Management of a Case of Ruptured Pseudoaneurysm and Stenosis of Femoral Artery Caused by Femoral Osteochondroma
Vikas Deep Goyal1, Vipin Sharma2, Sandeep Kalia3, Shivam Pathak4
1Assistant Professor, Department of Cardiothoracic and Vascular Surgery,Dr. RPGMC Kangra, Tanda (H.P), India.
2Associate professor Orthopedics, Department of Orthopedics,Dr. RPGMC Kangra, Tanda (H.P), India.
3Assistant Professor Orthopedics, Department of Orthopedics,Dr. RPGMC Kangra, Tanda (H.P), India.
4PJunior Resident Orthopedics, Department of Orthopedics,Dr. RPGMC Kangra, Tanda (H.P), India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vikas Deep Goyal, Assistant Professor, Department of Cardiothoracic and Vascular Surgery, Dr. RPGMC Kangra, Tanda (H.P)-176001, India.
E-mail: goyalv34@gmail.com
We present a rare case of ruptured pseudoaneurysm of distal femoral artery due to osteochondroma in a 21-year- old male. The patient was initially treated for osteochondroma as ruptured pseudoaneurysm was not suspected. Diagnosis of ruptured pseudoaneurysm could only be made intraoperatively when rent in the femoral artery was found along with surrounding hematoma and obstruction in the distal femoral artery. Patient underwent multiple surgeries (resection of osteochondroma and femoro-popliteal bypass) and recovered well with palpable pulsations in the operated limb.
Pain, Bone tumor, Femoro-popliteal bypass
Case Report
A 21-year-old male patient presented with history of pain and paresthesia in right lower limb alongwith difficulty in walking. The patient was investigated and roentgenogram of right femur revealed presence of a bone tumor arising from posterior aspect as seen in lateral view [Table/Fig-1].
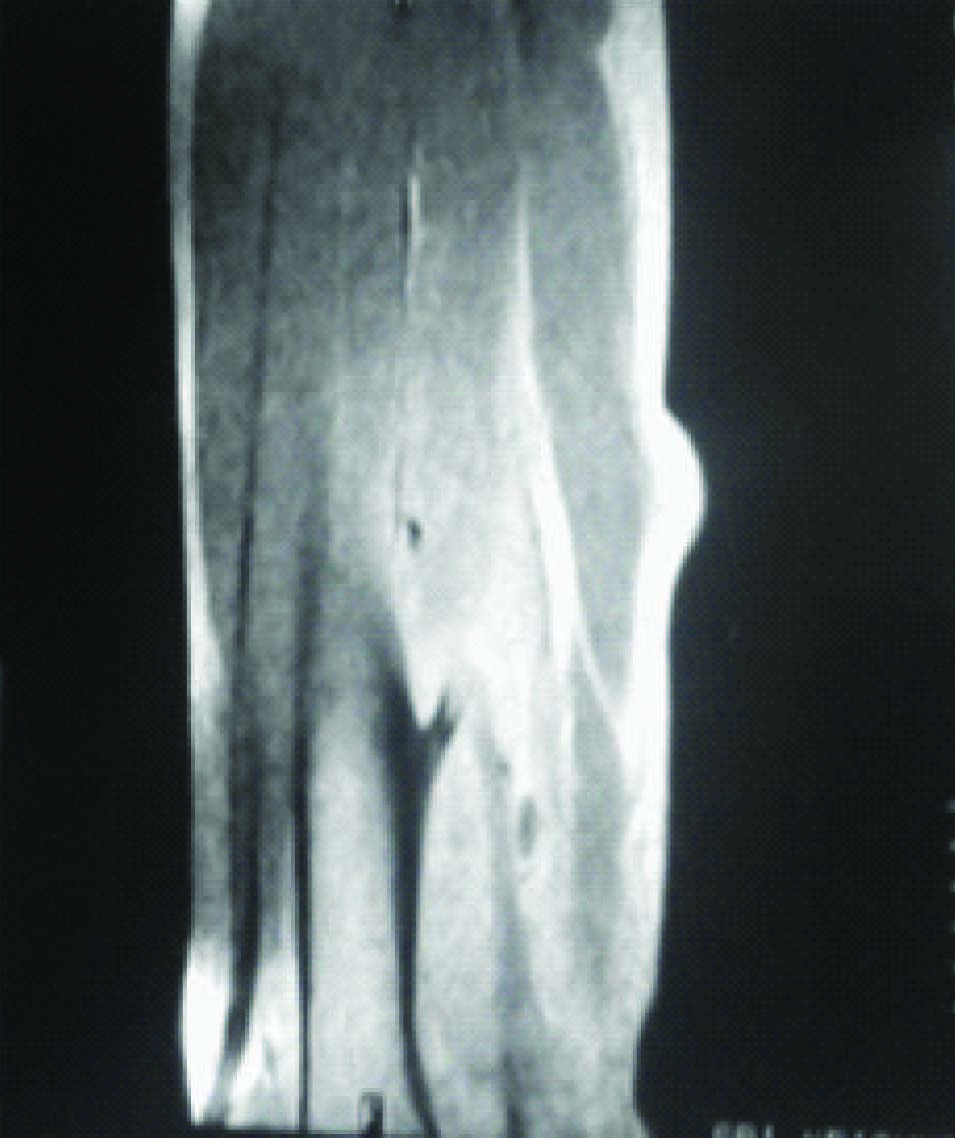
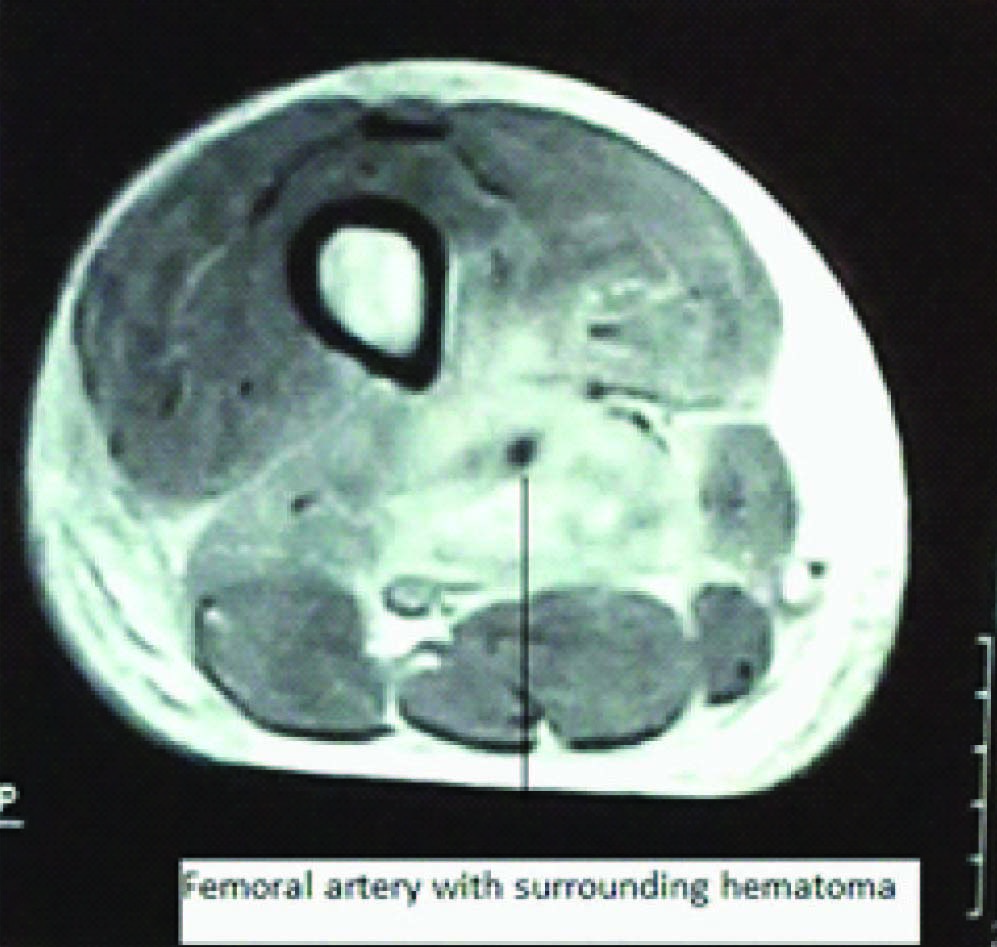
Magnetic resonance imaging (MRI) was also done and it revealed exostosis arising from femur with surrounding hematoma, without any evidence of infiltration into surrounding structures [Table/Fig-2a,2b].
