The aims and objectives of Orthodontic treatment are aesthetics, stability and function. Successful treatment requires a great deal of diagnostic skills and precise execution of therapeutic methods. The main reason for seeking orthodontic treatment for Class-II malocclusions is aesthetic improvement. If the malocclusion is skeletal in origin treatment options change according to patient’s age. Growth modification treatment procedures offer better results for a patient with significant potential growth [1].
The rationale behind functional appliance therapy is to improve functional relationships of dentofacial structures by eliminating unfavourable developmental factors and improve the muscle environment enveloping the dentition. The origin of functional appliance therapy goes way back to early 1900 s or late 1800 s. Robin’s monoblock was considered the forerunner of all forms of functional appliance therapy and Andresen’s Activator was considered to be the first functional appliance. Modifications of Activator and a variety of new appliance systems were introduced [2].
The total treatment outcome in any form of functional appliance therapy is a combination of skeletal and dental changes making a Class - II occlusion to Class - I occlusion. However, very limited methods and studies available to quantify skeletal and dental effects separately to assess treatment results in patients with decelarating phase of the growth. The S-O ( saggital occlusal ) analysis by Pancherz was chosen to evaluate skeletal and dental effects contributing to the responses with Twin block therapy.
Materials and Methods
The present study was undertaken in Division of Orthodontics and Dentofacial Orthopedics, Rajah Muthiah Dental College & Hospital, Annamalai University, Chidambaram, Tamilnadu, India. Strict diagnostic protocol viz. growing individuals with horizontal growth pattern, skeletal class II due to retrognathic mandible with positive VTO, bilateral class II molar relation, minimal or no crowding in either arch and overjet more than 5 mm was used for case selection. The growth status was assessed on Lateral cephalograms using cervical vertebrae and later confirmed by Hand wrist radiographs. Initially Skeletal maturation evaluation was done using cervical vertebrae (CVMI) [4,5]. Patients in the stages of CVMI- III (transition) and CVMI- IV (Deceleration) were selected for the study. Among these selected patients, again those with MP3-H stage on Hand wrist radiographs were chosen [5]. The patients in permanent dentition period with all the second molars erupted were included in the study. The cephalometric criteria included Normal SNA angle of 80-82 degrees, reduced SNB angle of less than 78 degrees indicating mandibular retrognathism. The patients with average FMA angle of 25-30 degrees were included in the study. The other cephalometric parameters which fit the case for a class II skeletal correction by way of functional appliance such as saddle angle less than 130 degrees, articular angle greater than 143 degrees, Lower gonial angles less than 60 degrees were set for the sample. The sum of the saddle angle, articular angle and gonial angle should not exceed 360 degrees.
The exclusion criteria are (1) Patients with syndromic malocclusions. (2) Patients with systemic diseases. (3) Patients with abnormal vertical and Transverse growth pattern. Appropriate records – photographs study models, lateral cephalogram, OPG, Hand– wrist X-rays were taken [Table/Fig-1a,b,c]. Out of 28 selected cases, 17 patients received Twin Block (TB) therapy and 11 patients were maintained as control group. The control group comprised of cases that are willing to postpone the treatment due to personal reasons and was kept under observation until the end of the study. Two cases from treatment group did not wear the appliance as instructed and were excluded from the study. So, totally 15 cases which received treatment comprised the treatment group.
Pre treatment extra oral photographs

Pre treatment intra oral photographs

Pre treatment lateral cephalogram,
Standard removable TB appliances with lower incisor capping were delivered to treatment group [Table/Fig-2]. The horizontal advancement was about 8 mm and 2-3 mm vertical opening between the upper and lower central incisors were maintained for all the cases. The patients were instructed to wear the appliance 24h/d except while performing oral hygiene procedures.
