Prosthetic rehabilitation of a severely atrophic maxilla poses a challenging therapeutic problem, because bone augmentation is required to enable placement and ensure stability of a sufficient number and length of implants [1].
This area of the posterolateral maxilla presents a sort of low-quality bone tissue which makes it an inappropriate site for dental implantation. Bone from this area is typically classified as type IV (poor quality) on the classification scale devised by Lekholm and Zarb. Implantation in this region calls for the surgical technique of maxillary sinus lifting, through which bone grafts are inserted in order to permit immediate or future implant installation. These procedures are usually followed by the placement of endosseous dental implants. This is done either simultaneously or after allowing time for consolidation of the grafted material [2]. Numerous clinical studies have reported excellent prognosis for dental implants placed in augmented sites [3].
Autogenous bone grafts, allograft, alloplast, and xenografts are used for the purpose of bone grafting in this region. Autogenous grafts are considered the golden standard in terms of osteogenic potential, but they present with disadvantages as they are harvested from the patient [4]. Many bone substitutes have been tried in the search for an acceptable alternative to autografts, but even the best among them are only osteoconductive materials (hydroxyapatite, allografts, xenografts, and alloplastic materials). These materials have been applied in sinus augmentation procedures, since they are readily available in the needed quantity and maintain the original volume during healing [5]. An-organic bovine bone is a xenograft which has a chemical composition and architectural geometry similar to that of human bone and can support new bone formation in direct contact to the graft. An-organic bovine bone is regarded to be an osteocompatible grafting material that may serve the purpose of space provision or possibly as a bone promoting substance [6]. An ideal, a bone grafting material should be biocompatible, allowing formation of new bone or bone substitution through the process of osteoconduction and should provide significant structural integrity. Through our study we reported on the bone forming potential of this material in human subjects.
Cone-beam computed tomography has to be considered as a giant leap forward with regards to the field of dental radiology. Cone beam computed tomography provides us a medium through which we can evaluate this new bone in all three dimensions without any invasive procedure using a considerable low radiation dose [7]. Although, there exist studies that report on the density of the existing alveolar bone [8], but they have utilized conventional CT with a much higher radian dose [9].
Materials and Methods
Our study consisted of a total of 19 subjects with the mean age of 51±4.70. There were 11 male and 8 female patients. Mean age of male patients was 49±3.43. And the mean age for female patients was 54±5.34. All patients had undergone a maxillary sinus augmentation procedure carried out with immediate placement of dental implants in the region of the augmented sinus at Hospital Universiti Sains Malaysia. All subjects were indicated for dental implants and each patient had a missing tooth in the posterior maxillary region with a bone height of less than 5mm. A total of 19 implants were placed in our region of interest in the posterior maxilla with one implant per patient. All implants had a uniform length of 10 mm.
Surgical Protocol for Sinus augmentation and implant placement
A Single/1- stage surgical protocol was carried out in which the implant placement was done in conjunction with the maxillary sinus augmentation [10]. The surgical stage and the second stage prosthetic protocols were standardized for each patient.
After a graft maturation period of 6mnths the implant was loaded with the prosthesis. One year after loading the patient was called up for a follow up scan. All implants were clinically successful based on the criteria of implant success proposed by [11], all our implants were clinically osseointegrated, non mobile, dull sounding to percussion, asymptomatic and did not exhibit any radiolocency around them.
Follow up Scan
Follow up CT scans using PlanmecaPromax 3D® (Planmeca Oy, Finland) were taken 18 months after placement of the dental implant housed in the grafted region. The scanning conditions were: tube voltage 84kV, tube current 12 mA, and slice thickness 1 mm. CT images were stored in DICOM format.
Data Analysis
Patient scans were analysed using the Cone Beam CT machines computer based software; PlanmecaRomexis” Imaging Software 2.2® by which the data is analysed in all three dimensions. The scans are analysed in the 3D X-ray volume view mode.
Pre-measurement preparations included a 30 min warm-up time for the liquid crystal display (LCD) screen to attain its maximum performance, room lighting control to eliminate reflections on the screen having comfortable seat in place for the examiners (Practice guideline for digital radiography, The American College of Radiology 2007).
The implant was divided into 2 parts of 5 mm each using the length measurement tool of the software by drawing a 10 mm line from neck of the implant embedded the alveolar bone towards the apical end of the implant embedded in the grafted region. Hence, the measurement above 5mm of the embedded implant apically (towards the maxillary sinus) is considered to be bone formed as a result of osteoconduction by the graft and was termed as the grafted region. The region below the 5mm of the implant coronally (Towards the neck of the implant/towards the prosthesis) is termed as the existing alveolar bone underneath the grafted region. In the grafted region and in the existing alveolar bone region, radiographic measurements were taken at three different points per implant with four readings per point making a total of 12 readings per subject.
