Megaloblastic anaemia as a cause of pyrexia is a rare entity. Similarly, hyperpigmentation of skin has rarely been reported as the presenting manifestation of folate and/or vitamin B12 deficiency. The author reports the case of a patient who presented with fever and hyperpigmentation and was diagnosed to have megaloblastic anaemia secondary to vitamin B12 and folate deficiency after other infective, inflammatory/autoimmune, endocrine causes of pyrexia and hyperpigmentation were excluded by appropriate investigations. The patient responded remarkably well to the treatment with vitamin B12 and folic acid supplementation. Although presentation of megaloblastic anaemia as isolated fever or hyperpigmentation are noted in literature, simultaneous fever and hyperpigmentation as its initial presentation is exceedingly rare.
Case Report
A 62-year-old non-smoker and non-alcoholic male presented with fever and anorexia since last two months. The fever was irregular, intermittent, moderate grade, not associated with chills and rigors and without any localising symptoms. He also had easy fatigability with loss of weight and appetite. He had noted progressively increasing darkening of skin and discoloration of hair and nails for last six months. He was non-diabetic and non-hypertensive and he did not have any history of chronic intake of any drug. He enjoyed pure vegetarian diet. There was no significant past history or family history of any chronic illness like tuberculosis. He had received intravenous cefotaxime1 g twice a day for 10 days from a private practitioner but he had no relief. He had undergone total gastrectomy and oesophago-jejunostomy due to gastric cancer six years ago.
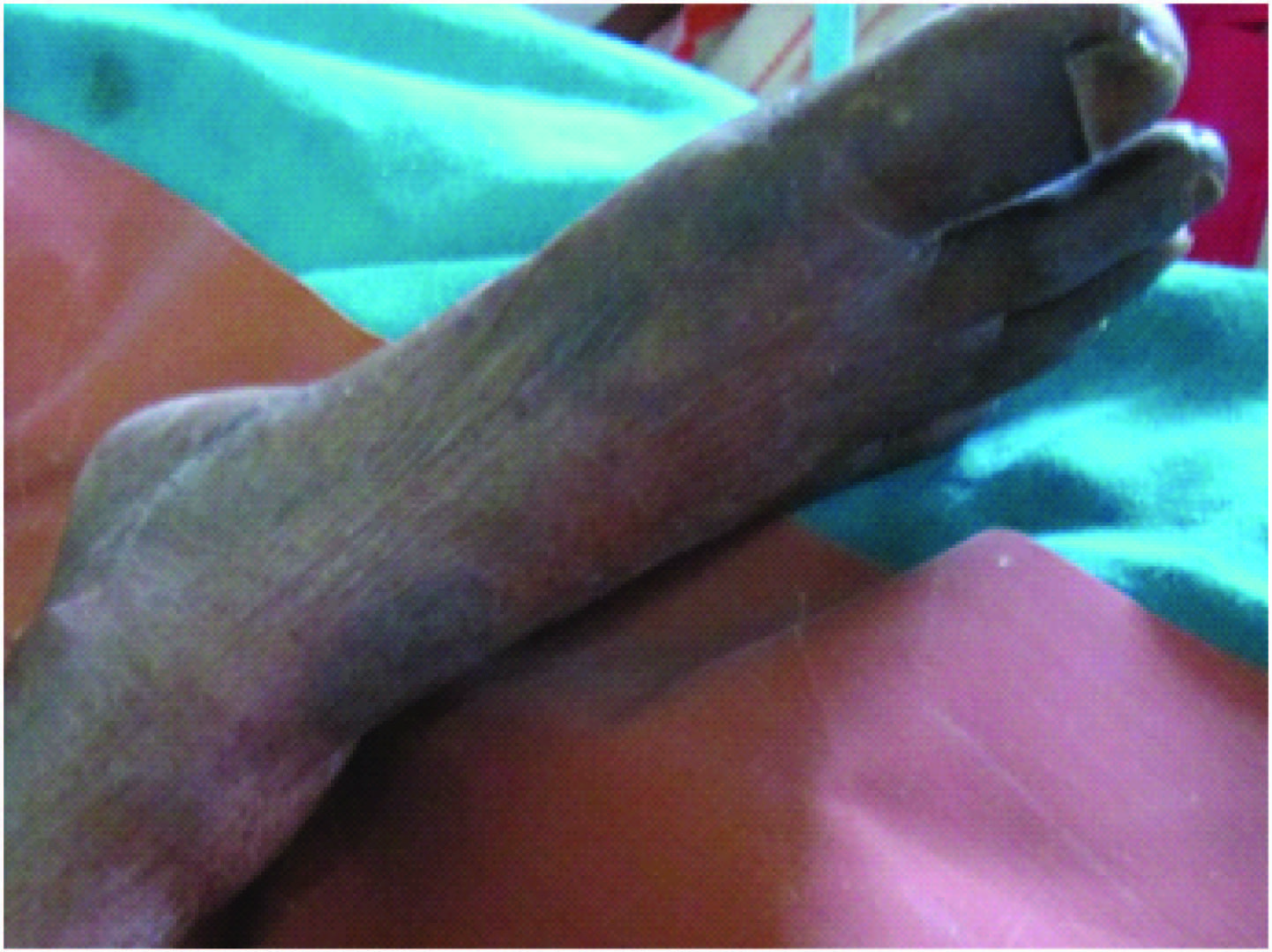
On examination, severe pallor was noted and hyperpigmentation was observed on skin of the dorsal aspect of the hands(mainly the knuckles) and the feet [Table/Fig-1,2]. The tongue was depapillated. There was no icterus, cyanosis, clubbing, lymphadenopathy, pedal oedema,rash or eschar or any peripheral stigmata of bacterial endocarditis. During examination, he was noted to be febrile with a temperature of 39.8°C but his vitals were stable. Cardiovascular examination revealed a systolic flow murmur in the aortic area.Abdominal examination revealed mild hepatosplenomegaly with no ascites. Other systemic examination was non-contributory. He was started on empiric broad-spectrum antibiotics (considering some underlying sepsis) after sending appropriate cultures.
Showing hyperpigmentation in the hands (mainly in the digits)

Showing hyperpigmentation in the feet (mainly in the toes)
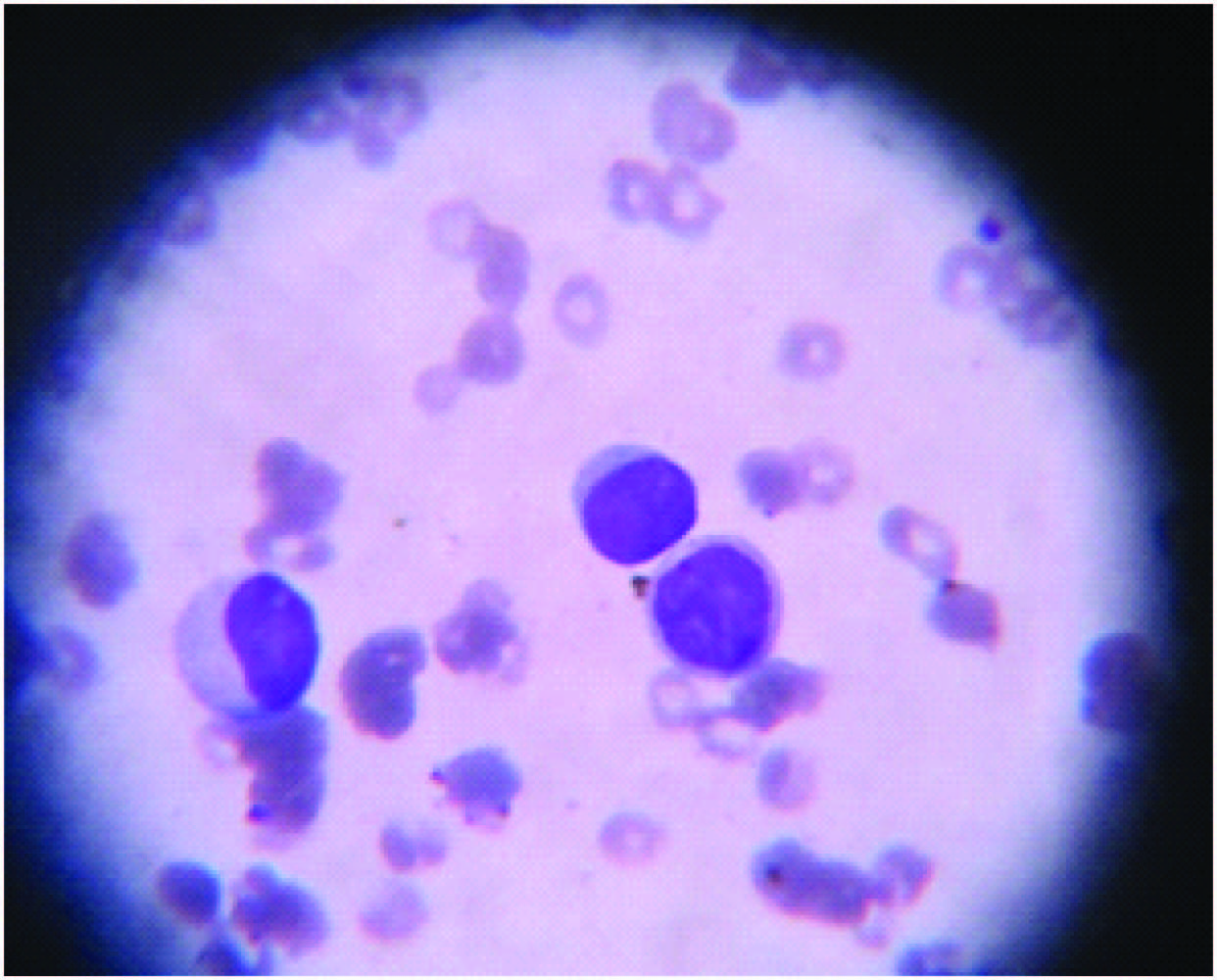
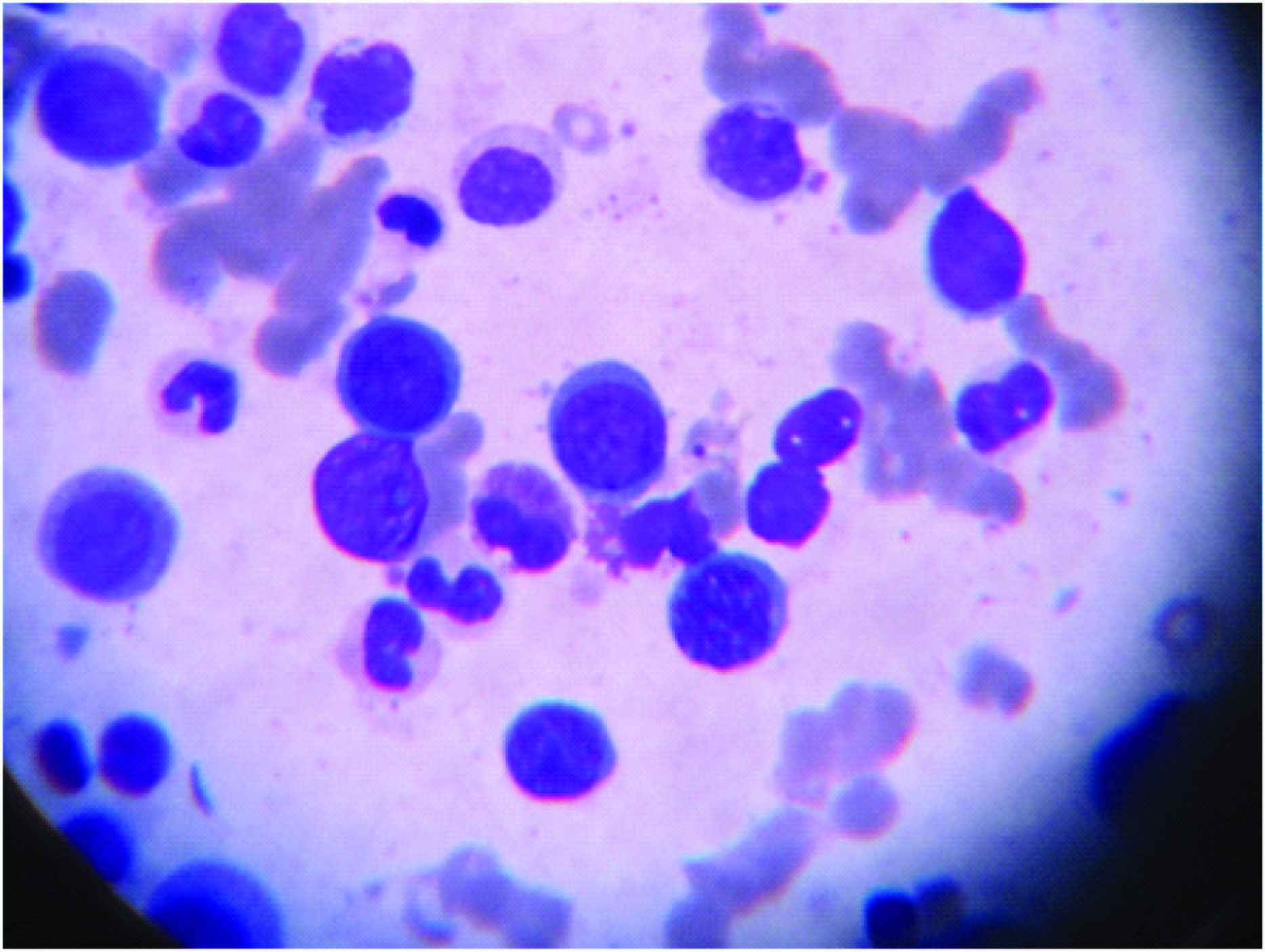
