any complications.
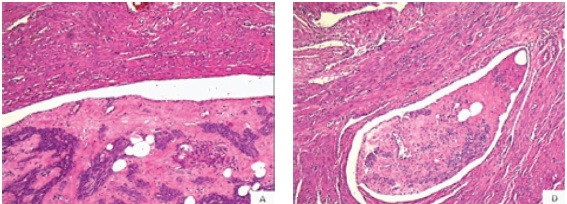
The gross-examination of the specimen revealed a 2.5 cm sized nodule with a whorled cut-surface located in myometrium and also protruded through the endometrial surface with a polypoid process. Histologically, tumor nodules were composed of trabeculae of spindle cells and lobules of adipocyts seen in vascular spaces. The spindle cell component of the tumor had no cytological atypia or necrosis and the mitotic activity was low [Table/Fig-1a,b].
Tumor nodules composed of trabecules of spinddle cells and lobules of adipocyts in vasculary spaces were seen (1a-b; H&E X 50)
Immunohistochemical studies revealed SMA, Caldesmon and Desmin positivity in the spindle cell component and CD 34 study revealed the intravascular distribution of the tumor. No reaction was seen by CD 10 immunohistochemistry [Table/Fig-2a–e]. The pathologic diagnosis was intravascular lipoleiomyomatosis.
Tumor exhibitied positive reaction with SMA
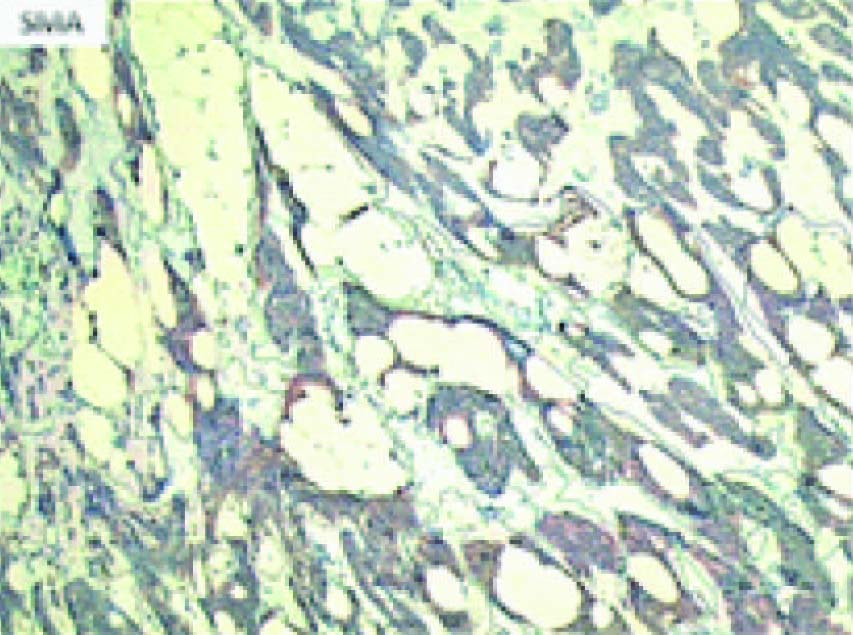
immunoperoxidaseX50), Caldesmon (2b; immunoperoxidaseX50), and Desmin(2c; immunoperoxidaseX50), and there was no reaction with CD10 (2d;. Immunohistochemical study with CD 34 revealed the intravasculary distrubution of the tumor (2e; immunoperoxidaseX50)

Discussion
Intravenous leiomyomatosis (IVL) is a lesion of uterus which is capable of local and/or distinct intravascular extension. Lipoleiomyoma (LPL) is also a benign tumor of the uterus consisting of smooth muscle and fat [1]. They are both rare lesions and their combination is extremely rare [2]. IVL is a smooth-muscle neoplasm originating from a uterine leiomyoma and is characterized by a growth within the uterine or pelvic veins [3–5]. IVL may present itself as a leiomyoma with symptoms of pelvic pain and vaginal bleeding or with different system symptoms such as cough and dyspnea in lung metastasis. It can also present with cardiac failure due to tumor extension in right heart chamber [6].
IVL not always but sometimes behave like a malignant tumor and benign metastatic leiomyomatosis often occur in the lungs [3,4]. Extrauterine involvement occurs 30%–80% of IVL cases and 10%– 30% cardiac involvement is present depending on the pathologic reports [7]. The tumor has the potential of growth inside the veins of broad ligament, and extend to the inferior vena cava through different vessels (i.e.,iliac veins and ovarian veins), reaching the right heart chambers and occasionally the pulmonary artery, resulting in death [8]. Our case was an example of intravascular lipoleiomyomatosis which was luckily confined to the uterus and might be prevented from such catastrophic results by proper and close follow-up.
CT and MRI are the most useful modalities in the assessment and follow-up of these patients since they are cross-sectional methods, with multiplanar capabilities, demonstrating continuity in intraluminal tumor growth from the pelvic veins [3–5].
Since this disease has a benign nature with a malignant behaviour we presented the case to our instution`s oncology council. The decision was to perform a cranial MRI and thoracical CT in order to evaluate the most blood-taking organs. The first results came clear and the patient was taken to follow-up in every 6 months with cranial CT and abdominal MR which is consistent with the literature. In her postop 12th month she is still desease-free without any complaints.
Conclusion
Intravascular lipoleiomyomatosis is a very rare condition and its behaviour may vary. This rare condition should not be oversight and serious attention must be paid when encountered for patient`s future well-being. Clinical follow-up and vigilance for cardiac symptoms are extremely important.
[1]. Brescia RJ, Intravascular lipoleiomyomatosis: a report of two casesHuman Pathology 1989 20:252-56. [Google Scholar]
[2]. Fasih N, Prasad Shanbhogue AK, Macdonald DB, Leiomyomas beyond the uterus: unusual locations, rare manifestationsRadio- graphics 2008 28(7):1931-48. [Google Scholar]
[3]. Bender LC, Mitsumori LM, Lloyd KA, Stambaugh LE, AIRP best cases in radiologic–pathologic correlation: intravenous leiomyomatosisRadiographics 2011 31(4):1053-58. [Google Scholar]
[4]. Hashuguchi J, Intravascular leiomyomatosis with uterine lipoleiomyomaGynaecologic Oncology 1994 52:94-98. [Google Scholar]
[5]. Peng H-J, Zhao B, Yao Q-W, Qi H-T, Xu Z-D, Liu C, Intravenous leiomyomatosis: CT findingsAbdom Imaging 2012 37(4):628-31. [Google Scholar]
[6]. Burke M, Opeskin K, Death due to intravenous leiomyomatosis extending to the right pulmonary arteryPathology 2004 36:202-03. [Google Scholar]
[7]. Liu B, Liu C, Guan H, Intravenous leiomyomatosis with inferior vena cava and heart extensionJ Vasc Surg 2009 50(4):897-902. [Google Scholar]
[8]. Wu CK, Intravenous leiomyomatosis with intracardiac extensionInternal Medicine 2009 48:997-1001. [Google Scholar]