A Rare Case of Foreign Body Causing Recurrent Vaginal Discharge in Prepubertal Child
Vijayalakshmi.R. Gobbur1, Raghavendra.H. Gobbur2, Ashwini.G Patil3, Preetish Endigeri4
1Professor, Department of Obstetrics and Gynaecology, Shri B.M.Patil Medical College Hospital & Research Centre, Bijapur, Karnataka, India.
2Professor, Department of Paediatrics, Shri B.M.Patil Medical College Hospital & Research Centre, Bijapur, Karnataka, India.
3Post Graduate, Department of Obstetrics and Gynaecology, Shri B.M.Patil Medical College Hospital & Research Centre, Bijapur, Karnataka, India.
4Senior Resident, Department of Orthopaedics, Shri B.M.Patil Medical College Hospital & Research Centre, Bijapur, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijayalakshmi.R.Gobbur, Professor, Department of Obstetrics and Gynaecology, BLDE University’s SBM Patil Medical College, Bijapur (Now, Vijayapur) 586103, India.
Vaginal discharge in prepubertal children is mainly due to hypoestrogenic state of vaginal mucosa making it thin and alkaline leading to mucosal invasion by pathogen. In a paediatric case with persistent foul smelling , blood stained vaginal discharge not responding to medical therapy, vaginal foreign body should always be ruled out. Here, we report a 3 -year -old girl with complaint of recurrent vaginal discharge occasionally blood stained not relieved despite few antibiotics courses. On X -ray pelvis, a radioopaque foreign body hair clip was seen. Under sedation foreign body was removed by forceps following which child became asymptomatic.
Foul smelling discharge, Sexual abuse, X-Ray pelvis
Case Report
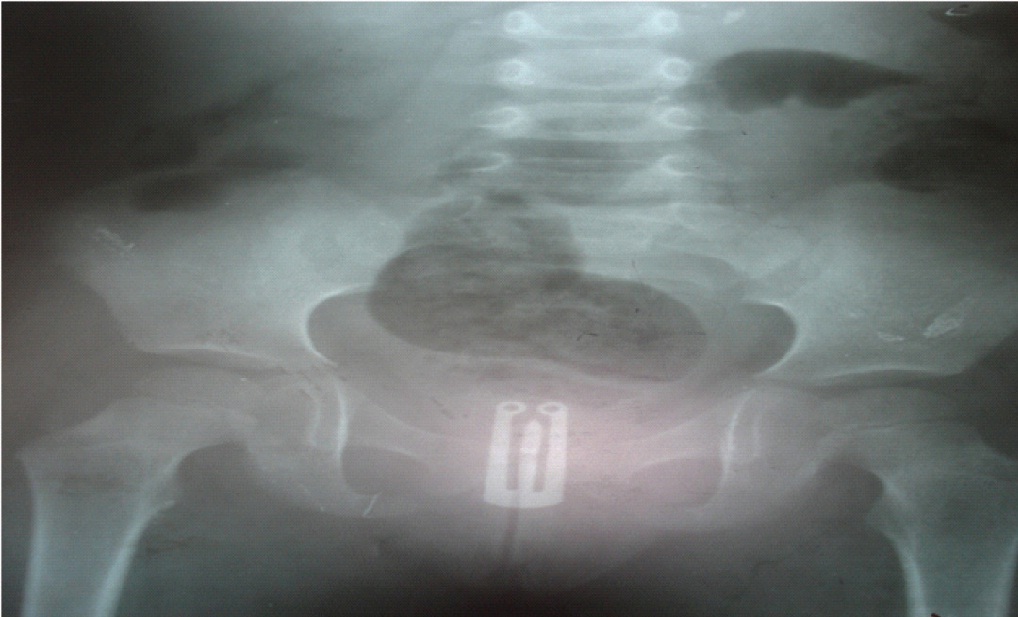
A 3-year-old girl was referred from paediatric clinic with chief complaint of discharge per vagina since one month which was moderate in quantity, mucopurulent, non blood stained and non foul smelling. There was no history of perineal or perianal itching, fever and any behavioural problems. On examination she was of sound physical and mental health. Local examination revealed normal external genitalia with redness of the introitus and slight vaginal discharge. Blood sample was sent for routine examination and the reports were within normal limits, vaginal discharge for AFB was negative and cultural sensitivity showed Klebsiella sensitive to amoxyclav, gatiflox and imipenem. Child was treated accordingly. Patient reported back after one month with same and this time with foul smelling discharge. Tridot test for RVD was negative, chest X -ray was normal, vaginal discharge culture sensitivity showed Klebsiella sensitive to co-amoxiclav, gatiflox and imipenem. Child was started on second course of antibiotics. Patient didn’t follow up and reported after three months with persistent foul smelling vaginal discharge which was slightly blood stained. The Child was sent for X-ray pelvis which revealed radioopaque foreign body (hair clip) in vagina [Table/Fig-1]. Under sedation foreign body was removed with artery, the forceps [Table/Fig-2,3], vagina was irrigated thoroughly with betadine solution and broad spectrum antibiotics were started following which child didn’t have any vaginal discharge and became asymptomatic.