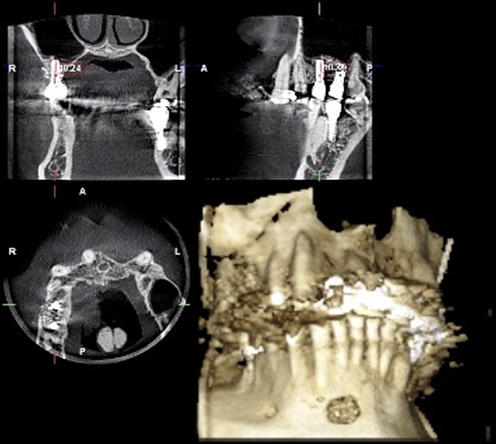
To standardise the cut on which every time the measurement is taken on different subjects, a set of steps are to be made for each implant in every case. The axial view is set to the level where all implants are seen, the coronal and the sagittal reference lines are adjusted to intersect at the center of the implant to be measured. The implant then is adjusted by rotation of the view in order to obtain an image of the implant of its long axis parallel to sagittal and coronal reference lines in coronal and sagittal views respectively. In the coronal and sagittal using the length measurement tool in the software a 10 mm tangential line is drawn along the long axis of the implant. In the coronal and sagittal views the axial line is set at the three levels (10, 9 & 8 mm for the grafted region and 4, 3 & 2 mm for the region of the existing alveolar bone) where measurements are to be taken around the implant. The bone density was measured in Hounsfield unit displayed on the screen was made using the automatic option for density measurement incorporated in the software. The bone densities at the buccal and palatal bone surfaces are measured on the coronal view screen. While the bone densities at the mesial and distal surfaces are measured on the sagittal view screen as shown in [Table/Fig-1].
Measurement using 3D explorer option of Planmeca Romexis® software
Statistical Analysis
For statistical analysis the latest version of IBM® SPSS® 20 was used. Data was normally distributed as checked by histogram. Data are presented as Mean ± standard deviation (SD). All the recorded density readings were in Hounsfield units. Comparisons between the density existing alveolar bone and density of the bone formed by the graft in the region of interest were made with the t-test.
Results and Findings
The mean bone density of the grafted region for each subject showed the density values in the range of 600 HU to 900 HU. The highest mean bone density was 832± 169.73 HU whereas the lowest bone density was 605± 226.76 HU shown in [Table/Fig-2].
Mean Bone density of the grafted region for each subject in Hounsfield Unit (HU)
| Patient | Mean (HU) SD |
|---|
| 1 | 648 ± 128.43 |
| 2 | 680 ± 241.23 |
| 3 | 659 ± 174.35 |
| 4 | 773 ± 147.20 |
| 5 | 809 ± 199.68 |
| 6 | 537 ± 174.09 |
| 7 | 754 ± 170.74 |
| 8 | 832 ± 169.73 |
| 9 | 765 ± 173.95 |
| 10 | 815 ± 235.78 |
| 11 | 722 ± 222.26 |
| 12 | 730 ± 178.78 |
| 13 | 605 ± 226.76 |
| 14 | 693 ± 162.22 |
| 15 | 699 ± 158.18 |
| 16 | 718 ± 245.27 |
| 17 | 710 ± 325.80 |
| 18 | 821 ± 276.18 |
| 19 | 710 ± 209.56 |
The mean bone density of the existing alveolar bone below the grafted region for each subject revealed the density values in the range of 200 HU to 500 HU. The highest mean bone density was 421±81.86 HU whereas the lowest bone density was 261±83.51 HU represented in [Table/Fig-3].