Computed tomography (CT) Angiogram although of valuable information was not done at this stage as the presence of a ruptured pseudoaneurysm was not suspected initially. Tumor was considered benign and surgical intervention in the form of excision of the tumor was planned. Spinal anesthesia was given and patient was turned in to prone position and a tourniquet was placed around upper thigh. Midline incision in the posterior aspect of lower part of right thigh was given and posterior thigh muscles were retracted to reach the tumor. Hematoma and clots were evacuated, injury to femoral artery was not suspected at that time, moreover presence of a hematoma had distorted the muscular planes and structure differentiation was difficult. Tumor was excised and sent for histopathology examination. There was no active bleeding, even after deflation of tourniquet, probably due to presence of a clot and or hypotension caused by anesthesia. After ensuring hemostasis and inserting a suction drain standard closure was done. The patient was well, without any complaints and there was minimal drainage therefore drain was removed on second post-operative day. The patient again developed pain and swelling few days later at the operative site and was taken for re-exploration under combined epidural and spinal anesthesia. Re-exploration was done through the same incision and large hematoma along with clots were found, which were removed. After removal of the clots bleeding started from a rent in femoral artery (neck of pseudoaneurysm) it was at that time diagnosis of ruptured pseudoaneurysm was made. Proximal control on femoral artery stopped the bleeding and there was no back bleeding from the distal end. The distal segment of femoral artery/proximal popliteal artery was found completely obliterated with unhealthy vessel wall and surrounding tissues. Rent in the femoral artery was closed with polypropylene 6-0 sutures. As the soft tissues were unhealthy and there was inadequate normal proximal and distal segment of femoral artery/popliteal artery for placement of interposition vein graft for repair of femoral artery through the posterior approach, decision for femoro-popliteal bypass in a planned way avoiding the site of previous surgery was taken. Patient was carefully monitored for ischemic symptoms and signs. Fortunately the patient was having mild ischemic symptoms only although, distal pulsations were absent and capillary refill was delayed but there was no cyanosis as the collaterals had maintained the perfusion. Patient was again taken for surgery five days after evacuation of hematoma, for femoro-popliteal bypass under combined epidural and spinal anesthesia in a planned way. Femoral artery was exposed in the groin and popliteal artery below knee was exposed using a medial approach, great saphenous vein was also harvested from right groin to upper one third of right leg through multiple incisions in right thigh and leg. Patient was heparinised 1mg/kg, proximal and distal control in the femoral artery was taken and end to side proximal anstomosis of reversed saphenous vein to femoral artery was done using polypropylene 6-0 sutures. Graft was thereafter tunneled through the incision used for harvesting of saphenous vein and end to side distal anstomosis of reversed saphenous vein to popliteal artery was also done using polypropylene 6-0 suture. Standard closure was done after hemostasis.
The patient was discharged on 12th postoperative day after CT Angiogram revealed patent graft [Table/Fig-3], there was minor leak from mid portion of the graft which subsequently closed, Patient came for follow-up six months after the procedure and was doing well and had palpable pulsations in the operated limb. Colour Doppler study was also done at that time and it revealed patent graft without any leak or pseudoaneurysm formation.
Discussion
Ruptured pseudoaneurysm of femoral artery due to osteochondroma is a very rare condition with limited literature available [1,2]. It is difficult to pre-operatively diagnose a ruptured pseudoaneurysm [2,3] caused by osteochondoma unless high index of suspicion is there. Available reports in literature on pseudoaneurysm caused at various locations by osteochondomas/bony exostosis include involvement of popliteal artery [4] femoral artery [5], brachial artery [6], tibial and peroneal arteries. A team approach comprising of vascular surgeons, orthopedic surgeons and radiologist is required for diagnosing the condition preoperatively and it’s appropriate management. Osteochondomas are a common tumor found in young adults and is usually found in metaphysis of long bones. Excision of osteochondoma is indicated as there are chances of malignant transformation. It can also cause pressure symptoms on adjacent structures and rarely can lead to pseudoaneurysm formation as happened in this case.
Cases of pseudoaneurysm caused by osteochondroma if diagnosed pre-operatively are managed by excision of the tumor and either direct repair of the vessel or patch arterioplasty or interposition vein graft depending on the situation in the same sitting. In this case femoro-popliteal bypass was performed as the distal femoral artery/popliteal artery was found damaged beyond repair and the presence of interposition graft in an infected and unhealthy tissue could have lead to blow out at the anastomotic site and complicated the management further. Other option in the management can be endovascular stenting of the pseudoaneurysm followed by excision of the tumor.
Taneda Y et al., [7] in their report published in year 2004 stated that pseudoaneurysm formation in a case of osteochondroma is very rare and they found 40 similar articles in English literature. We also searched the literature on Pubmed using terms "pseudoaneurysm "and "osteochondroma" and we could find 75 such articles (case reports) majority of which were related to unruptured aneurysms involving popliteal artery [8,9]. This case is an addition to the limited available literature on the diagnosis and management of ruptured aneurysm caused by osteochondroma. Management of cases with ruptured aneurysm is more complicated then cases with unruptured aneurysm. Cases with unruptured aneurysm usually can be treated in a single stage with excision of the osteochondroma alongwith repair of the vessel using any of the techniques; patch arterioplasty, ischemic symptoms also thrombosis of the veins end to end anastomosis, interposition vein or prosthetic graft or stent grafting using endovascular techniques, whereas cases with ruptured aneurysm may require multiple procedures and bypass grafting as was done in this case.
