Acquired Jejunal Atresia in a 2-Month-old Infant
Ankur Mandelia1, Sandeep Agarwala2
1 Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi, India.
2 Professor, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ankur Mandelia, Senior Resident, Department of Paediatric Surgery, All India Institute of Medical Sciences, New Delhi 110029, India. E-mail : drankurmandelia@gmail.com
Acquired intestinal atresia in non–necrotizing enterocolitis affected patients is very rare. We report a 2 month old male infant who presented with bilious vomiting, abdominal distension and constipation. He was exclusively breast fed, gained weight and was asymptomatic till six weeks of age. Exploratory laparotomy revealed blind-ended, dilated proximal segment and collapsed distal segment of jejunum at approximately 30 cms from duedeno-jejunal flexure, with a V-shaped mesentery defect resembling a type III-a congenital jejunal atresia.
Acquired atresia, Intestinal atresia, Intestinal obstruction
Case Report
A 2-month-old male infant was admitted with bilious vomiting, abdominal distension and constipation that were ongoing for 2 weeks. The child was born to a 24-year-old mother by spontaneous vaginal delivery at 38 wk of gestation, weighing 2400g. The pregnancy and delivery were uneventful. There was no evidence of intra-uterine ischemic insult including placental abruption, preeclampsia, intrauterine growth restriction, chorio amnionitis or placental infarction. There was no history of birth asphyxia. The child passed meconium within the first 6 h of birth, and his stooling pattern was normal until 6 wk of age. He was exclusively breast fed, gained weight and was asymptomatic till 6 wk of age.
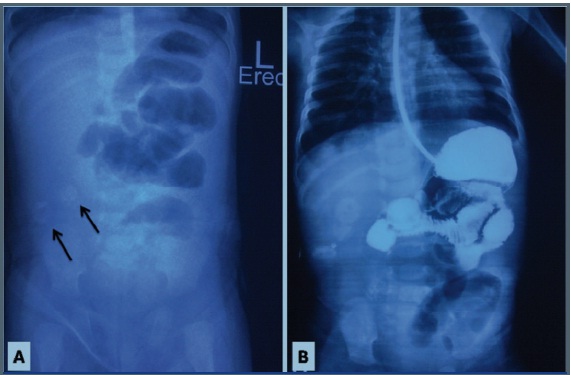
Physical examination revealed a male infant who was pale, anicteric, and severely dehydrated. He had a soft and distended abdomen with visible peristalsis. The laboratory studies including complete blood count, serum electrolytes, and renal function tests were normal. An erect abdominal plain radiograph revealed dilated bowel loops, multiple air fluid levels and flecks of calcification in the right lower quadrant [Table/Fig-1a]. An upper GI contrast study done at the referring hospital revealed dilated small bowel loops with non visualization of colon even in delayed images [Table/Fig-1b]. A barium enema study revealed normal sized colon visualized till the level of ascending colon. A working diagnosis of healed intrauterine meconium perforation with postnatal adhesive obstruction was made.
(a) An erect abdominal plain radiograph showing dilated bowel loops, multiple air-fluid levels and flecks of calcification in the right lower quadrant (arrows) (b) An upper GI contrast study showing dilated small bowel loops with non visualisation of colon
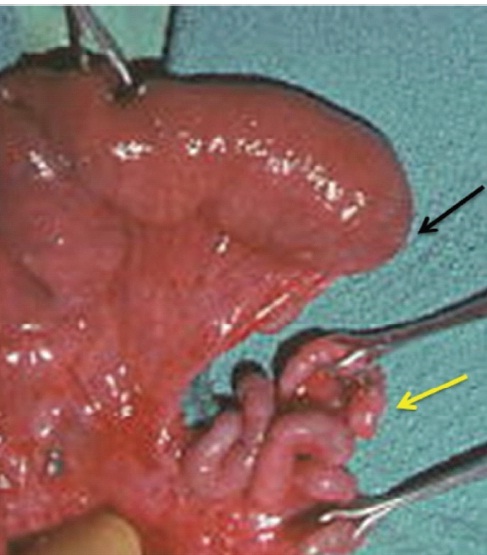
Exploratory laparotomy revealed dense inter-loop adhesions with foci of calcification on the small bowel serosa. Adhesiolysis revealed blind-ended, dilated proximal segment and collapsed distal segment of jejunum at approximately 30 cms from duedeno-jejunal flexure, with a V-shaped mesentery defect resembling a type III-a congenital jejunal atresia [Table/Fig-2]. Jejunal resection and end-to-end anastomosis was performed.
Laparotomy revealed blind-ended, dilated proximal segment (black arrow) and collapsed distal segment of jejunum (yellow arrow) at approximately 30 cms from duedeno-jejunal flexure, with a V-shaped mesentery defect resembling a type III-a congenital jejunal atresia
Histopathological examination revealed chronic inflammatory changes. Normal gastrointestinal motility was achieved in three days. The patient had an uneventful course and was discharged on the 8th postoperative day.
