Biochemical and microbiological research has suggested that periodontal disease is the result of an interplay between bacterial activity and the host tissue [1]. The host response to gingival microorganisms is characterized in part by an influx of polymorphonuclear leukocytes or neutrophils (PMN) [2]. Periodontitis is a multifactorial disease, manifestation and progression of which is influenced by a wide variety of determinants, including social, behavioral, systemic, environmental and genetic risk factors [3].
Cigarette smoking is a well established risk factor for periodontitis and is associated with an increased risk for periodontal attachment loss and bone loss [4]. The biological plausibility of the increased periodontal disease severity and rate of progression associated with smoking has been hypothesized to be due to interactions among smoking, bacterial periodontal pathogens, and the host [5].
Exposure to environmental cigarette smoke is associated with increased leucocyte counts, chemotaxis an increased release of reactive oxidants from stimulated neutrophils. Smokers demonstrate 2.6 – 6 times increased prevalence of periodontal diseases compared to non-smokers [6]. Cigarette smoking also affects VB12 and FA mechanisms [7].
Smokeless tobacco has also been shown to affect the immune response both in vitro and in vivo [5]. Clinical attachment level (CAL), gingival recession, mobility, furcation and lesions like leukoplakia, periodontal disease, delayed wound healing and dental caries were significantly higher amongst smokeless tobacco users as compared to those not consuming smokeless tobacco [8]. Although available in many different forms, smokeless tobacco is mainly used as chewing tobacco and snuff (moist or dry) [9].
VB12 is a water-soluble, heat-sensitive vitamin of the B-vitamin group. It is often protein bound as methylcobalamin, hydroxycobalamin and deoxyadenosycobalamin in nutrients [7]. FA (also known as folate) is an essential vitamin, which is also heat sensitive and water soluble. It belongs to the class of vitamin compounds related to pteroylglutamic acid (PGA), which serve as cofactors in the enzymatic transfer of single carbon units in a variety of metabolic pathways [10]. Factors affecting VB12 and FA are listed in [Table/Fig-1].
Folate deficiency, which is associated with increased oxidative stress, endothelial dysfunction, genomic instability, defective DNA repair, and apoptosis, has been shown to be related to a number of human diseases, including periodontal disease [3]. Repair and maintenance of periodontal tissue requires high turnover of squamous epithelium which is impaired in cases of reduced levels of FA. Deficiency of FA is also known to cause necrosis of gingiva, periodontal ligament and loss of alveolar bone [10].
Cyanide, being one of the major component of cigarette smoke, adversely affects VB12 nutritional status [11]. Further tetrahydrofolic acid combines with cyanate to yield a biologically inactive compound [12] , which could result in folate deficiency in tissues affected by cigarette smoke. Organic nitrites also inactivate methyl cobalamin by cleaving the methyl–cobalamin bond [13].
The chemical carcinogens in smokeless tobacco include polynuclear aromatic hydrocarbons (usually benzo-a-pyrene), polonium-210, and N-nitrosamines. Other chemicals include radium-226 and lead-210 [14]. The primary periodontal alteration in smokeless tobacco users is localized gingival recession (25-30 %) [15].
Whereas the untoward effect of smoking on periodontal health is abundantly documented, little is known about the possible effects of non smoked tobacco products [9] and it’s effect on serum levels of VB12 and FA. To our knowledge from the indexed literature, no study has yet analysed the comparative evaluation of serum VB12 and FA concentrations in patients with chronic periodontitis who are Gutkha users.
Taking this into consideration, the present study was conducted to estimate and correlate the serum VB12 and FA levels among periodontally healthy (Group I),chronic periodontitis (Group II) subjects, smokers with CP (Group III) and gutkha chewers with CP (Group IV) and also to correlate the serum levels with clinical parameters which will be of great importance in the diagnostic and preventive strategy of periodontal diseases.
Materials and Methods
Study Design
In the present cross-sectional study, 120 systemically healthy subjects aged between 18 to 60 y were randomly selected from the out-patient department, Department of Oral medicine, P.M.N.M Dental College and Hospital, Bagalkot, India among which nine were excluded (four aggressive, three noncurrent smoker and two on steroid therapy for OSMF ). Further, all the participants were clearly explained regarding the need and design of the study. Written informed consent was obtained from all recruits. The research project was approved by the Ethical Committee.