Apart from pseudoaneurysm formation osteochondomas in limbs sometimes cause stenosis/thrombosis of the artery leading to ischemic symptoms and thrombosis of the veins can lead to features of deep vein thrombosis [10]. Arterial involvement in a case of osteochndroma is not common as seen from large volume studies reported in literature on osteochondorma by Khare GN [11] and by Saglik Y et al., [12]. Delayed presentation of brachial artery pseudoaneurysm 13 years after excision of osteochondroma [13] has also been reported therefore long term follow is required for patients undergoing excision of osteochondroma.
Plain radiograph showing osteochondroma arising from posterior aspect of right femur in lateral view

MRI showing osteochondroma arising from posterior aspect of right femur in sagittal section with surrounding hematoma
MRI showing osteochondroma arising from posterior aspect of right femur in axial view with surrounding hematoma (Ruptured pseudoaneurysm)
Post-operative CT Angiogram showing patent graft of femoro-popliteal bypass and blocked segment of distal femoral/popliteal artery

Conclusion
High index of suspicion should be there for presence of pseudoaneurysm or ruptured pseudoaneurysm if bone tumor/ exostosis is seen along the course of a vessel or there is associated hematoma.
Peripheral pulsations should always be examined in a case of bone tumor involving limbs and compared to other side.
[1]. C Scotti, EM Marone, LE Brasca, GM Peretti, R Chiesa, A Del Maschio, Pseudoaneurysm overlying an osteochondroma: a noteworthy complicationJ Orthop Traumatol 2010 11(4):251-55. [Google Scholar]
[2]. Q Pellenc, C Capdevila, P Julia, JN Fabiani, Ruptured popliteal artery pseudoaneurysm complicating a femoral osteochondroma in a young patientJ Vasc Surg 2012 55(4):1164-65. [Google Scholar]
[3]. A Ballaro, AD Fox, J Collin, Rupture of a popliteal artery pseudo-aneurysm secondary to a fibular osteochondromaEur J Vasc Endovasc Surg 1997 14(2):151-52. [Google Scholar]
[4]. VK Bhalla, H Coulson, W Parker, J Wynn, WL Pipkin, CG Howell, Popliteal pseudoaneurysm caused by Nora's lesion of the femur in a young child: a rare presentation and first reportJ Pediatr Surg 2012 47(12):e55-59. [Google Scholar]
[5]. E Blazick, WB Keeling, P Armstrong, D Letson, M Back, Pseudoaneurysm of the superficial femoral artery associated with osteochondroma--a case reportVasc Endovascular Surg 2005 39(4):355-58. [Google Scholar]
[6]. SJ Koenig, AP Toth, S Martinez, JW Fletcher, RD Goldner, Traumatic pseudoaneurysm of the brachial artery caused by an osteochondroma, mimicking biceps rupture in a weightlifter: a case reportAm J Sports Med 2004 32(4):1049-53. [Google Scholar]
[7]. Y Taneda, K Nakamura, M Yano, H Nagahama, E Nakamurqa, K Niina, Popliteal artery pseudoaneurysm caused by osteochondromaAnn Vasc Surg 2004 8(1):121-23. [Google Scholar]
[8]. JM Wiater, FA Farley, Popliteal pseudoaneurysm caused by an adjacent osteochondroma: a case report and review of the literatureAm J Orthop (Belle Mead NJ) 1999 28(7):412-16. [Google Scholar]
[9]. RS Davies, U Satti, RG Duffield, Popliteal artery pseudo-aneurysm secondary to femoral osteochondroma: a case report and literature reviewAnn R Coll Surg Engl 2007 89(5):W8-11. [Google Scholar]
[10]. DA Leggett, SJ Sinnott, HN Kienzle, Pseudoaneurysm and deep vein thrombosis complicating femoral osteochondroma: multimodality imagingAustralas Radiol 2006 50(3):258-61. [Google Scholar]
[11]. GN Khare, An analysis of indications for surgical excision and complications in 116 consecutive cases of osteochondromaMusculoskelet Surg 2011 95(2):121-5. [Google Scholar]
[12]. Y Saglik, M Altay, VS Unal, K Basarir, Y Yildiz, Manifestations and management of osteochondromas: a retrospective analysis of 382 patientsActa Orthop Belg 2006 72(6):748-55. [Google Scholar]
[13]. AM Tobias, B Chang, A rare brachial artery pseudoaneurysm 13 years after excision of a humeral osteochondromaAnn Plast Surg 2004 52(4):419-22. [Google Scholar]