Complete blood count revealed depression of all three lineages with peripheral smear showing macrocytic RBCs with anisopoikilocytosis and hypersegmented neutrophil and few nucleated RBC [Table/Fig-3]. Bone marrow aspirate and trephine biopsy showed cellular marrow with megaloblastic erythropoiesis with altered myeloid to erythroid ratio (1:2) [Table/Fig-4]. The results of complete haemogram are summarised below in [Table/Fig-5].
Showing megaloblastic RBCs with pancytopenia in peripheral blood smear
Showing megaloblastic erythropoiesis in bone marrow
Summary of complete haemogram
| Haematological parameter | Value |
|---|
| Haemoglobin | 6.6 g/dl |
| Platelet count | 68000/cmm |
| Total WBC count | 3900/cm |
| Differential count | N:64 ;L:26; M:7; E:2; B:1 |
| Peripheral smear | Macrocytic RBCs with anisopoikilocytosis and hypersegmented neutrophil |
| Bone marrow study | Megaloblastic erythropoiesis |
Biochemical tests including renal function tests and liver function tests and serum electrolytes were completely normal. Urine microscopy, gram’s stain of sputum, Mantoux test, Chest X ray showed no abnormal result. Repeated blood culture, urine culture revealed no growth. Malaria parasite was not noted in peripheral smear and Dual antigen test was negative. Abdominal ultrasonography revealed mild hepatosplenomegaly but no intra-abdominal lymphadenopathy or ascites.Serum level of vitamin B12 was diminished (76pg/ml;N:150-900 pg/ml);antibody to intrinsic factor and parietal cell antibodies were absent;serum folate levels was also found to be somewhat low at 3.2μg/L (normal range 4–24 