Patient with twin block appliance during treatment

All of the subjects were followed every four week interval until the end of active appliance therapy. Appliance use was discontinued when overjet and overbite were reduced to 1-3 mm. Duration of appliance therapy varied from 8-13 month depending on the level of patient cooperation. The mean time interval between the initial (T1) and post treatment (T2) cephalograms of Twin-Block group was 11 month, with a range of 8 month to 13 month. In the control group, the mean time interval between the first (C1) and second (C2) cephalometric films was 12 month, with a range of 10 month to 14 month [Table/Fig-3a,b,c]. For each subject, lateral cephalograms were taken using a cephalostat (Panmeca Proline 2002cc, Finland) and radiographic film (Kodak X o mat China) of size 8 x 10 inches. The exposure parameters were 72 Kvp, 10 mA and 1.2 sec and the source to mid-sagital plane distance was maintained at 60 inches. All lateral cephalometric films were traced on a transparent cellulose acetate sheet of 0.076 mm thickness by the same operator. The T1 and T2 cephalograms were traced and Pancherz S-O analysis was used to segregate dental and skeletal effects [6,7].
post treatment extra oral photographs

Post treatment intra oral photographs

Post treatment lateral cephalogram

The SO ( Saggital occlusal) – Analysis (Pancherz 1982)
The SO-Analysis [Table/Fig-4] was excellent in predicting the alterations in sagittal occlusion (overjet, molar relationship) between skeletal and dental components in the maxilla and mandible [6,7]. This analysis have a reference grid comprising an occlusal reference line (RL) and a line perpendicular to that through sella (RLp) is defined on the first head film and then transferred to the after treatment head films by superimposition of the films on the nasion-sella line (NSL) with sella as a common registration point. All measurements were done parallel to RL.
Diagram showing the sagittal analysis( so) of Pancharz
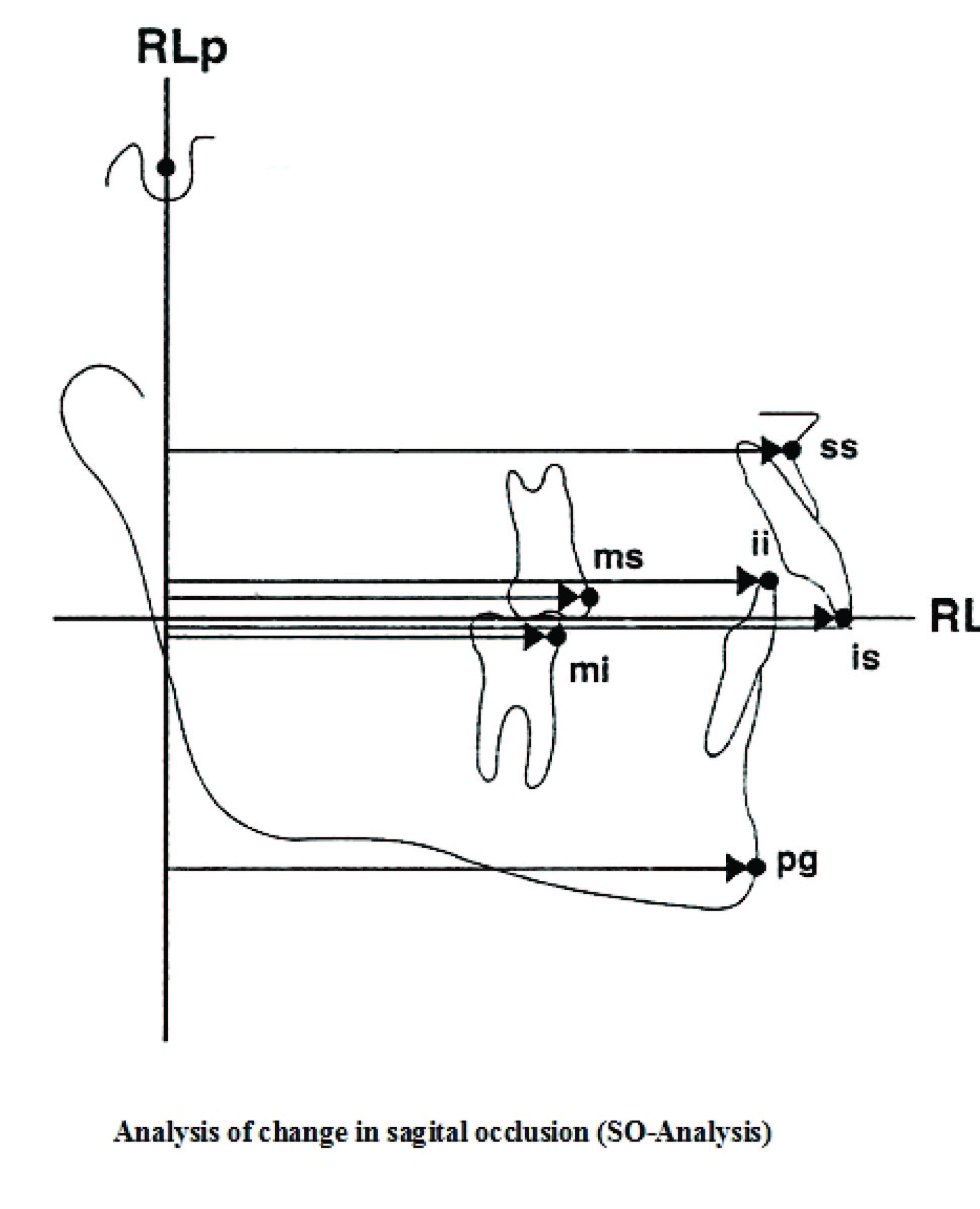
is/RLp minus ii/RLp – Overjet.
ms/RLp minus mi/RLp – Molar relation (a positive value indicates a distal relation; a negative value indicates a normal relation).
ss/RLp – Position of the maxillary jaw base.
pg/RLp – Position of the mandibular jaw base.
is/RLp – Position of the maxillary central incisor.
ii/RLp – Position of the mandibular central incisor.
ms/RLp – Position of the maxillary permanent first molar.
mi/RLp – Position of the mandibular permanent first molar.
