Adenoid Cystic Carcinoma– A rare Differential Diagnosis for a mass in the External Auditory Canal
Vishnu Prasad1, Vijendra S Shenoy2, Raghavendra A Rao3, Panduranga M Kamath4, Haseena Shihab5
1 Consultant, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
2 Associate Professor, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
3 Associate Professor, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
4 Professor, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
5 Junior Resident, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vishnu Prasad, Consultant, Department of Otorhinolaryngology – Head & Neck Surgery, Kasturba Medical College, Mangalore, Manipal University, Karnataka – 575001, India. E-mai : dr.vishnukp@yahoo.com
Primary external auditory canal malignancies are very rare; in which, adenoid cystic carcinoma is extremely rare tumour accounting for approximately 5%. Majority of the patients presents with unilateral severe or dull aching constant ear pain of prolonged duration, reduced hearing and mass in the External Ear. These tumours are treated with aggressive surgical excision and adjuvant radiotherapy. Despite this, the overall prognosis is poor due to recurrences and distant metastasis. We report a rare case of adenoid cystic carcinoma in a 36-year-old female, who presented with right ear pain for the last one year. She was treated with wide local excision of the mass followed by adjuvant radiotherapy.
Adenoid cystic carcinoma, Ceruminous gland malignancy, Hearing loss, Otalgia
Case Report
A 36-year-old south Indian female came to the outpatient department with one year history of constant right ear pain and minimal hearing impairment. She had no history of ear discharge, tinnitus, bleeding from ear and vertigo. No previous history of surgery or trauma was noted. Physical examination showed approximately 1x1cm elevated lesion on the posterior and inferior wall of the cartilaginous external auditory canal (EAC), partially occluding the lumen. No cervical lymphadenopathy was noted. Examination of the parotid gland and facial nerve was unremarkable. A contrast enhanced computed tomography (CECT) scan of temporal bone revealed isodense enhancing mass lesion measuring1x 1cm arising from posterior and inferior canal wall, with no erosion of bone [Table/Fig-1]. Biopsy of the swelling was performed. Histopathological examination revealed adenoid cystic carcinoma with perineural invasion [Table/Fig-2a,b,c,d]. Patient underwent wide local excision, and reconstruction with split thickness graft, followed by adjuvant radiotherapy. Gross specimen of the excised mass from the EAC is shown in [Table/Fig-3]. During last clinical examination; chest X-ray, ultrasound abdomen and CT scan were repeated. At 10 months, postoperatively, the patient had shown no signs of recurrence.
Contrast enhanced computed tomography (CECT) scan of temporal bone showing isodense enhancing mass lesion (block arrow) arising from posterior and inferior wall of right ear canal, with no erosion of bone

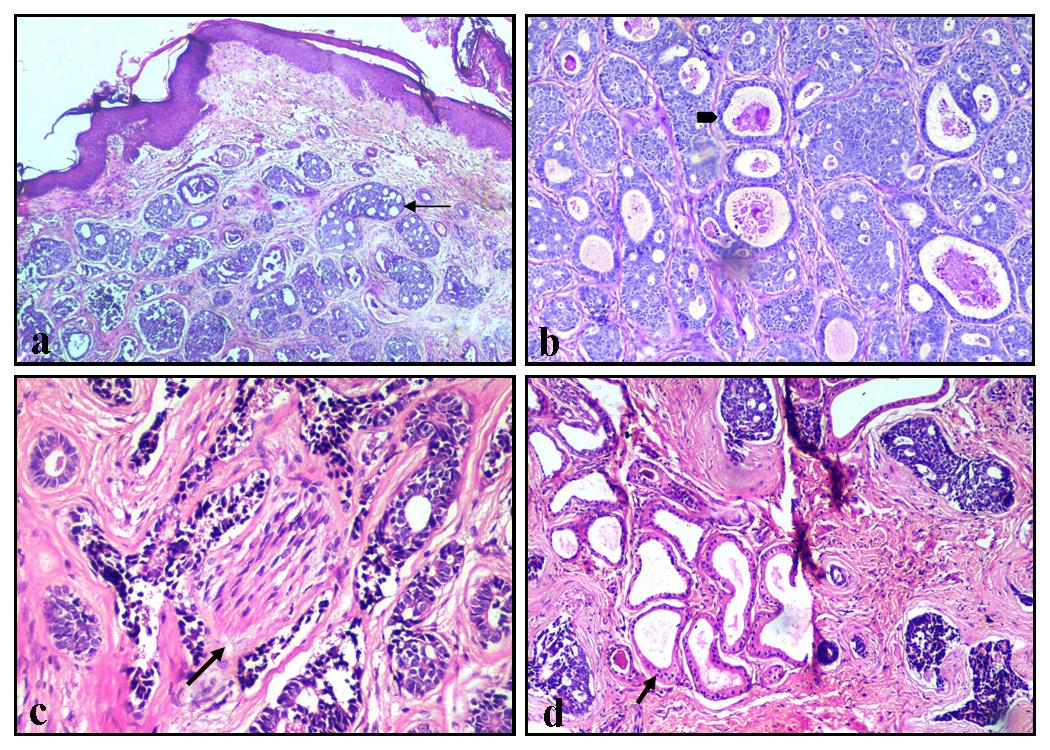
a)Adenoid cystic carcinoma showing the tumor cells in cribriform patterns (arrow). 100X, b) Adenoid cystic carcinoma in solid pattern and glands lined by basaloid cells. The lumen of the glands showing mucopolysaccharide secretions (arrow head). 400X, c) Adenoid cystic carcinoma with perineural invasion (nerve pointed by arrow), the hallmark of the lesion. 400X, d) Tumor tissue surrounding the normal ceruminous glands (arrow)
Wide excision of Adenoid cystic carcinoma of external auditory canal – Surgical specimen

Discussion