Discussion
Recurrent vaginal discharge is a common gynaecological complaint in children. It is mainly due to hypoestrogenic state of vaginal mucosa with lack of acidic pH which is the main predisposing factor causing mucosal invasion by pathogen [1]. Common causes of vaginal discharge in prepubertal age groups includes:- diaper dermatitis, bacterial vulvovaginitis, fungal vulvovaginitis, lichen sclerosis, eczema, rarely foreign body and sexual abuse [2]. Although vaginal foreign body is rare it should be suspected when a child has recurrent foul smelling or blood stained vaginal discharge [3]. Diagnostic procedures include non invasive imaging as plain radiography, ultrasonography and MRI. In case of negative findings vaginal irrigation and/or diagnostic vaginoscopy should be considered [4]. Thus, in vaginal discharge not responding to repeated antibiotic therapy, then foreign body should be suspected.
Foreign bodies are reported in 4% of girls under 13 y presenting with genitourinary complaints [5]. Foreign bodies can be accidently inserted and/or by traumatic injury. Common vaginal foreign bodies are small fibrous material from clothing or carpet, small pieces of toilet paper, beads, safety pin, plastic stoppers [1,6]. Complications of unrecognised foreign body cause ulceration of vaginal wall, perforation, vesicovaginal fistula, vaginal stenosis due to scarring and adhesions, peritonitis after perforation or even complete obstruction of vagina [5]. Foreign body is usually suspected in long standing foul smelling discharge without any obvious cause 10-20% cases [5].
Approach to a suspected case of foreign body vagina is by good elaborate history taking, careful and thorough clinical examination, bimanual rectoabdomenal examination. Investigations includes routine blood count, culture and sensitivity of vaginal discharge, pelvic ultrasound, plain pelvic radiography and MRI. The use of Magnetic Resonance Imaging (MRI) has increased the localization of non metallic objects missed by USG and radiography [3,7]. Vaginoscopy with 4mm hysteroscopy under GA and vaginal irrigation with normal saline or betadine solution are used in detection and management of foreign body [8]. The child with vaginal foreign body should be assessed psychologically for underlying emotional and behavioral problem [6]. The possibility of sexual abuse should be kept in mind while treating.
P Pallavee et al., reported a case of chronic vaginal discharge in a 5-year-old, who had retained a foreign body in her vagina for 6-7 months. Removed by nephroscope (vaginoscope was not available), a yellowish structure covered with flakes of pus was found in the vagina. It was removed by a small artery forceps and was found to be a groundnut with the shell intact and concluded children presenting with persistent purulent or bloody discharge per vaginum, unresponsive to general measures and medical therapy, the possibility of a vaginal foreign body should always be considered [9].
Dahiya P reported an intravaginal foreign body of long duration in an eight and a half year old girl who was suffering from blood stained vaginal discharge for 3 y. A vaginal examination performed under general anaesthesia revealed a foreign body (lead pencil). It was concluded that in cases of peadiatric vaginitis one should always look for foreign body in vagina [10].
Plain X-ray pelvis with radioopaque foreign body (hair clip) in vagina
Plain X-ray pelvis with radioopaque foreign body (hair clip) in vagina


Conclusion
In children presenting with persistent foul smelling or blood stained vaginal discharge not responding to general hygenic measures and antibiotic therapy, the possibility of a vaginal foreign body should be considered. Plain X-ray or USG is useful as a non invasive screening tool.
[1]. K Merkley, Vulvovaginitis and vaginal discharge in the pediatric patientJ Emerg Nursing 2005 1315:400-02. [Google Scholar]
[2]. T Stricker, F Navratil, FH Sennhauser, Vulvovaginits in prepubertal girlsArch Dis Child 2003 88(4):324-26. [Google Scholar]
[3]. A Deborah, BS Simon, S Berry, Recurrent, purulent vaginal discharge with long standing presence of a foreign body and vaginal stenosisJ Pediatr Adolosc Gynecol 2003 16(6):361-63. [Google Scholar]
[4]. UR Smith, DR Berman, EH Quint, Premenarchal vaginal discharge, finding of procedures to rule out foreign bodiesJ Pediatr Adolesc Gynecol 2002 15(4):227-30. [Google Scholar]
[5]. JE Paradise, ED Willis, Probability of vaginal foreign body in girls with genital complaintsAm J Dis Child 1985 139:472-76. [Google Scholar]
[6]. PJ Adams, Benign diseases of the female reproductive tract - symptoms and signs. In: Berek JS, editors.Berek & Novak’s Gynecology 2007 14th EditionPhiladelphia Lippincott William Wilkins:434-35. [Google Scholar]
[7]. M Kihara, N Sato, N Kimura, Magnetic resonance imagning in the evaluation of vaginal foreign bodies in a young girlArch Gynecol Obstet 2001 265(4):221-22. [Google Scholar]
[8]. A Golan, S Lurie, R Sagiv, M Glezerman, Continuous flow vaginoscopy in children and adolescentsJ Am Assoc Gynecol Laparosc 2000 7(4):526-28. [Google Scholar]
[9]. P Pallavee, S Samal, P Sabita, Foreign body in vagina: a cause of persistent vaginal discharge in childrenInt J Reprod Contracept Obstet Gynecol 2013 2(2):224-25. [Google Scholar]
[10]. P Dahiya, K Sangwan, A Khosala, N Seth, Foreign body in vagina-an uncommon cause of vaginitis in childrenIndian J Pediatr 1999 (3):466-67. [Google Scholar]