Mean bone density of the existing alveolar bone below the grafted region for each subject in Hounsfield Unit (HU)
| Patient | Mean (HU) SD |
|---|
| 1 | 305 ± 94.42 |
| 2 | 304 ± 111.36 |
| 3 | 412 ± 47.65 |
| 4 | 375 ± 53.82 |
| 5 | 421 ± 81.86 |
| 6 | 264 ± 98.11 |
| 7 | 261 ± 83.51 |
| 8 | 309 ± 93.59 |
| 9 | 340 ± 70.68 |
| 10 | 292 ± 96.34 |
| 11 | 364 ± 62.27 |
| 12 | 350 ± 78.29 |
| 13 | 306 ± 70.87 |
| 14 | 307 ± 54.27 |
| 15 | 357 ± 61.24 |
| 16 | 294 ± 104.07 |
| 17 | 344 ± 74.65 |
| 18 | 265 ± 77.29 |
| 19 | 398 ± 76.17 |
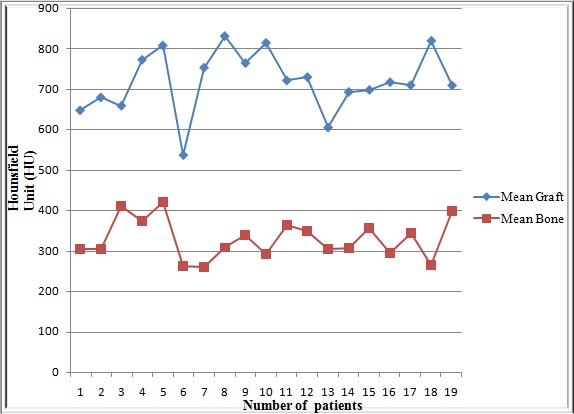
A highly significant (p value <0.05) increase in bone density at the site of grated sinus compared to the density of the alveolar bone already present underneath the grafted site. Results are summarized in [Table/Fig-4] and graphically represented in [Table/Fig-5].
Comparison of bone density at the site of the graft and of the underlying alveolar bone *significant at p-value < 0.05
| Site of bone | n | Mean (HU) ± SD | t | p-value |
|---|
| Mean density of grafted region | 19 | 720 ± 76.22 | 41.202 | 0.001 |
| Mean density of existing alveolar bone | 19 | 330 ± 49.03 | 29.363 |
Graphic representation showing comparison of mean bone density at the site of the graft and the underlying alveolar bone in each of the 19 subjects
Discussion
Today in modern dentistry there exist various bone grafting materials that offer the platform of bone regeneration prior to, during and after implant therapy.
The bone substitute that was used for our study is the an-organic bovine bone. Various authors have reported the material to be suitable for sinus augmentation [12,13]. The most commonly used product that has been reported in literature comes under the proprietary name of Bio-Oss® (Geistlich Pharma Switzerland) which is considered to be a highly biocompatible and osteoconductive material which leads to appropriate osseointegration of dental implants [14].Mainly studies on the an-organic bovine bone graft have focused primarily on histomorphometric analysis of biopsy specimens [15,16] where as we carried out a radiological density measurement study.
Our bone density values at the site of the an-organic bovine bone graft for all 19 subjects fell between 600 and less than 900 Hounsfield units. Hounsfield value for alveolar bone in the human jaw ranges from >0 and 850> Hounsfield [17,18]. The bone formation was consistent regardless of gender, age, age group or the diameter of the implant the graft was placed around.
This finding is consistent and can be correlated with histomorphometric findings that an-organic bovine bone graft is a bone forming grafting material. This finding of bone formation has been reported in both animal and human studies.
A study by Palma et al., [19] demonstrated histological evidence that there is formation of new bone in grafted sinuses of monkeys. A similar study Xu et al., [20], found that after two weeks post grafting with an-organic bovine bone mineral, the augmented space was almost completely obliterated by both newly formed bone and fibrous cancellous tissue in the sinus of rabbits. Two studies carried out on dogs similarly reported that an-organic bovine bone graft is responsible for new bone formation [21,22]. Our report of an-organic bovine bone graft as a bone forming material is consistent with numerous human histological studies as well. The new-bone generated is 100% based on the osteoconductive properties of the grafted materials, as reported by [23] who have conducted a comparative study using an-organic bone matrix material and a synthetic β-Tricalcium phosphate.
We have related and confirmed our radiological findings with the histological reports on the bone forming potential of an-organic bovine bone graft.
Our region of interest, posterior maxilla houses the poorest bone quality in the human jaw. In previous studies the mean HU bone density in the four jaw regions decreased in the following order: anterior mandible, anterior maxilla, posterior mandible, and posterior maxilla [8,24].
In our study, the recorded bone density values 330 ±49HU, which is slightly lower than the bone density reported in a study by Norton and Gamble 2001 [17]. They observed that the mean bone density values in the anterior mandible, the posterior mandible, the anterior maxilla and the posterior maxilla were 970 HU, 669 HU, 696 HU and 417 HU, respectively. This may be contributed to the fact that their research was conducted on a different set of population, as their study was carried out in the United Kingdom.
Although, our the recorded bone density is similar to that of a study carried out by Fuh et al., [25]. Carried out in an Asian population. Although, the sample size was larger than what is in our study [19], the recorded density values in the posterior maxillary area were 332 ± 136.
Conclusion
Our results suggest that an-organic bovine bone graft is a viable osteoconductive grafting material when used for the procedure of maxillary sinus augmentation and Cone beam Computed Tomography may be a useful tool for determining the invivo bone density. Furthermore, a significantly stronger bone quality was seen at the augmented site that houses the dental implants leading to increased implant stability.