Metastases of Squamous Cell Carcinoma of Uterine Cervix to Duodenum: A Case Report
Sanjay M. Chawhan1, Aarti A. Dani2, Saroj A. Meshram3, Archana A. Randale4, D.T. Kumbhalkar5
1 Assistant Professor, Department of Pathology, GMC & SSH, Nagpur Maharashtra, India.
2 Associate Professor, Department of Pathology, GMC & SSH, Nagpur Maharashtra, India.
3 Assistant Professor, Department of Pathology, GMC & SSH, Nagpur Maharashtra, India.
4 Assistant Professor, Department of Pathology, GMC & SSH, Nagpur Maharashtra, India.
5 Professor, Department of Pathology, GMC & SSH, Nagpur Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Sanjay M. Chawhan, 59, Bajrang Nagar, Manewada Road, Nagpur-440027, India.
Phone: 09823642628,
E-mail: chawhansanjay30@gmail.com
We report a case of squamous cell carcinoma of uterine cervix metastasizing to the duodenum through lymphatics. Para-aortic group of lymph nodes were involved which ultimately infiltrated the duodenum. On endoscopic examination, peri-ampullary growth was noted. Endoscopic biopsy from the growth was studied by routine histopathology and metastasis of squamous cell carcinoma involving duodenum was reported.
Cervix, Duodenum, Endoscopy, Suamous cell carcinoma
Case Report
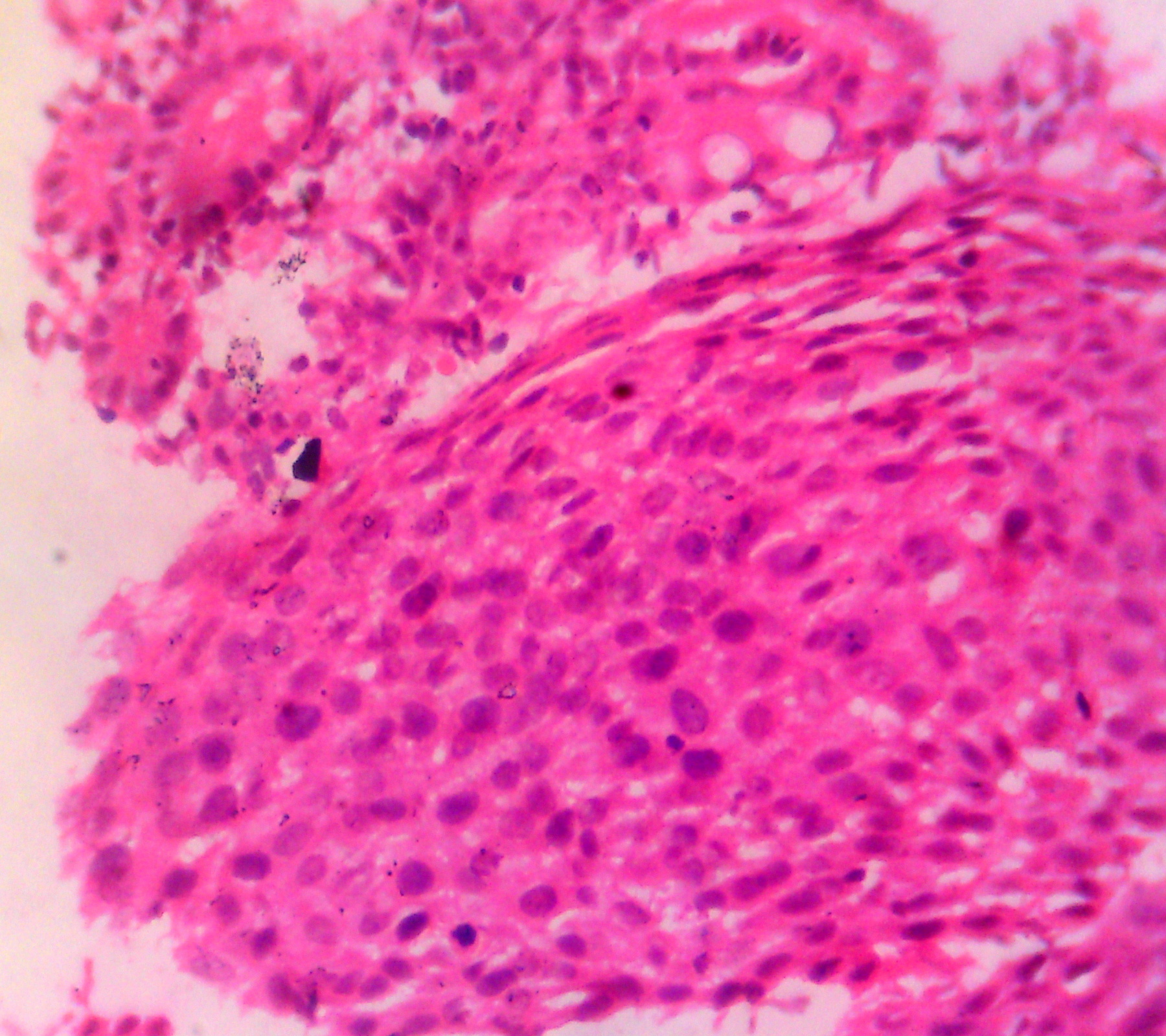
A 52-year-old non smoker female patient presented with the complaints of pain in abdomen associated with heartburn and nausea. She was operated case of hysterectomy for squamous cell carcinoma of uterine cervix. She was given radiotherapy for the same two years back but the time period and dosage of radiation was not available due to loss of records. On examination, she was complaining of loss of weight approximately 10 to 15% of body weight and anorexia since six months. CT abdomen showed heterogeneously enhancing mass in upper retroperitoneum directly involving third part of the duodenum [Table/Fig-1]. Radiological provisional diagnosis was lymph node mass with secondary involvement of duodenum. Upper gastrointestinal endoscopic examination showed multiple nodular areas at periampullary region extending beyond ampulla. Endoscopic biopsy from periampullary region was taken. Multiple tiny grey brown tissue bits were submitted for histopathology examination. Sections were prepared by paraffin embedding method and stained with haematoxylin and eosin. Microscopic examination revealed normal duodenal mucosa with sparse inflammatory infiltrate [Table/Fig-2]. The duodenal wall was infiltrated by squamous islands. It showed malignant squamous cells with pleomorphism and hyperchromasia [Table/Fig-3]. So, the final diagnosis was metastasis of squamous cell carcinoma involving duodenum was done. Further management of patient was not known due to loss of follow up.