The selection of patients was made according to the criteria approved by the 1999 International Workshop for the classification of periodontal diseases and conditions [16]. Further, in Department of Periodontics,111 Patients were divided into four groups as clinically healthy periodontium (Group I), chronic periodontitis (Group II), smokers with CP(Group III) & gutkha chewers with CP (Group IV).
All the study participants with no history of any acute/chronic systemic disorders were included. Subjects belonging to the group III were enrolled if they had smoked ≥100 cigarettes in their lifetime and currently smoked [17]. Gutkha chewers with chronic periodontitis (Group IV) were enrolled if they regularly chewed smokeless tobacco at least one sachet daily for atleast 12 months [18].
Pregnant women, lactating mother, individuals with trauma or who underwent recent tooth extraction or who had received any periodontal / antimicrobial and anti-inflammatory therapy or vitamin supplements in last three months before sampling were excluded from the study.
Periodontal parameters
Depending upon the GI, PPD and CAL measurements, study subjects were divided into 4 groups:
Group I (n= 30): Periodontally healthy subjects characterized by GI=0 (absence of clinical inflammation), PPD ≤ 3 mm and CAL=0,
Group II (n= 29): Subjects with CP characterized by at least 30% sites with PPD ≥ 5 mm, GI >1 and CAL ≥4 mm,
Group III (n=25): Smokers with CP and
Group IV (n=27): Gutkha chewers with CP.
One calibrated examiner obtained all the measurements so as to reduce intra-examiner variability for Gingival index (GI) [19], probing pocket depth (PPD) and clinical attachment level (CAL). Both PPD and CAL were recorded using the Williams graduated periodontal probe at four sites around all present teeth , excluding the third molars.
Serum sampling
Around 4 ml of blood was drawn between 08:30 and 11:00 am in fasting state, from the antecubital fossa by venipuncture using 20-gauge needle with a 5ml syringe. The blood sample was allowed to clot at room temperature, and, after one hour, serum was separated from blood by centrifuging at 3000-3500 rpm for five minutes. It was immediately transferred to a plastic vial and stored at -70oC until further examination was carried out [7, 20].
Spectrophotometric analysis
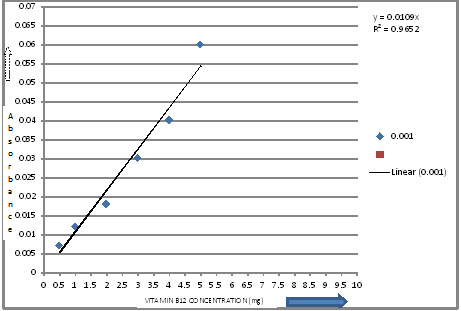
Standardization was done for getting calibration curve of FA and VB12 [Table/Fig-2&3]. For VB12 estimation, equal amount of the distilled water was added to the sample in a test tube, after which it was shaken for 30 min and then forcedly vibrated for 10 min. Later, samples were assessed by UV-Visible spectrophotometer (Shimadzu Model) set at 361 nm wavelength to calculate the values through absorbance [21,22].
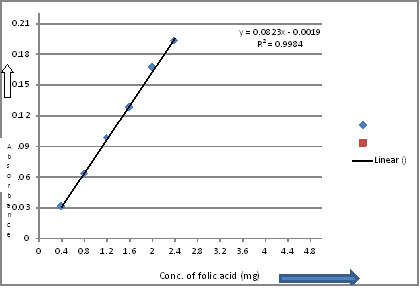
For FA determination in a sample, 20 tablets of FA (FOLVITE 5 mg) were weighed and grounded into fine powder. An amount of powder equivalent to 5 mg of FA was dissolved in 0.1 mol L-1 sodium hydroxide and diluted to 50 ml in volumetric flask. The dissolved solution of this drug was filtered through Whatman No.42 filter paper and diluted with 0.1 mol L-1 sodium hydroxide to the volume so as to obtain the appropriate concentration for analysis [23].
Afterwards, accurate volumes (1.0 mL) of standard or sample of FA were mixed with 1.0 mL of 4 mol L-1 hydrochloric acid, 1.0 mL of 1% (w/v) sodium nitrite, 1.0 mL of 1% (w/v) sulfamic acid and 1.0 mL of 1% (w/v) 3-aminophenol which resulted in an orange-yellow complex. The absorption of colour intensity was recorded at 460 nm against the corresponding reagent blank using UV-Visible spectrophotometer [23].