Discussion
Strictures and occasionally atresia of the bowel are known to occur in premature infants after recovery from necrotizing enterocolitis (NEC). This is particularly true in the segment of the intestine distal to an established enterostomy, most commonly the colon [1,2]. It is postulated that passage of stool through a partially damaged intestinal segment will render some protection against the development of strictures or atresia, whereas diversion of the fecal content will cause mucosal adherence and stricture or atresia formation [3].
Michaelis et al., reported a case of a 19-month-old boy in whom intestinal atresia developed after drainage of a large intra-abdominal abscess [4]. The proximal segment fistulized to the umbilicus which eventually healed without surgical intervention. Two months later at the time of surgical exploration, complete atresia with a V-shaped gap defect in the mesentery was noted. Sigge and Wurtenberge reported a 1430 gm premature infant in whom NEC developed in the 1st week of life and who 2 wk later was found to have a 7-mm mid-ileal atresia [5]. Jona described a similar case in a premature low-birth-weight neonate who developed ileal atresia as a sequel to NEC and intestinal continuity was established via an ileo-ileal fistula [3].
Acquired intestinal atresia in non–necrotizing enterocolitis affected patients is very rare. We could find only four case reports of acquired atresia of the small bowel in non-NEC patients in the English literature [6–9]. Puvabanditsin et al., reported a case of postnatal intususception that caused jejunal atresia in an infant born at 26 wk of gestation [6]. Elemen et al., reported acquired ileal atresia in a 2-year-old girl because of chronic entrapment of the ileal segment together with its mesentery by an adhesive band interrupting the blood supply resulting in a V-shaped mesenteric defect between the atreticsegments [7]. Osuoji et al., reported a case of acquired ileal atresia in a 4-month-old female infant who had an ileo-colic intussusception [8]. Ratan et al., described two patients, aged three months and our months, in whom episodes of diarrhea caused unusual acute development of atresia in the distal ileum after brief symptomatology of approximately 14 d. The authors proposed that a thromboembolic event affecting the blood supply to that segment may underlie intestinal stenosis or atresia presenting a few weeks after birth [9].
Conclusion
The acquired atresia in our patient may be because of chronic entrapment of the jejunal segment together with its mesentery by an adhesive band interrupting the blood supply resulting in a V-shaped mesenteric defect between the atretic segments. Local ischemia and ongoing inflammation with further resorption of the devitalized segment and subsequent healing were likely involved resulting in complete healing of the atretic ends. We speculate that the reason for adhesions and calcification would have been a healed intra-uterine meconium perforation.
This brief report suggests an adhesive band, which may entrap a jejunal orileal segment together with its mesentery, may be a potential cause for acquired small bowel atresia in non-NEC patients.
[1]. Mares AJ, Freud E, Efrati Y, Acquired colonic atresia: A rare sequel of necrotizing enterocolitisJ Pediatr Gastroenteral Nutr 1993 16:93-97. [Google Scholar]
[2]. Beardmore HE, Rodgers BM, Outerbridge E, Necrotizing enterocolitis (ischemic enteropathy) with the sequel of colonic atresiaGastroenterology 1978 74(914):9-17. [Google Scholar]
[3]. Jona JZ, Acquired ileal atresia and spontaneous reconstitution of intestinal continuity in a premature infant with necrotizing enterocolitisJ Pediatr Surg 2000 35:505-07. [Google Scholar]
[4]. Michaelis L, Shaw A, Alrich M, Acquired intestinal atresiaJ Pediatr Surg 1971 6:666 [Google Scholar]
[5]. Siegge W, Wurtenberger H, Atresia and obliteration of small bowel in cases of necrotizing enterocolitisZ Kinderchir 1981 32:104-11. [Google Scholar]
[6]. Puvabanditsin S, Garrow E, Samransamraujkit R, Postnatal Intussusception in a premature infant, causing jejunal atresiaJ Pediatr Surg 1996 31(5):711-12. [Google Scholar]
[7]. Elemen L, Tugay M, Erkus B, Acquired ileal atresia because of adhesive small bowel obstructionJ Pediatr Surg 2010 45:1383-85. [Google Scholar]
[8]. Osuoji R, Idika O, Odomeja E, Acquired ileal atresia complicating an ileocolic intussusception in a 4-month-old infantJ Pediatr Surg 2011 46:E13-14. [Google Scholar]
[9]. Ratan SK, Rattan KN, Mathur SK, Maheshwari J, Sehgal T, Acquired ileal atresia in infancy: report of two casesPediatr Surg Int 2005 21:305-07. [Google Scholar]