CT abdomen showed heterogeneously enhancing mass in upper retroperitoneum directly involving third part of the duodenum

Photomicrograph showing normal mucosa with squamous islands

Photomicrograph showing malignant squamous cells with pleomorphism & hyperchromasia
Discussion
Carcinoma cervix is the most common malignancy in Indian women, with an incidence of 19 to 44 per 100 000 women [1]. It is well known that carcinoma of cervix exhibits a low incidence of distant metastases and more often spreads locally. It is exceedingly rare for squamous cell carcinoma (SCC) of the cervix to clinically present with symptoms related to small bowel metastases. The lymphatic system is the usual route through which cervical cancer spreads to distant regions and there is rarity of the blood vessel invasion. Metastasis to the lymph nodes at the bifurcation of the aorta is invariably accompanied by distant spread [2]. Most of the reported cases of squamous cell carcinoma in the pyloroduodenal region are from lung primary [1].
Although metastatic lesions in the GIT are rare, they do occur. They usually present as single and primary carcinoma-like lesions, with the stomach and duodenum most commonly involved [3]. Metastatic tumours involve the small bowel and present as obstruction or perforation, necessity palliative resection. Metastatic lesions are more common in the duodenum, jejunum and ileum than primary lesions [4]. Common types of primary are melanoma, carcinoma of lung, carcinoma of breast, carcinoma of ovary and choriocarcinoma [5]. Carcinoma of cervix spreads characteristically by direct extension, but lymph node metastasis is also common. First station is represented by paracervical, hypogastric, obturator and external iliac group. The second station includes sacral, common iliac, aortic and inguinal group. Nodal involvement is directly related to the stage of the disease; hence the crucial predictor of prognosis [6]. Extra-pelvic spread of SCC of the cervix to the small bowel is rare with only six reported cases in the English literature since 1981 [4].