μg/L). Iron studies were normal. Cosyntropin stimulation test (done to exclude primary adrenal insufficiency as cause behind hyperpigmentation) showed normal hypothalamo-pituitary-adrenal axis.Upper gastrointestinal endoscopy(done to exclude any gastropathy or enteropathy as contributory factor to vitamin B12 and/or folate depletion)was normal and histopathological examination of the second part of the duodenum showed normal mucosa with no evidence of atrophic gastritis, tropical sprue, celiac sprue or Crohn’s disease. Fever did not respond to antibiotics.Therefore, in the absence of any positive microbiological tests and definite evidence of B12 and folate deficiency, antibiotics were stopped with initiation of B12 (intramuscular cyanocobalamin) and oral folate supplementation. After two days of B12 and folate treatment, he became afebrile, and he noticed improvement in subjective symptoms (malaise and fatigue) within two weeks. Patient was initially prescribed intramuscular injection of vitamin B12 (1000 mg) daily for ten days, then weekly for one month and then advised monthly doses for life-long. Along with it, oral folate (5 mg daily) was asked to continue life-long.Diagnosis of fever and hyperpigmentationsecondary to vitamin B12 and folate deficiency was established.Subsequent measurement of B12 and folate levels at follow-up after 3 months showed almost normalisation along with improvement in skin pigmentation.