Changes in the different measuring points in relation to RLp occurring during the examination period were registered by calculating the difference (d) in landmark position. Changes in variables 3 and 4 represent skeletal changes, while changes in variables 5 to 8 represent a composite picture of skeletal and dental changes. Variables for dental changes within the maxilla and mandible were obtained by the following calculations (variables 9 to 12)
is/RLp(d) minus ss/RLp(d) – Change in position of the maxillary central incisor within the maxilla.
ii/RLp(d) minus pg/RLp(d) – Change in position of the mandibular central incisor within in mandible.
ms/RLp(d) minus sp/RLp(d) – Change in position of the maxillary permanent first molar within the maxilla.
mi/RLp(d) minus pg/RLp(d) – Change in position of the mandibular permanent first molar within the mandible.
Results
The results obtained from pretreatment and post treatment cephalometric findings is Tabulated [Table/Fig-5]. The Cephalometric variables were imported to SPSS software for statistical analysis. Students Paired t-test was carried out to check any significant variations exists between pretreatment and post treatment levels. The test has been carried out at 5% level of significance. If the p<0.05, then it was considered that the change is significant. Significance was determined at the 0.05 (* significant), 0.01 (**very significant), and 0.001 (***Highly significant) levels of confidence. A test for normality of the observations for the cephalometric variables resulted in the following conclusions. Overjet decreased by 6.54±1.12mm, which was statistically significant. Molar relation showed 4.62±1.18 mm distally which was also highly statistically significant. Mandibular base moved 4.88±3.15mm mesially, which was statistically significant. Maxillary base moved 0.674±1.56mm distally, which was statistically significant. Maxillary central incisor moved distally within the maxilla by 0.866±1.125mm, which was statistically significant. At the same time the Mandibular central incisor moved mesially with in the mandible by 1.40±1.638mm, which was statistically significant. Thus the reduction of overjet is brought about by the movement of the both Upper and lower incisors. Maxillary First molar moved distally within the maxilla by 0.133±1.245mm, which was statistically significant. Mandibular first molar moved mesially with in the mandible by 0.666±1.496mm, which was statistically significant.