Metastases to remote sites from invasive carcinoma of the uterine cervix were reported with varying incidence rates in the literature [7]. Most of these data were based on autopsy investigation. A case series by Marcial-Rojas et al., found the incidence to be 22.4%.The lymphatic system is the usual route through which cervical cancer spreads to distant regions and the rarity of the blood vessel invasion [2,8]. Clinically, the pattern of recurrence of carcinoma of cervix varied with the treatment. Increased central pelvic recurrences were seen after surgery due to inadequate surgical excision, lateral deep pelvic recurrences after combined treatment (Surgery & Radiation) with surgery and radiotherapy due to inadequate radiation doses to parametria and distant metastases after radiation. In this case, patient belongs to the third category. The distant metastases were widespread and the distribution was unaffected by the kind of treatment given for the primary disease [8].
In the radiation group, relatively high incidence of distant metastases may be secondary to a relatively longer survival and better local control of the disease. In the analysis by Badib AO et al., for organ involvement, the radiation group showed an increased risk of extrapelvic metastases without involvement of local pelvic organs. Spread through lymphatic channels with lymph node involvement generally occurs in an orderly manner, first to the primary, then to secondary and then to the extrapelvic lymph nodes, probably through embolus or anomalous circulatory communications. The most common sites of extrapelvic metastases were lungs and liver with greater frequency [8]. Apart from the parametrium and vagina, the urinary tract, uterus and adnexa, uterosacral ligaments, and abdominal and pelvic viscera were found to be involved with an increasing incidence rate as the clinical stage increases [8].
Conclusion
Carcinoma of cervix spreads characteristically by direct extension, but lymph node metastasis is also common. Metastasis to the lymph nodes at the bifurcation of the aorta is invariably accompanied by distant spread. The most common sites of extra pelvic metastases were lungs and liver. Extra pelvic spread of squamous cell carcinoma of the cervix to the small bowel is rare. Awareness of such infrequent patterns of metastases in cervical cancer is important for best therapeutic decisions. As well as there is a need to identify molecular markers of systemic relapse in cervical cancer which will help in identifying the patients at risk of systemic relapse and justify the option of offering adjuvant systemic therapy despite aggressive loco regional treatment.
[1]. Raphael JC, Ram TS, Pavamani S, Choudharie L, Viswanathan PN, Squamous cell carcinoma cervix with metastasis to pyloroduodenal regionJ Can Res Ther 2011 7:183-84. [Google Scholar]
[2]. Marcial-Rojas RA, Meigs JV, Cancer of the cervix uteri. A review of 169 necropsied casesAm J Pathol 1955 31:1077-82. [Google Scholar]
[3]. Wei SC, Su WC, Chang MC, Chang YT, Wang CY, Wong JM, Incidence, endoscopic morphology and distribution of metastatic lesions in the gastrointestinal tractJournal of Gastroenterology and Hepatology 2007 22(6):827-31. [Google Scholar]
[4]. Kanthan R, Senger JL, Diudea D, Kanthan S, A review of duodenal metastases from squamous cell carcinoma of the cervix presenting as an upper gastrointestinal bleedWorld J Surg Oncol 2011 9:113 [Google Scholar]
[5]. Juan Rosai, Gastrointestinal tractIn, Michael Houston. Rosai and Ackerman’s surgical pathology 2004 Vol.19th editionSt. Louis, MissouriElsevier publishers:740 [Google Scholar]
[6]. Juan Rosai, Female reproductive systemIn, Michael Houston. Rosai and Ackerman’s surgical pathology 2004 Vol.29th editionSt. Louis, MissouriElsevier publishers:1537 [Google Scholar]
[7]. Badib AO, Kurohara SS, Webster JH, Pickren JW, Metastases to organs in carcinoma of uterine cervix. Influence of treatment on incidence and distributionCancer 1968 21:434-39. [Google Scholar]
[8]. Uqmakli A, Bonney WA Jr, Palladino A, The nonlymphatic metastases of carcinoma of the uterine cervix. A prospective analysis based on laparotomyCancer 1978 41:1027-33. [Google Scholar]