Statistical Analysis
The statistical analysis was performed using Statistical Package for Social Scientists (SPSS) software (version11). The results were presented as mean and standard deviation. Any differences between the four groups along with the clinical and serum variables, viz. GI, PPD,CAL,VB12 and FA were carried out through Pearson correlation coefficient test .The pair-wise differences among the four groups were carried through Mann-Whitney U-test and Kruskal Wallis test. The p-value i.e. p ≤ 0.5 was considered to be statistically significant.
Results
The present cross sectional study was carried out among 111 subjects and categorized into 4 groups based on their history and clinical presentation. Pairwise comparison of all the subjects revealed the absence of female subjects in Group III and Group IV and comparatively younger subjects in Group IV [Table/Fig-4]. The differences between the four groups were significant (p< 0.001) in terms of GI scores, PPD and CAL [Table/Fig-4]. The mean scores of all the parameters (GI, PPD, CAL) were significantly higher among Group II, III and IV compared to Group I (p < 0.001). Likewise, pairwise comparison of GI, PPD and CAL among four groups by Mann-Whitney U-test were highly significant (p<0.001). The mean GI score was statistically significant when Group II was compared with Group III (p< 0.004) [Table/Fig-5].
Study population data, periodontal and serum parameters (Mean±SD)
| Charact-eristics | Group I | Group II | Group III | Group IV | p-value |
|---|
| Age in yrs | 37 ± (5.1) | 41 ± (4.9) | 54 ± (5.6) | 32.5 ± (4.2) | |
| Male or Female% | 80 /20 | 70/30 | 100 /0 | 100/0 | |
| GI Score | 0.23 ± (0.1) | 1.86 ± (0.45) | 0.63 ± (.13) | 1.83 ± (0.51) | <0.001* |
| PPD(mm) | 0 | 5.53 ± (1.23) | 5.4 ± (.62) | 5.2 ± (1.23) | <0.001* |
| CAL (mm) | 0 | 6.13 ± (0.25) | 5.9 ± (1.17) | 6.03 ± (.15) | <0.001* |
| VB12 (mg/ml) | 83.91± (37.82) | 90.91 ± (35.63) | 105.46 ± (59.73) | 120.74 ± (51.32) | |
| FA (mg/ml) | 9.63 ±(4.45) | 9.51 ± (3.05) | 7.61 ± (3.94) | 8.64 ± (3.62) | |
GI,gingival index; PPD, pocket probing depth; C A L, clinical attachment level;, VB12 ; vitamin B 12, FA, folic acid; * Statistically significant; p< 0.001-***, p<0.01- **, p<0.05-*
Pair wise comparison of GI among four groups by Mann-Whitney U test
| Group I vs II/III/IV | p< 0. 001* |
| Group II vs III/IV | p< 0.004 / .001* |
| Group III vs IV | p< 0. 001* |
* Statistically Significant When; P< 0.001-***, p<0.01- **, p<0.05-* ; GI,gingival index
Upon pairwise comparison of four Groups, significant difference in mean VB12 levels were found between Group I and Group IV (p= 0.01) and Group II and Group IV (p = 0.01) [Table/Fig-6]. The VB12 values were significantly higher in group IV as compared to other groups. Likewise, significant difference in mean levels of FA was found between Group I and Group III. (p = 0.046) and Group II and Group III (p=0.009) suggesting it’s concentration being lower in smokers [Table/Fig-6]. According to Pearson correlation method, serum VB12 & FA levels are directly proportional to each other in Group I and Group II where as inversely proportional in Group III and IV [Table/Fig-7].
Pairwise comparison of four groups with VB12 and FA levels by Mann-Whitney U-Test
| Groups | | Other groups | VB12 | FA |
|---|
| Group I | v/s | Group II | p=0.37 | p=0.728 |
| | Group III | p=0.096 | p=0.046* |
| | Group IV | p=0.01** | p=0.515 |
| Group II | v/s | Group III | p=0.425 | p=0.009** |
| | Group IV | p=0.01** | p=0.198 |
| Group III | v/s | Group IV | p=0.069 | p=0.124 |
p-value is significant in : Group I/II v/s Group IV for VB12 and Group III v/s Group I/II for FA; VB12,vitamin B-12; FA, folic acid Statistically Significant when p< 0.001***, p<0.01 **, p<0.05*
Group correlation coefficient between VITAMIN B 12 , FOLIC ACID, GI , CAL and PPD.