Discussion
Vitamin B12 is a water soluble vitamin, present in various forms: cyanocobalamin (vitamin B12), hydroxocobalamin (vitamin B12a), aquacobalamin (vitamin B12b), nitritocobalamin (vitamin B12c), 59-deoxyadenosylcobalamin (coenzyme B12), and methylcobalamin (methyl B12) [1]. Both folate and B12act as coenzymes which participate in one carbon metabolism in which a carbon unit from serine or glycine is transferred to tetrahydrofolate (THF) to form methylene-THF; these reactions are important in synthesis of DNA and RNA [2]. Gastrectomy causes vitamin B12 deficiency due to a lack of Castle’s intrinsic factor orto bacteria breeding in the intestine.The median time to develop megaloblastic anaemia following total gastrectomy is 15 months and without proper treatment, it appears in almost all patients three years after a gastrectomy especially in elderly patients who usually have decreased body stores [3]. Vegetarians have increased predisposition to B12 deficiency as it is obtained only from animal sources [4]. The folate and B12 deficiency may be due to the prior gastrointestinal surgery and vegetarian food habits and B12 deficiency probably compounded by the patient’s age [3]. The index patient (62-year-old) probably has developed severe megaloblastic anaemia due to combination of these factors.
The characteristic dermatological sign of vitamin B12 deficiency is cutaneous pigmentation, which can be reversed by administration of vitamin B12 [5]. Increased cutaneous pigmentation is especially noticed in palmar creases, on the dorsa of hands and feet, in intertriginous areas, on oral mucosa and in recent scars. A few patients exhibit generalized hyperpigmentation [6]. Baker et al., provided an early description of hyperpigmentation as a sign of vitamin B12 deficiency in 1963 [7]. Lee et al., reported asimilar case in a 65-year-old Korean female [8] while Ahuja et al., reported similar picture in a 10-month-old child [9]. Marks et al., reported yet another case in a 65-year-old female [10]. Srivastava et al mentioned a case of reversible darkening of skin and discoloration of hair and nails in a 34-year-old male [11]. The index patient was a 62-year-old male.
The mechanism of hyperpigmentation is only postulatory. According to one hypothesis, the deficiency of vitamin B12 decreases the level of glutathione and the melanocytes are stimulated as the tyrosinase-inhibiting effect of glutathione gets diminished.Vitamin B12 deficiency lowers the intracellular redox potential with a concomitant decrease in the reduced glutathione to oxidized glutathione ratio. Once the tyrosinase-inhibiting effect of reduced glutathione has diminished, the epidermal melanocytes are then stimulated to produce melanin [12]. Another hypothesis is that high intracellular tyrosine levels, which may be found in vitamin B12 deficiency, produce excess DOPA, presumably by mass effect inducing excess melanin production [8]. In still another possibility, hyperpigmentation has been attributed to a defect in the melanin transfer between melanocytes and keratinocytes, resulting in pigmentary incontinence. Infact, an increased number of melanocytes in the basal layer with numerous melanophages in the papillary dermis and increased melanin in the dermis and epidermis have been known to occur [13]. Cutaneous hyperpigmentation is usually associated with reversible premature greying of hairs [14].
The incidence of pyrexia in megaloblastic anaemia has been reported about 40-65%. Negi et al., reported a case of anicteric 18-year-old male with pyrexia, bicytopenia, and macrocytosissecondary to B12 deficiency [15]. Singanayagam et al., reported a young male with pyrexia of 6-weeks’ duration, severe pancytopenia and mild hyperbilirubinemia secondary to folate deficiency and low normal vitamin B12 [16]. The index case involved an elderly male patient who presented with low-grade pyrexia, pancytopenia with macrocytosis secondary to combined deficiency of B12 and folate. In all the 3 cases including the index one, pyrexia subsided 24 to 72 h after initiation of supplementation therapy.