Adenoid Cystic Carcinoma (ACC) arising from the EAC are extremely rare approximately 5%; others with more than 80% being squamous cell carcinoma [1]. Therefore adenoid cystic carcinoma arising from the EAC is very rarely encountered in the clinical practice. ACC of the head and neck is usually found in the salivary glands, oral cavity, palate, nasal cavity, and nasopharynx [2]. The mean age for ACC reported is at fifth decade, and is two times more common in women than men [1]. The ACC of the EAC is characterized by an indolent clinical course, which usually leads to a delayed diagnosis of the condition and therefore management. Majority of the patients presents with unilateral severe or dull aching constant ear pain of prolonged duration. They also complain of reduced hearing at later stages because of the mass in the EAC [3–5]. The clinical presentation was similar in our case. ACC may present as a polypoidal mass, epithelial ulceration with associated granulation tissue [6]. The cause for the ear pain may be due to early perineural invasion by these tumours.
A wide/deep incisional biopsy should be performed in every EAC lesion as it is imperative for the diagnosis of ACC; otherwise it is frequently missed in superficial biopsy. While reporting the biopsies from the external auditory canal, one should keep the ACC as one of the differential diagnosis. This rare neoplasm can metastasis into the central nervous system in patients with occult malignant neoplasm [7,8].
Three main histological patterns of ACC have been described: tubular, cribriform and solid. In our patient, histopathological evaluation of the resected mass confirmed it to be of cribriform subtype. These tumours are positive for cytokeratin and S-100 protein, which indicates ceruminous gland origin [8,9].
Gadolinium-DTPA contrast enhanced MRI is most helpful in demonstrating infiltration into surrounding structures [2,10]. Aggressive surgical resection with adjuvant radiotherapy is the standard treatment for local disease control [9]. Important prognostic factors include positive surgical margins, parotid gland and surrounding structures and bone involvement [3,9]. Inspite of aggressive and early management, patients with ACC of EAC often experience recurrences. Metastasis to regional lymph nodes and distant sites like lungs were well noted [1].
Conclusion
Patients with long standing otalgia, decreased hearing and ear canal mass should be considered for early and deep incisional biopsy along with imaging. Early aggressive surgical management with adjuvant radiotherapy may help to prevent distant metastasis.
[1]. Dong F, Gidley PW, Ho T, Luna MA, Gingsberg LE, Sturgis FM, Adenoid cystic carcinoma of external auditory canalLaryngoscope 2008 118(9):1591-96. [Google Scholar]
[2]. Sigal R, Monnet O, de Baere T, Micheau C, Shapeero LG, Julieron M, Adenoid cystic carcinoma of the head and neck: evaluation with MR imaging and clinical-pathologic correlation in 27 patientsRadiology 1992 184:95-101. [Google Scholar]
[3]. Perzin KH, Gullane P, Conley J, Adenoid cystic carcinoma of external auditory canal. A clinicopathological study of 16 casesCancer 1982 50:2873-83. [Google Scholar]
[4]. Nayak SP, Walke VA, Helwatkar SB, Bobhate SK, Adenoid cystic carcinoma of the external auditory canal: Report of two casesIndian J Pathol Microbiol 2009 52:540-42. [Google Scholar]
[5]. Arshad MH1, Khalid U, Ghaffar S, Adenoid cystic carcinoma of the external auditory canalJ Coll Physicians Surg Pak 2009 19(11):726-28. [Google Scholar]
[6]. Hicks GW, Tumours arising from the glandular structures of the external auditory canalLaryngoscope 1983 93(3):326-40. [Google Scholar]
[7]. Garbyal RS, Kumar M, Bohra A, Adenoid cystic carcinoma of ceruminous gland: a case reportIndian J PatholMicrobiol 2006 49:587-89. [Google Scholar]
[8]. Liu SC1, Kang BH, Nieh S, Chang JL, Wang CH, Adenoid cystic carcinoma of the external auditory canalJ Chin Med Assoc 2012 75(6):296-300. [Google Scholar]
[9]. Zainor S, Mamat H, Saad SM, Adenoid cystic carcinoma of external auditory canal: A case reportEgyptian Journal of Ear, Nose, Throat and Allied Sciences 2013 14(1):41-44. [Google Scholar]
[10]. Conlin PA, Mira JL, Graham SC, Kaye KS, Cordero J, Ceruminous gland adenoid cystic carcinoma with contralateral metastasis to the brainArch Pathol Lab Med 2002 126:87-89. [Google Scholar]