| Groups and Parameters | Group I VB12 | Group II VB12 | Group III VB12 | Group IV VB12 | Group I FA | Group II FA | Group III FA | Group IV FA |
|---|
| GI | r | 0.066 | 0.185 | 0.297 | -0.303 | 0.062 | -0.003 | 0.313 | -0.053 |
| P | 0.728 | 0.327 | 0.011* | 0.104 | 0.746 | 0.986 | 0.042* | 0.020* |
| PPD | r | 0.125 | 0.068 | -0.003 | 0.265 | -0.227 | -0.226 | -0.171 | 0.028 |
| P | 0.511 | 0.841 | 0.985 | 0.047* | 0.27 | 0.891 | 0.037* | 0.884 |
| CAL | r | 0.016 | 0.098 | -0.047 | -0.248 | -0.103 | -0.106 | -0.207 | 0.082 |
| P | 0.935 | 0.605 | 0.804 | 0.187 | 0.587 | 0.578 | 0.272 | 0.668 |
GI,gingival index; PPD, pocket probing depth ; CAL , clinical attachment level ; VB12 , vitamin B-12; FA , folic acid; r = value of correlation statistically Significant when p< 0.001***, p<0.01 **, p<0.05*
Correlation between GI , PPD , Vitamin B12 and Folic Acid
In group I, the r-value of GI in relation to FA and VB12 is positively correlated (r <0.066) and (0.062). However, when seen statistically, results are insignificant. In group III, GI is positively and significantly correlated with FA and VB12 i.e. if GI increases, FA and VB12 will increase. In group IV, GI is negatively correlated with FA and VB12 but p<0.05 in relation to FA. In group III, PPD is negatively correlated and P-value is significant (p = 0.037) in relation to FA. When comparing PPD with VB12, it is found significant (p=0.047) in group IV [Table/Fig-8].
Pearson co-relation between VB12 and FA groups, (-) showing negative co-relation
| Group I | .074 |
| Group II | .070 |
| Group III | -.029 |
| Group IV | -.192 |
Discussion
Smoking and smokeless tobacco have shown to impair various aspects of innate and immune host responses. The habit of chewing tobacco is increasing because of its free availability and cheaper cost and ban on smoking at public places in India. Adults currently using smokeless tobacco are twice as likely to have severe active periodontal disease than adults who never used smokeless tobacco [5]. Although there is wide documentation of the adverse effects of cigarette smoking on periodontal disease, vitamin B12 and folic acid but the effects of gutkha on concentrations of water soluble vitamins is less well studied.