Association of pyrexia and megaloblastic anaemia appears to be causal, whereas in other types of anaemia, it seems more coincidental [17]. Severity of pyrexia usually correlates with degree of anaemia and improve swiftly after correction of anaemia. It is seen in deficiency of both B12 or folic acid either acting alone or in combination. This is a noticeable feature considering the fact that hyperpigmentation is usually seen in pernicious anaemia only, not in isolated folate deficiency megaloblastic anaemia. Usually fever is low grade; however high grade fever may be seen in those patients who present with more severe anaemia. Those with severe disease characterized by high Mean Corpuscular Volume (MCV), low haematocrit (<20%), low thrombocytopenia (<100×109 /L), high Lactate Dehydrogenase (LDH>1000 IU/L), and unconjugated hyperbilirubinemia (>1.5 mg/dL) are more likely to be febrile [18].
As in case of hyperpigmentation, the exact cause of pyrexia in megaloblastic anaemia is not known. Earlier, it was theorized that it may reflect a defect in oxygenation to the temperature regulatory centres in the brain [19]. However, it fails to explain why the fever seen in megaloblastic anaemia is not noted in other forms of anaemia. Lack of correlation between neurological manifestation and pyrexia in megaloblastic disease also does not lend credibility to this theory. Finally, studies have also shown that a rise in temperature might cause depletion of folate stores, both in red blood cells and serum, leading to disturbance of folate metabolism [20]. So, whether pyrexia is the cause of folate deficiency or vice versa is not certain at present.
Another proposed mechanism is that megaloblastic anaemia causes remarkable intramedullary haemolysis and possibly ineffective leucopoiesis and thrombopoiesis. Increased activity in bone marrow may be related to systemic pyrexia as premature destruction of hematopoietic precursors possibly releases intracellular substances, which might function as systemic pyrogens [17]. Dramatic response to B12 and/or folate supplementation (within 24 to 72 h) strongly supports the above hypothesis suggesting that the rapid correction of ineffective haematopoiesis may be curative [21].
An important but controversial theory is that the commonest cause of fever in megaloblastic anaemia is infection, to which the individual is much more susceptible in this disease due to impaired intracellular killing of ingested bacteria by the neutrophils and macrophages. The metabolic activation is reduced by 35% in the leukocytes that are deficient in B12 (but not with folate deficiency) [22].
In a study by Tahlan et al., the incidence of low-grade fever in nutritional megaloblastic anaemia varied from 28% to 60% [23]. Although the isolated occurrence of low grade fever in megaloblastic anaemia is common, the coexistence of fever and hyperpigmentation asshown in the index case is much uncommon. Recently, Mangaraj et al., reported a similar case in a 24-year-old male [24]. Khanduri et al., reported persistent low-grade fever in 70% of the cases with B12 and/or folate deficiency. In the same study, hyperpigmentation was found in only 18% cases [5]. However, the exact percentage of patients having both fever and hyperpigmentation was not given.
Conclusion
Measurement of Vit B12 and folate levels should be considered in all patients of pyrexia with features of megaloblastic anaemia and/or pancytopenia after ruling out infections, inflammatory and endocrine causes. However, persistence of fever for several days or its failure to decrease even after 2 - 3 days of initiating vitamin B12 and folate therapy should suggest the possibility of another aetiology for fever.It can be concluded that megaloblastic anaemia is a rare but treatable cause of fever of unknown cause as well as hyperpigmentation that responds well to the treatment. It should be considered in any patient who presents with unexplained pyrexia and/or hyperpigmentation, especially if pancytopenia is present.
Consent
Informed consent was taken from the patient regarding publication of this case report.