Comparison of Pre-treatment Twin Block and Post-treatment Twin Block (SO-Analysis)
| Variables Linear Measurements | Pre-treatment Twin Block (T1) | Post treatment Twin Block (T2) | p-value |
|---|
| Mean | S.D | Mean | S.D |
|---|
| Maxillary Base (ss/RLp) | 78.46 | 3.35 | 77.78 | 3.47 | 0.022* |
| Mandibular Base (pg/RLp) | 75.60 | 3.04 | 80.48 | 3.27 | 0.000*** |
| Maxillary incisor (is/RLp) | 87.33 | 3.99 | 86.73 | 4.02 | 0.054* |
| Mandibular incisor (ii/RLp) | 78.46 | 4.34 | 85.40 | 4.28 | 0.012** |
| Maxillary Molar (ms/RLp) | 54.62 | 3.77 | 54.20 | 3.62 | 0.055* |
| Mandibular molar (mi/RLp) | 52.40 | 4.23 | 56.60 | 3.95 | 0.014** |
| Overjet | 8.74 | 0.88 | 2.20 | 0.77 | 0.000*** |
| Molar relation | 2.22 | 1.18 | -2.40 | 1.18 | 0.000*** |
(*) significant, (**) highly significant, (***) very highly significant
Discussion
The concept of functional jaw orthopedics, especially functional appliance treatment philosophy evolved from animal studies. Several animal studies have suggested that protracting the mandible in young animals can stimulate mandibular condylar cartilage growth, producing significant changes in mandibular morphologic features as well as major occlusal changes [8]. Thus, growth modification can be accomplished in a matter of weeks for animals wearing mandibular protraction devices. In contrast similar growth changes in humans require months. Accepting these limitations many orthodontists use functional appliances in the hope of correcting class II skeletal malocclusion by enhancing mandibular growth.
The Twin Blocks have been described by patients as the most comfortable of all the functional appliances. As a result of altered muscle balance and continuous wear, significant changes in facial appearance are seen within 2 or 3 months of starting treatment with Twin Blocks which encourage good patient motivation. Rapid soft tissue adaptation occurs in response to an improved occlusal relationship. The patients included in this study were 10-14 y of age and the active treatment period was carried out as recommended by Clark [9].
Skeletal Changes
In this study, the mean movement of maxilla was 0.67mm which represents significant restriction of forward maxillary growth in contrast to control groups. Thus twin block can restrain maxillary growth to certain extent and suggest that a factor contributory to Class II skeletal correction [Table/Fig-6,7,8].
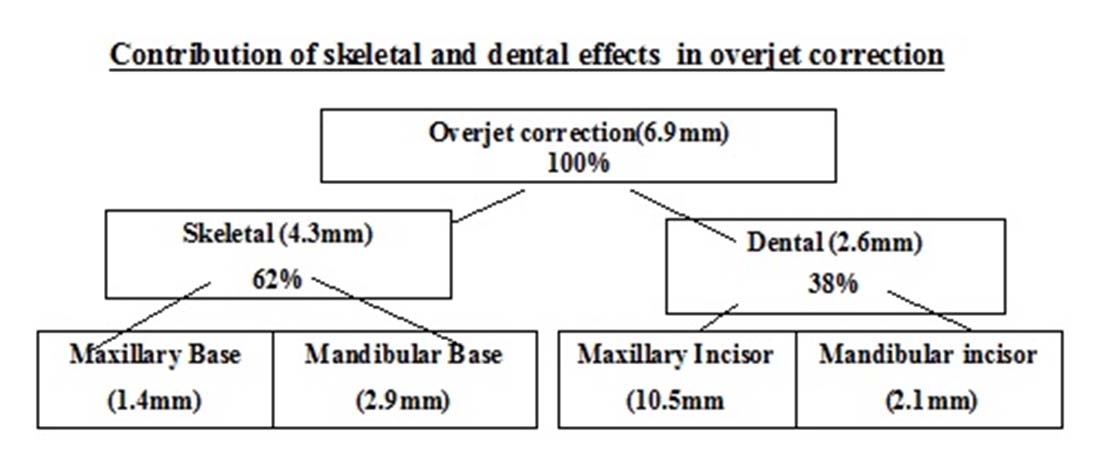
Skeletal and dental changes in reduction of overjet
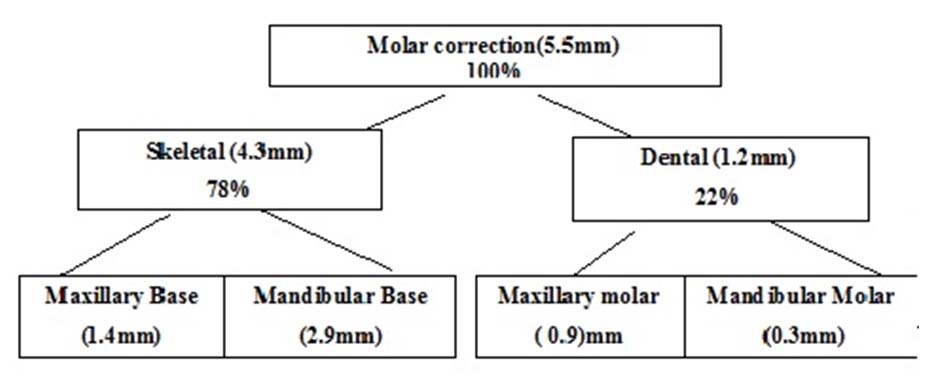
skeletal and dental changes in molar correction
cephalometric tracing of pretreatment, posttreatment and superimposition to show dental and skeletal effects

The role of functional appliances in increase in size of the mandible or acceleration of growth is a controversial issue. This study showed an increase in mandible length by 4.88mm. It suggests a significant growth of mandible in forward direction and contribute to the correction of Class II malocclusion. As comparable with other studies by Christine and Kara [4], David and Paul [10], SAbbie and James [11], this study also showed the head gear effect on maxilla and increased mandibular growth with Twin block therapy.