Cobalamin is released from intrinsic factor cobalamin complex and binds either to transcobalamin (T C II) or serum haptocorrins. TC II accounts for 10- 30 % of the measurable serum cobalamin level. After absorbtion of folate in jejunum, the principal storage site is the liver. Distribution of folate to other tissues depends mostly on enterohepatic recirculation, in which folate in a methylated form is re-absorbed from bile into the serum [24]. Folic acid works with vitamin B12 in many functional processes throughout the body, including the periodontium [7].
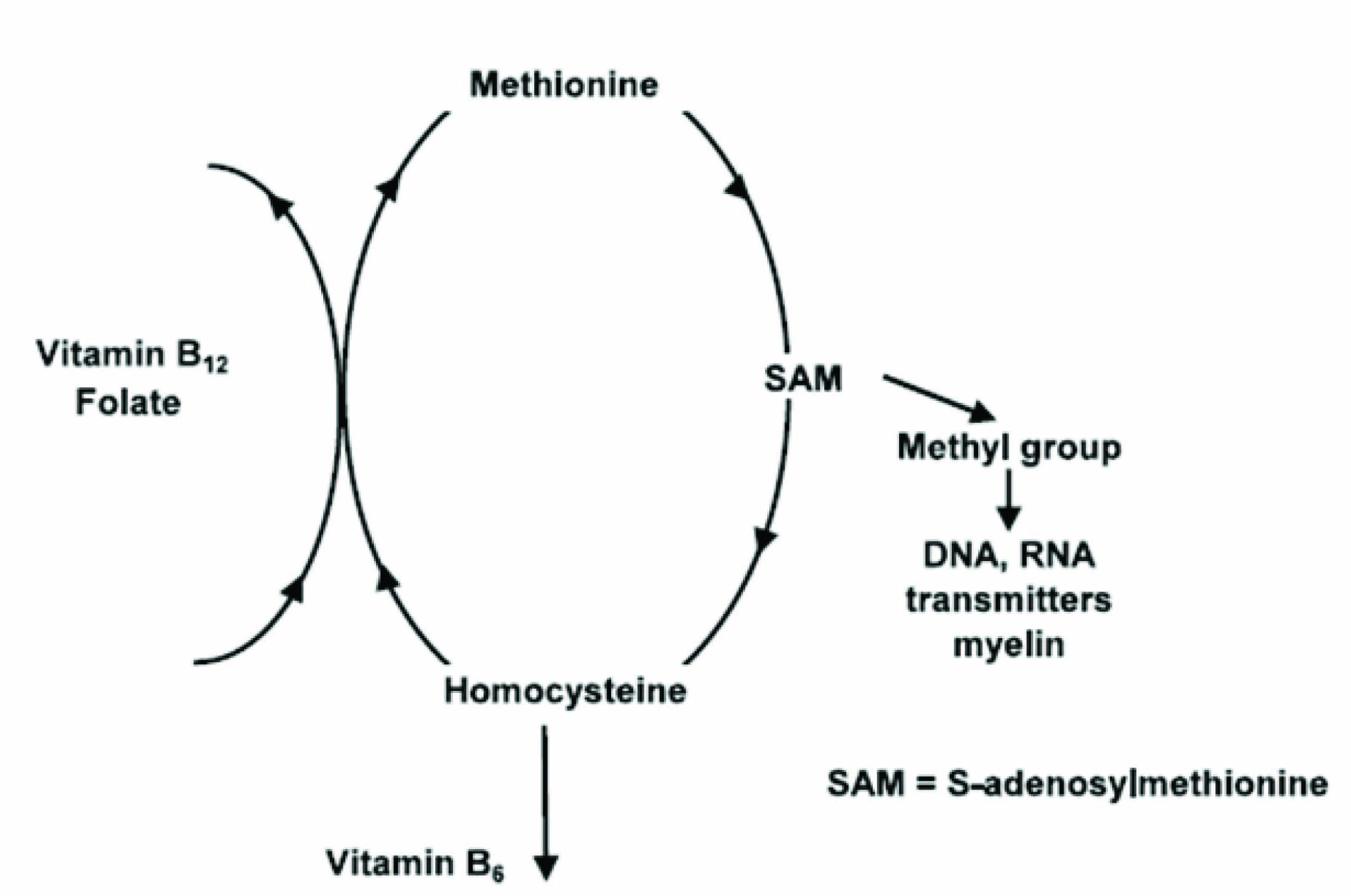
Methylcobalamin is essential for the removal of the methyl group from 5-methyl tetrahydrofolate in the homocysteine - methionine transmethylation catalyzed by methionine synthase [Table/Fig-9]. As a consequence, vitamin Bl2 deficiency or inactivation results in most of the folates being ‘trapped’ in a form (5-methyl tetrahydrofolate) that cannot be utilized. Folate deficiency secondary to the “methyl folate trap” could therefore develop in the vitamin B- 12 depleted tissues [11].
Interaction between folate, vitamin-b12 and homocysteine
Interestingly, the results suggested that VB12 levels were highest in Group IV as compared to other groups while FA levels were found to be decreased in Group III and Group IV when compared to healthy and CP groups. In group IV, there is also a risk of lesions like oral submucous fibrosis that causes restricted mouth opening in later stages and which can be a reason of less intake of fruits and vegatables leading to decreased levels of folic acid as compared to group I and group II . The serum folic acid levels of smokers was less in comparison with that of healthy subjects which is in accordance with several previous studies [11,25,26].
Via chemical inactivation , exposure to cigarette smoke may result in folic acid deficiency that principally affects the bronchial epithelium, rendering it more susceptible to neoplastic transformation by the carcinogenic hydrocarbons of tobacco smoke [26].
Smoking stimulates the oxidative burst of neutrophils, increases reactive oxygen species production and leads to lipid peroxidation and alterations in protein carbonyls in plasma [4]. Erdemir EO and Bergstro J have investigated the relationship between smoking and the serum levels of FA, VB12 in patients with periodontal disease. The serum FA concentration of smokers was lower than that of non-smokers (p < .05) whereas serum VB12 concentrations did not significantly differ between the two groups [7].