[1]. Gomber S, Kela K, Dhingra N, Clinico-hematological profile of megaloblasticanemiaIndian Pediatr 1998 35:55-58. [Google Scholar]
[2]. Selhub J, Folate, vitamin B12 and vitamin B6 and one carbon metabolismJ Nutr Health Aging 2002 6(1):39-42. [Google Scholar]
[3]. Hu Y, Kim HI, Hyung WJ, Song KJ, Lee JH, Kim YM, Vitamin B(12) deficiency after gastrectomy for gastric cancer: an analysis of clinical patterns and risk factorsAnn Surg 2013 258(6):970-75. [Google Scholar]
[4]. Nishimura O, Kibara N, PostgastrectomyanemiaNihon-Rinsho 1991 49:230-36. [Google Scholar]
[5]. Khanduri U, Sharma A, Megaloblastic anaemia: prevalence and causative factorsNat Med J India 2007 20:172-75. [Google Scholar]
[6]. Hoffman CF, Palmer DM, Papadopoulos D, Vitamin B12 deficiency: A case report of ongoing cutaneous hyperpigmentationCutis 2003 71:127-30. [Google Scholar]
[7]. Baker SJ, Ignatius M, Johnson S, Hyperpigmentation of the skin assign of vitamin B12 deficiencyBr Med J 1985 1:1713-15. [Google Scholar]
[8]. Lee SH, Lee WS, Whang KC, Lee SJ, Chung JB, Hyperpigmentation in megaloblasticanemiaInt J Dermatol 1988 27:571-75. [Google Scholar]
[9]. Ahuja SR, Sharma RA, Reversible cutaneous hyperpigmentation in vitamin B12 deficiencyIndian Pediatr 2003 40:170-71. [Google Scholar]
[10]. Marks VJ, Briggaman RA, Wheeler CEJ, Hyperpigmentation in megaloblastic anemiaJ Am AcadDermatol 1985 12:914-15. [Google Scholar]
[11]. Srivastava N, Chand S, Bansal M, Srivastava K, Singh S, Reversible hyperpigmentation as the first manifestation of dietary vitamin B12 deficiencyIndian J Dermatol Venereol Leprol 2006 72(5):389-90. [Google Scholar]
[12]. Lin SH, Sourial NA, Lu KC, Hsueh EJ, Imerslund-Grasbeck syndrome in a Chinese family with distinct skin lesions refractory to vitamin B12J Clin Pathol 1994 47:956-58. [Google Scholar]
[13]. James NG, Alvin JC, Epidermal Change in vitamin B12 DeficiencyArch Dermatol 1973 107:231-35. [Google Scholar]
[14]. Noppakun N, Swasdiskul D, Reversible hyperpigmentation of skin and nails with white hair due to vitamin B12 DeficiencyArch Dermatol 1986 122:896-99. [Google Scholar]
[15]. Negi RC, Kumar J, Kumar V, Singh K, Bharti V, Gupta D, Kashyap R, Vitamin B12 deficiency presenting as pyrexiaJ Assoc Physicians India 2011 59:379-80. [Google Scholar]
[16]. Singanayagam A, Gange N, Jones H, Folate deficiency presenting as pyrexia: a case reportCases J 2008 1(1):275 [Google Scholar]
[17]. McKee LC Jr, Fever in megaloblasticanemiaSouth Med J 1979 72(11):1423-24. [Google Scholar]
[18]. Jones RV, Payne RW, The occurrence of fever in anemiaPractitioner 1960 184:618-20. [Google Scholar]
[19]. Manuel K, Padhi S, Varghese RG, Pyrexia as a presentation of Megaloblastic Anemia: A Case Report and Literature ReviewIran J Med Sci 2013 38(2):198-201. [Google Scholar]
[20]. Osifo BO, Lukanmbi FA, Familusi JB, Increase of body temperature and folic acid metabolismActa Vitaminol Enzymol 1981 3:177-81. [Google Scholar]
[21]. Davidson S, Clinical picture of pernicious anemia prior to introduction of liver therapyin 1929 and in Edinburgh subsequent to 1944Lancet 1957 1:241-43. [Google Scholar]
[22]. Kaplan SS, Basford RE, Effect of Vitamin B12 and Folic Acid Deficiencies on Neutrophil functionBlood 1976 47:801-05. [Google Scholar]
[23]. Tahlan A, Bansal C, Palta A, Chauhan S, Spectrum and analysis of bone marrow findings in anemic casesIndian J Med Sci 2008 62:336-39. [Google Scholar]
[24]. Mangaraj S, Sethy G, Behera SK, Sahu NC, An interesting case of fever, pancytopenia and hyperpigmentationAnn Trop Med Public Health 2013 6:586-88. [Google Scholar]