Dental Changes
The dental changes in our cases indicated a more forward movement of mandibular molars.
In this study the maxillary molars appear to move distally with a mean value of 0.13mm. Comparing this to the movement of maxillary jaw base itself, maxillary distal movement of molar is less. But still it contributes to Class II correction. While considering mandibular first molar, it moves mesially about 0.67mm within its jaw base. Since the entire jaw base moves mesially in a major extent the contribution from mesial molar movement is far less towards Class II correction [Table/Fig-6–8].
Regarding anterior teeth maxillary incisors move distally about 0.87mm which contribute to overjet reduction to a lesser extent. The mandibular incisors move 1.40mm mesially and contribute more for ovejet reduction which is comparable to studies conducted by Kevin and Jean [12] and Tiziano and Lorenzo [13] It suggests that even with incisor capping incorporated to Twin block design lower incisor proclination is inevitable in functional appliance therapy.
By comparison, the average total molar correction and the overjet correction in the treated group was about 5.5 mm and 6.9 mm respectively which was a highly significant difference from the controls. This correction was the combination of both the skeletal and dental movements. About 62% overjet correction is by skeletal responses and 38% by dental responses. The skeletal responses occurred almost exclusively in the mandible-42%. It correlates with the findings with the that of Tiziano and Lorenzo [13] and Kevin and Jean [14]. The skeletal and dental effects of Twin block therapy on Indian population were done by Sharma et al., [15]. The subjects selected in that study are all in mixed dentition period with active growth potential. The findings of our study also correlated with their findings but the skeletal effects are less pronounced and dental effects are more pronounced in our study.
Conclusion
The following conclusions were drawn from the study-
Twin Block showed highly significant anterior movement of the skeletal pogonion and significant increase in mandibular length resulting in reduction in facial convexity.
The SNA value decreased marginally in the Twin Block suggesting a restraining effect in the maxilla by the Twin Block appliance.
The dental changes observed were retroclination of the maxillary incisors and proclination of the mandibular incisors resulting in a reduction in the overjet.
Mesial movement of the mandibular Ist molar and slight distal movement of the maxillary Ist molar were noticed.
The favourable occlusal changes for both reduction in the overjet and molar correction were mainly due to skeletal modifications occurring almost exclusively in the mandible.
(*) significant, (**) highly significant, (***) very highly significant