Rungsunn et al., have reported that the serum FA of smokers was lower than that of nonsmokers which was not significantly different and serum VB12 levels were significantly higher in smokers than the non-smokers which supports the results of our study [26].
It has been recognised that smoking affects the nutritional status of FA, VB12 and vitamin B6 [7,10,27] each of which regulates homocysteine metabolism [28]. Alternatively, it may be because cigarette smokers have poorer diets than non-smokers. The connection between smoking and dietary intake is extremely complex. Smokers ate more white bread, sugar, cooked meat dishes, butter and whole milk and less wholemeal bread, high-fiber breakfast cereals, fruits and carrots [29]. The dietary habits of smokers are characterized by higher intakes of energy, total fat, saturated fat, cholesterol and alcohol and by lower intakes of antioxidant vitamins and fiber, compared with non-smokers [30]. However, this result is not in accordance with the results of a study by Pagan et al., who found serum vitamin B12 concentrations to be significant lower in smokers than in non-smokers [31].
Nicotine, the most characteristic of tobacco components, is a highly toxic alkaloid that is both a ganglionic stimulant and a depressant. Many of its complex effects are mediated by the release of catecholamines. Tobacco smoke exposure is associated with a marked reduction in monoamine oxidase, an enzyme that is associated with mood function. It is conceivable that such effects result in dysregulation of appetite or attitudes toward food. Others have suggested that modifications of taste related to smoking may lead smokers to prefer certain foods [30].
It was observed that there was no significant correlation between VB12 and FA with age, CAL in any of the groups when seen group wise. Although , there exists significant correlation between vitamin B12 , folic acid PPD, and GI if one ignores the other groups [Table/Fig-8].
The result obtained in this current study demonstrates that the highest value of serum VB12 is found in gutkha group. This may be attributed to the fact that gutkha chewers have altered taste sensation, eat more of sweet and salty foods which could lead to elevation in amount of VB12. There are several causes of inadequate serum levels of VB12 and FA, the binding proteins of the vitamins may be falsely high or low, the distribution to the cell may be disturbed and enzymatic defects may demand higher vitamin levels. Serum levels may be considered specific, however non-sensitive [32].
The most salient finding of our study is that the serum VB12 and FA levels were higher in Group IV as compared to Group III. This observation may be related to the actual physical location of the ST on the external tissue surface, the differences in tissue characteristics, or the greater surface area of alveolar mucosa in contact with the tobacco. The findings of our study suggest that both periodontitis and smokeless tobacco chewing lead to significant changes in VB12 and FA in serum.
Oral conditions, such as periodontal infections, may be risk factors or indicators for important medical outcomes represents a paradigm shift in thinking about causality and the directionality of oral and systemic associations [33].
Conclusion
Among the risk factors, smoking and chewing tobacco are the most prevalent ones which are also the most common oral abusive habits in today’s life style. Our study provides evidence that gutkha being one of the causative factors for periodontitis, indeed showed difference in serum levels of VB12 and FA, contributing to the inflammatory burden on periodontium. We suggest that higher VB12 and lower FA levels reflect increased periodontal inflammation.
However, the present study suggests that the impact of quantified tobacco use on periodontitis in small population may be limited to the importance of serum VB12 and FA levels and, the cardinal role of oral hygiene as one of the aetiology of periodontal disease should also be assessed.
Special educative methods should be designed depicting the role of gutkha on systemic health other than oral cancer. Further intervention with expanded study sample including other fluids is acceptable to be more specific towards the effect of gutkha which can set these two vitamins as biomarkers for oral health in future. It becomes important to consider gutkha chewing which can be as harmful as smoking for periodontitis.
GI,gingival index; PPD, pocket probing depth; C A L, clinical attachment level;, VB12 ; vitamin B 12, FA, folic acid; * Statistically significant; p< 0.001-***, p<0.01- **, p<0.05-*
* Statistically Significant When; P< 0.001-***, p<0.01- **, p<0.05-* ; GI,gingival index
p-value is significant in : Group I/II v/s Group IV for VB12 and Group III v/s Group I/II for FA; VB12,vitamin B-12; FA, folic acid Statistically Significant when p< 0.001***, p<0.01 **, p<0.05*
GI,gingival index; PPD, pocket probing depth ; CAL , clinical attachment level ; VB12 , vitamin B-12; FA , folic acid; r = value of correlation statistically Significant when p< 0.001***, p<0.01 **, p<0.05*